Kudesan q10 tablets with potassium and magnesium 40 pcs. Vneshtorg pharma
pharmachologic effect
Cardiotonic drug of non-glycoside structure.
Composition and release form Kudesan q10 tablets with potassium and magnesium 40 pcs. Vneshtorg pharma
1 ml of drops contains ubidecarenone 30 mg, as well as additional substances: ascorbyl palmitate, tocopherol acetate, citric acid, cremophor, sodium benzoate, water.
The children's drug in 1 tablet contains 7.5 mg of ubidecarenone. As additional substances: dextrose monohydrate, silicon dioxide, povidone, magnesium stearate, talc, creamy flavor.
Tablets for adults Kudesan Forte consist of 30 mg of ubiquinone and 4.5 mg of tocopherol acetate. Additional substances: colidon, aerosil, calcium stearate, primelose, microcrystalline cellulose.
Kudesan Forte in the form of a 1 ml solution contains 60 mg of coenzyme Q10 and 6.8 mg of tocopherol.
Kudesan with magnesium and potassium in 1 tablet includes: 7.5 mg of ubiquinone, potassium - 97 mg (in the form of potassium aspartate 450 mg), magnesium - 16 mg (in the form of magnesium aspartate 250 mg).
Kudesan Forte per 1 ml contains twice as much ubidecarenone and additionally contains tocopherol acetate.
Kudesan and Kudesan Forte drops for oral administration in 20 ml bottles.
Chewable tablets for children in contour packages of 30 pcs.
Kudesan Forte tablets, 20 pcs. packaged.
Kudesan with magnesium and potassium 40 pcs. packaged.
Characteristic
Coenzyme Q10, potassium and magnesium are required by the heart to function.
The main function of the heart is to ensure the movement of blood in the body through constant contractions. They, in turn, occur due to physical processes and biochemical reactions continuously occurring in the heart, which require significant energy expenditure.
Potassium and magnesium are essential participants, and the energy supply to the heart depends on coenzyme Q10.
With various diseases, emotional stress, intense physical work, as well as with the development of a number of age-related diseases, the load on the heart increases. Therefore, it requires more energy and nutrients.
“Cardio Potassium and Magnesium tablets” of the “Kudesan” trademark supplies the heart with the substances necessary for its full functioning throughout life.
Directions for use and doses
Adults: 2 tablets 2 times a day with meals.
Duration of treatment: 1 month.
Pharmacodynamics
Ubidecarenone (coenzyme Q10, ubiquinone) is a natural substance that is a vitamin-like coenzyme. Ubidecarenone is an endogenous substrate that takes part in the transfer of electrons in the transport chain of redox processes, in the process of energy exchange, and in the reaction of oxidative phosphorylation in the respiratory chain of cell mitochondria. Participates in the processes of cellular respiration, increasing the synthesis of adenosine triphosphoric acid (ATP). Has a clinically significant antioxidant effect. Protects cell membrane lipids from peroxidation. Reduces the area of myocardial damage under conditions of ischemia and reperfusion. Ubidecarenone prevents QT interval prolongation and improves exercise tolerance. Due to endogenous synthesis, 100% satisfaction of the body's need for coenzyme Q10 occurs only until the age of 20. Endogenous synthesis of coenzyme Q10 is reduced in various diseases in both adults and children, as well as in the elderly.
Indications for use Kudesan q10 tablets with potassium and magnesium 40 pcs. Vneshtorg pharma
The drug is used as part of complex treatment and for prevention.
In adults:
- cardiomyopathy;
- heart failure;
- arrhythmias;
- myocardial infarction during the recovery period;
- cardiac ischemia;
- arterial hypertension;
- preparation for aorto-coronary bypass surgery and other surgical interventions on the heart.
Instructions for use of Kudesan for children determine the possibility of taking it for the following diseases:
- heart disease (cardiomyopathy, heart failure, arrhythmias);
- preparation for operations for congenital and acquired defects;
- kidney diseases (metabolic nephropathy, chronic pyelonephritis);
- diseases of the nervous system (vegetative-vascular dysfunction, hereditary neurodegenerative diseases, muscular dystrophies, congenital myopathies);
- chronic gastroduodenitis;
- recovery period after operations and serious illnesses;
- asthenic syndrome.
In children and adults, the drug is used to increase adaptation to increased physical activity and to compensate for the lack of coenzyme Q10 in the body.
Contraindications
individual intolerance; children under 1 year old.
If you have low blood pressure, use it with caution.
Application of Kudesan q10 tablets with potassium and magnesium 40 pcs. Vneshtorg pharma during pregnancy and breastfeeding
The drug is not recommended for pregnant and lactating women due to the lack of sufficient experience in clinical use.
special instructions
Impact on the ability to drive vehicles and operate machinery
The effect of the drug "Kudesan® for children" on the ability to drive vehicles and operate machinery has not been studied.
Overdose
Cases of drug overdose have not been described.
Side effects Kudesan q10 tablets with potassium and magnesium 40 pcs. Vneshtorg pharma
Allergic reactions are possible. Very rare: nausea, diarrhea.
Drug interactions
The simultaneous use of lipid-lowering drugs (statins, fibrates), beta-blockers (atenolol, metoprolol, propranolol), tricyclic antidepressants can lead to a decrease in the concentration of ubidecarenone in the blood plasma. Ubidecarenone may reduce the effect of warfarin.
Ubidecarenone can potentiate the effect of nitrates and enhance the antihypertensive effect of diltiazem and metoprolol.
Kudesan is a complex antioxidant in the treatment of cardiovascular diseases
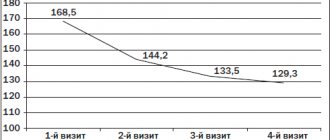
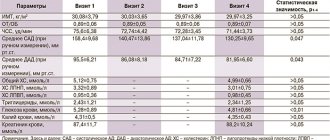
The development of modern society, the introduction of high technologies in the social and industrial sphere of human activity is accompanied by an intensification of the functioning of various organs and systems of our body. The intense rhythm in social and industrial activity is a kind of acute and chronic stress with the active consumption of biological components involved in the functioning, restoration of the structure and function of cells of various organs (cardiovascular system, central nervous system, etc.). Modern advances in the study of cell function (in particular, endothelium) of various organs indicate the leading role of oxidative stress - excessive formation of reactive oxygen species (ROS - O2-), in the formation of cardiovascular diseases (CVD), through lipid peroxidation (LPO) cell membrane. ROS – O2–, which have an unpaired electron, have directly opposite biological effects depending on the concentration: at normal concentrations – regulatory, at excess concentrations – toxic effects. [1,3,8,13]. The main source of ROS in cells is mitochondria (Mx), during the normal functioning of which 98% of the incoming oxygen is used for the oxidation of substrates with the formation of ATP (the main energy substrate of cells) and 2% for the synthesis of ROS, which can increase significantly in various pathological conditions (Fig. . 1). Currently, three forms of ROS are distinguished: primary, secondary and tertiary (Fig. 2) [3]. Primary ROS – nitric oxide (NO) and superoxide (O2–) have regulatory functions: NO – has a vasodilatory effect, O2– – with the help of the enzyme superoxide dismutase, is successively converted into hydrogen peroxide (H2O2) and hypochloride (ClO–), which are used by macrophages for fight against bacteria (regulation of immune status). Secondary ROS – hydroxyl and lipoxyl radicals (OH– and LO–), are formed from primary forms of ROS through their interaction with excess superoxide and the formation of ferrous iron from ferric iron (Fe3+ҐFe2+). It is this category of ROS that has a strong toxic effect on cell membrane lipids, DNA molecules, carbohydrates and proteins. Tertiary ROS are formed when secondary ROS are neutralized by antioxidant molecules, and their role can be varied. The proposed mechanism of action of oxidative stress on the vascular bed is mediated through blocking the availability of NO (the main regulator of endothelial function) to the tissues of the vascular wall. The bioavailability of NO depends to a certain extent on its interaction with reactive oxygen radicals – O2–. O2– inactivates NO in vivo with impaired vascular function in various pathophysiological situations. The “side” branch of the use of O2 (oxidative system), due to its potential danger to cellular structures, in the process of evolution contributed to the formation of a protective system of antioxidants, which is represented by enzymes and low-molecular compounds, and, depending on its location, is divided into lipophilic and hydrophilic antioxidants. Antioxidants either directly bind free radicals (direct antioxidants) or stimulate the tissue antioxidant system (indirect antioxidants). The first link of antioxidant “protection” is the hydrophilic compounds of superoxide dismutase (SOD), which converts the superoxide anion (O2–) into the electrically neutral form of H2O2 (hydrogen peroxide), followed by its removal from the cell through cleavage to O2 and H2O by two enzymes: catalase and glutathione peroxidase ( Fig. 3). Peroxidation is based on a chain reaction of destruction of unsaturated fatty acids that make up the phospholipids of cell membranes. Therefore, cell membranes have their own lipophilic antioxidants: Coenzyme Q10 and a-tocopherol (vitamin E). Coenzyme Q10 is central to the antioxidant system. The second official name for coenzyme Q10 is ubiquinone (“ubiquitous quinone”), since it is found in varying concentrations in almost all tissues of animal origin, and its content in the myocardium is much higher than in all other tissues of various organs. With age, the content of ubiquinone in the myocardium decreases by 1.5–2 times, which significantly reduces the protective role of the antioxidant system. Coenzyme Q10, a vitamin-like substance, was first isolated from bovine heart mitochondria by the American scientist F. Crane in 1957, and in 1958 K. Folkers determined its structure. In the 60s, the role of coenzyme Q10 was shown as an electron carrier in the respiratory chain of mitochondria - a “factory” of energy substrates (ATP) for cell life. In 1978, P. Mitchell proposed a scheme explaining the participation of coenzyme Q10, both in electron transport in mitochondria and in the coupling of the processes of electron transport and oxidative phosphorylation, for which he received the Nobel Prize. Coenzyme Q10 effectively protects the lipids of biological membranes and lipoprotein blood particles (phospholipids (“membrane glue”) from the destructive processes of peroxidation, protects DNA and body proteins from oxidative modification by reactive oxygen species (ROS). The synthesis of coenzyme Q10 in the body is carried out from the amino acid tyrosine with the participation of vitamins B2, B3, B6, B12, C, folic and pantothenic acids, and a number of microelements. With age, the biosynthesis of coenzyme Q10 progressively decreases, and its consumption increases during physical, emotional stress and oxidative stress in the pathogenesis of various cardiovascular diseases [3]. The uniqueness of the substance under discussion lies in its ability to regenerate (reproduce) under the action of the body’s enzyme systems, which distinguishes coenzyme Q10 from other antioxidants (vitamins E, A, C, b-carotene), which, while performing their function, irreversibly oxidize themselves, requiring additional administration . The metabolism of ubiquinone is closely related to the metabolism of another lipophilic antioxidant, vitamin E, which is the most effective antioxidant in the myocardium. Ubiquinone is able to regenerate the reduced form of vitamin E. At the same time, the concentration of vitamin E in plasma increases several times. The concentration of ubiquinone in tissue cells is much higher than that of vitamin E, and in plasma the opposite ratios occur. Vitamin E belongs to the group of a-tocopherols, can improve immune status (especially in older people), reduce the risk of developing atherosclerosis - a risk factor for coronary artery disease and its complications, which indirectly indicates its usefulness in improving the quality and prolonging life. The ability of a-tocopherols to inhibit the peroxidation of low-density lipoproteins (LDL) suggests its effectiveness in the prevention of coronary artery disease through the suppression of atherogenesis, which is confirmed by data from 4 multicenter clinical studies on the possible preventive effect of vitamin E on the development of CVD [1,3,9]. The damaging effect of ROS at the cellular level in clinical practice is classically illustrated during the development of AMI. Restoration of coronary blood flow in the area of myocardial ischemia is accompanied by a “surging” supply of O2 into cardiomyocyte cells. During ischemia, the O2 concentration in the cardiomyocyte drops sharply, with a simultaneous increase in xanthine oxidase activity and the transition of oxidized Fe3+ atoms to Fe2+. Both of these processes, with an increase in the partial pressure of O2 in the cytoplasm, sharply activate the formation of OH- and damage to intracellular structures with possible cell death (apoptosis). Similar mechanisms of dysfunction and damage to the vascular endothelium can be traced in hypertension and the development of atherosclerosis [9]. More than 25 years of experience in clinical studies of the use of coenzyme Q10 in thousands of patients convincingly proves the role of its deficiency in the development of pathological processes in the cardiovascular system, which is not surprising, since it is in the cells of the heart muscle that the energy needs are greatest. The protective role of coenzyme Q10 is due to its participation in the processes of energy metabolism of the cardiomyocyte and its antioxidant properties. Clinical studies in recent decades have shown the therapeutic effectiveness of coenzyme Q10 in the complex treatment of coronary artery disease, arterial hypertension, atherosclerosis and chronic fatigue syndrome. The accumulated clinical experience allows us to recommend the use of Q10 not only as an effective drug in the complex treatment of CV diseases, but also as a means of preventing them. Recommended doses of coenzyme Q10 in the prevention of CVD for adults are 15 mg daily, therapeutic doses are 30–150 mg/day, and in cases of intensive care up to 300 mg/day. [4,6]. The first positive clinical experience in cardiology with the use of coenzyme Q10 was accumulated by Japanese researchers in the treatment of patients with dilated cardiomyopathy (DCM) and mitral valve prolapse (MVP): convincing data were obtained on the improvement of diastolic myocardial function. The diastolic function of cardiomyocytes and smooth muscle cells of other organs (lungs, gastrointestinal tract) and systems (vessels, muscular skeleton) is an energy-intensive process, and under various pathological conditions the cardiovascular system consumes up to 50% or more of the total energy contained in ATP synthesized in cells , which determines its strong dependence on the level of intracellular concentration of coenzyme Q10 [3,4,11]. Clinical experience with the use of ubiquinone in children with chronic tachyarrhythmias, sick sinus syndrome and long QT interval, as well as cardiomyopathies, has shown that in most children there are pronounced positive dynamics in the form of normalization or significant improvement of repolarization processes in the ST segment of the ECG [10]. The results of clinical studies, summarized in reviews, indicate that the content of ubiquinone in plasma is reduced in hyperlipidemia, after statin therapy, and its addition to traditional therapy reduces plasma oxidation [9]. At the same time, the feasibility of using a complex of antioxidants contained in natural products in the prevention of CVD has been postulated. One of the representatives of antioxidants is Kudesan (a product made from the oil of red palm fruits), and not individual components of antioxidants presented in tablet preparations [5,7,11,13]. Currently, the water-soluble antioxidant Kudesan has been created and introduced into clinical practice in Russia. which promotes faster and more efficient absorption of antioxidant components in the gastrointestinal tract in the treatment of patients with CVD (Fig. 4) [12]. Kudesan is a complex antioxidant, 1 ml of which contains 30 mg of coenzyme Q10 and 4.5 mg of vitamin E. In our observations of patients with AMI (127 patients) who received thrombolytic therapy (up to 6 hours from the onset of pain), 42 patients thrombolytic therapy, Kudesan was added at a dose of 50 ml per day for 2-3 days, which in total corresponded to taking 1500 mg of coenzyme Q10 and 225 mg of vitamin E per day. In the study group, “reperfusion” syndrome (cardiac rhythm disturbances - ventricular extrasystoles, the appearance of chest pain, progression of heart failure, reduction of the ST segment and prolongation of the QT interval on the ECG), which required additional treatment, was registered only in 16.6%, while as in the control group (standard therapy for AMI against the background of thrombolysis) – in 23.3% of cases (Fig. 5). At the same time, under our supervision there were 38 patients with CHF (atherosclerotic and post-infarction cardiosclerosis) with signs of dilatation of the left heart, to whom Kudesan 5 ml per day (150 mg - ubiquinone, 22.5 mg - vitamin E) was added to the standard treatment of heart failure. As a control group, 26 patients with a similar pathology were selected, in whom Kudesan was not included in the heart failure treatment program. The age of patients in the study and control groups was not statistically different and, respectively, was 58.7±4.1 years and 60.2±3.7 years (p>0.05). At the first stage, treatment of CHF was carried out while taking ACE inhibitors, b-blockers, cardiac glycosides with the use of potassium-sparing diuretics. All patients before and after treatment underwent an echocardiography study to assess the pumping activity of the heart (cardiac ejection fraction - EF%), end-diastolic volume (LVEDV) and left ventricular end-systolic volume (LVESV). The degree of CHF was assessed according to the classification of the Russian Scientific Society of Heart Failure (2001), the functional class of CHF was assessed according to the NYHA classification and a stress test - the number of meters of a 6-minute walk without shortness of breath [2]. The results of the examination before and after treatment are presented in Table 1. As can be seen from the table, indicators of central hemodynamics and exercise tolerance before treatment in the study and control groups were not statistically different from each other and corresponded to FC III–IV of HF. Before treatment, all patients in the study and control groups had stage IIB HF: in the study group, 71.05% had FC III HF, 28.95% had FC IV HF; in the control group, FC III HF was registered in 76.9%, FC IV HF – 23.1%. The average values of ejection fraction and exercise tolerance in general for the groups did not differ statistically from each other and, accordingly, were: in the study group - 44.6 ± 3.8%, 242.3 ± 38.1 meters; in the control group – 45.2±4.1%, 261.1±42.3 meters (p>05). After the treatment (after 3 weeks), a statistically significant more pronounced improvement in the pumping activity of the heart was noted in the study group of patients with CHF compared to the control group of patients. Thus, in the study group, where Kudesan was added to the standard therapy for CHF (5 ml per day - 150 mg of coenzyme Q10 and 22.5 mg of vitamin E), EF in the group as a whole increased by 16.8% (from 44.6± 3.8% – to 52.1±3.2%, p<0.01), exercise tolerance increased by 62.7% (from 242.3±38.1 – to 394.3±35.2 meters in 6 minutes, p<0.001). In the control group, there was a statistically insignificant increase in similar indicators: EF increased by only 9.7%, exercise tolerance increased by 23.9% (p>0.05). In general, LDL in the study group decreased statistically significantly by 8.8% (from 102.8±3.7 ml to 93.8±3.9 ml, p<0.05), while in the control group LDL statistically insignificantly decreased by only 3.5% (from 104.0±4.1 ml - to 100.4±3.8 ml, p>0.05). LSV in the study group also decreased after treatment by 19.3% (from 57.0±2.4 ml to 46.1±2.3 ml, p<0.01), in the control group the same indicator decreased statistically significantly only by 9.5% (from 57.1±2.9 ml to 51.7±2.4 ml, p<0.05). After treatment, such positive dynamics of indicators that determine the efficiency of the pumping activity of the heart made it possible in the study group to more effectively stop the clinical signs of HF and improve the functional class: in the study group of patients with CHF, class I HF was achieved in 55.3% of cases and in 44.7% – II FC HF, while in the control group FC I HF was registered in 46.2%, II FC HF – in 53.8% of cases (Fig. 6). Thus, the addition of water-soluble Kudesan (50 ml per day) and therapy for CHF (5 ml per day) to standard therapy for AMI has a significant positive therapeutic effect, manifested by a decrease in the number of cases of the development of “reperfusion” syndrome during thrombolytic therapy for AMI by 6.7% and achieving a more favorable FC of CHF in the treatment of CHF. Similar results on the use of water-soluble coenzyme Q10 in the treatment of AMI and CHF are presented in clinical studies by other authors [1,4,6,12,13]. One of the problems of modern treatment tactics for AMI (thrombolytic therapy) is myocardial damage during restoration of blood flow in the infarct-dependent coronary artery (reperfusion syndrome) [1,6,8]. In case of AMI, one of the possible mechanisms of the positive effect of coenzyme Q10 has been identified - prevention of the development of the long QT interval syndrome on the ECG (a component of the “reperfusion” syndrome), which is associated with a higher frequency of sudden cardiac death. In the control group of patients with AMI - 29 patients (6 hours from the onset of pain) - with standard therapy, 40% observed an extension of the QT interval > 440 ms; in a similar group of patients with AMI, with the addition of coenzyme Q10 at a dose of 100 mg per day, there was no prolongation of the QT interval observed. At the same time, it was noted that the use of coenzyme Q10 in patients with acute coronary syndrome significantly reduces the level of LDL cholesterol and increases the level of HDL cholesterol [1,12,13]. The protective role of coenzyme Q10 under conditions of ischemia and reperfusion has been convincingly proven in experiments on rats using fat- and water-soluble forms of the drug. Mitochondria isolated from the hearts of rats treated with ubiquinone were distinguished by better structural preservation and the level of oxidative phosphorylation. The rate of succinate-dependent generation of superoxide radicals in mitochondria from the hearts of rats receiving the hydrophilic form of coenzyme Q10 (35±8 nmol O2/min per 1 g of protein) was two times lower than in the control group (74±12 nmol O2/min per 1 g of protein) [3,4,5,6]. Given the main purpose of the Q10 Coenzym - ensuring sufficient energy formation of ATP for the normal functioning of the cardiomyocyte - it can be assumed that its use is useful in the treatment of heart failure of various etiologies, including dilatation cardiomyopathy. It was found that with heart failure there is a reliable correlation with the low level of Coenzyme Q10 and the severity of CH. In meta -analysis, including 13 double blind randomized studies using Coenzyme Q10, only 3 (10% of 1000 treated patients) obtained neutral results. In all the rest, reliable evidence has been obtained: a - improvement of the functional class of patients, b - increase tolerance to physical activity, c - reducing the frequency of repeated hospitalization [1.13]. Another randomized double blind study included 319 patients with CHAI - IV FC (against the background of ordinary treatment, Coenzyme Q10 was prescribed at a dose of 2 mg/kg during the year) and 322 patients with KHS without adding coenzyme Q10. After one year, in the study group of patients with heart failure, re -hospitalization was required in 73 cases, in the control - 118 patients (p <0.001), cardiac asthma took place in 97 patients against 198 patients of the control group (p <0.001), and swelling of the lung developed in 20 against 20 against 50 patients of the control group (p <0.001) [1,11,13]. The results allowed the authors to come to the conclusion - the addition of Coenzyme Q10 in the treatment of patients with heart failure of severe classes significantly improves the course of the disease, with a decrease in the need for repeated hospitals and the prevention of clinical complications. The greatest difficulties occur in the treatment of CH in patients with dilatation cardiomyopathy. In the treatment of 137 patients with cardiomyopathy for 3 months (standard therapy + Coenzyme Q10 150 150 mg per day) having the initial FV 25 ± 10.3%, the content of Q10 coenzyme in blood plasma increased by 170.6% with a simultaneous increase in FV to 41 , 6 ± 14.3% (p <0.001). At the same time, in patients with low FV, survival in 36 months amounted to 75% [1.12]. A number of works show the high efficiency of Q10 coenzyme in a dose of 200 mg per day in the treatment of diastolic dysfunction in patients with hypertension: a regression of hypertrophy of the left ventricle was noted in 53% of observations with a decrease in blood pressure in 85% of observations [11]. Thus, summarizing our results and literature data, the use of water -soluble Kudesian (Coenzima Q10 - Kilikhinon and Vitamin E) - a natural comprehensive antioxidant in the complex therapy of SSZ, contributes to a more effective restoration of the pumping of the heart, which underlies the development of CH of various etiology. The optimal dosage of Coenzyme Q10 in the treatment of chronic forms of SVD is 2 mg per 1 kg of patient weight, in acute coronary syndrome (in particular, with OMA) to prevent the development of “reperfusion” syndrome, higher doses of the drug are possible - up to 1500 mg per day. The expected effects of treatment are manifested after 1 month from the start of taking the drug, the maximum of the therapeutic effect is expected with a treatment period of up to 6 months. In addition, the water -soluble kudsian (a pharmaceutical company Aquion) is a safe drug: not a single severe side effect or sudden heart death is described with the use of Coenzyme Q10.
Literature 1. Aronov D.M. Application of coenzyme Q10 in cardiological practice. RMJ. 2004, T 12, No. 15, 905 – 909; 2. Belenkov Yu.N. Classification of chronic heart failure. Heart failure. 2001, T. 2, No. 6, 249 – 250; 3. Kapelko V.I. Reactive oxygen species, antioxidants and heart disease prevention. RMJ. 2003, T.11, No. 21, 1185 – 1188; 4. Kapelko V.I. Ruuge E.K. Study of the effect of coenzyme Q10 (Ubiquinone) in cardiac ischemia and reperfusion. The use of the antioxidant drug kudesan (coenzyme Q10 with vitamin E) in cardiology. Moscow. 2002; 5. Korovina N.A., Ruuge E.K. The use of coenzyme Q10 in prevention and treatment. The use of the antioxidant drug kudesan (coenzyme Q10 with vitamin E) in cardiology. Moscow. 2002; 6. Lakomkin V.L., Korkina O.V. et al. Protective effect of ubiquinone (coenzyme Q10) in cardiac ischemia and reperfusion. Cardiology. 2002, 12, 51 – 55; 7. Lankin V.Z., Tikhaze A.K., Belenkov Yu.N. Free radical processes in diseases of the cardiovascular system. Cardiology. 2000, 40 (7), 48 – 61; 8. Lankin V.Z., Tikhaze A.K., Belenkov Yu.N. Antioxidants in complex therapy of atherosclerosis: pro et contra. Cardiology 2004, 2, 72 – 81; 9. Lankin V.Z., Tikhaze A.K., Belenkov Yu.N. Antioxidants in complex therapy of atherosclerosis: pro et contra. A manual for doctors. Moscow. 2006; 10. Shkolnikova M.A. Report of the Association of Pediatric Cardiologists of Russia on the use of kudesan. The use of the antioxidant drug kudesan (coenzyme Q10 with vitamin E) in cardiology. Moscow. 2002; 11. Bayrh VA, Abukhalaf IK, Ganafa AA Effect of palm oil on blood pressure, endothelial function and oxidative stress. PIPOC. 2003. International Palm Oil Congress. Food Technology and Nutrition Conference. 24 – 28 August. 2003, 280 – 283; 12. Chopra PK, Goldman R. Int. J. Vit. Nutr.Res. 1998, 68(2), 109 – 113; 13. Langsjoen PH, Langsjoen AM Overview of the CoQ10 in cardiovascular disease. BioFactors. 1999, 9, 273 – 284.
Kudesan forte solution 20ml (dietary supplement) (Rusfik)
There is such a form of the drug as Kudesan forte. It is available in the form of drops and tablets. According to the instructions, it can be used in adults and children over 14 years of age. The main difference is the increased content of coenzyme Q 10. Due to the higher concentration of the active substance, fewer drops are required per dose, which is much more profitable than using a 3% solution. The main active ingredient of Kudesan is coenzyme Q10, which is used in the prevention and composition of complex therapy: cardiovascular failure, atherosclerosis, coronary heart disease, arterial hypertension; chronic fatigue syndrome; The main active ingredients - coenzyme Q 10 and vitamin E - are necessary components for protecting cellular structures from adverse environmental influences. When used together, the effectiveness of these substances is highest. Functions of Q10 in the body If you have purchased a product containing Q10 for the first time, you will benefit from additional information about this substance. The scientific research that discovered the biological role of coenzyme Q10 was one of the largest achievements in the field of human biochemistry and was awarded the Nobel Prize. Due to its high efficiency, Q10 has become widely known, especially in cardiology. Coenzyme Q10 is a substance natural to the body. It is produced and present in all cells of the body. Causes and consequences of Q10 deficiency If the synthesis of Q10 in the body decreases, energy production and the preservation of cellular structures are disrupted. As a result, fatigue appears, activity decreases, heart function is disrupted, immunity weakens, etc. Q10 deficiency and a decrease in its synthesis can occur due to various diseases, medications, and heavy physical and mental stress. Its causes may be age-related disorders, metabolic failures, etc. You should also know that, starting from the age of 20, regardless of health and lifestyle, the synthesis of Q10 in the human body begins to decline. How to eliminate Q10 deficiency It is almost impossible to compensate for the Q10 deficiency by increasing its intake from food, because the Q10 content in most foods is low. So, in order to deliver the required amount of Q10 to the body per day, you need to eat at least 800 g of beef or 1 kg of peanuts. In order to eliminate Q10 deficiency and normalize its natural synthesis in the body, additional intake of Q10 is recommended. The natural origin and presence of Q10 in all cells determine the safety of its preparations. The possibility of overdoses, side effects and negative drug interactions is minimized. Efficiency of use The effectiveness of Q10 preparations depends on the form of release. Q10 is a fat-soluble substance (that is, it is absorbed only with fat). Most Q10-based drugs have to be taken with fatty foods, which is not very beneficial. Domestic specialists have developed and patented a technology that has made it possible to convert the poorly digestible fat-soluble substance Q10 into a water-soluble form that is optimal for absorption and easy to use. This technology is used in the production of Kudesan series drugs. Information for specialists Coenzyme Q10 is a vitamin-like compound present in all tissues of the human body. Most Q10 is found in the heart. The main function of Q10 is to couple oxidative phosphorylation reactions in the mitochondrial respiratory chain. Without Q10, insufficient ATP is produced. The second function of Q10 is to quench free radicals and restore the activity of other antioxidants. Q10 is synthesized endogenously, but from age 20, Q10 biosynthesis progressively decreases. In the myocardium, by the age of 50, Q10 deficiency reaches 40% and deepens with age. With a deficiency of Q10, negative changes occur in the cardiovascular system: myocardial contractility decreases, the risk of atherosclerosis, coronary heart disease, myocardial infarction, etc. increases. The effectiveness of Q10 in complex therapy and prevention of these diseases, as well as for slowing down processes associated with aging, has been established. . Coenzyme Q10 is recommended in complex therapy: with GM-CoA reductase inhibitors (statins) to level out side effects (such as myalgia, peripheral neuropathies); diseases caused by mitochondrial dysfunction (myopathies, asthenia); heart rhythm disturbances, vegetative dystonia, chronic gastroduodenitis, chronic pyelonephritis, nephropathy in pediatric practice. And also in case of malnutrition, growth retardation, during the period of convalescence after serious illnesses and surgical interventions. Coenzyme Q10 can be recommended for the prevention of chronic fatigue syndrome and asthenic syndrome. Water-soluble form of Q10 – ensures the most complete absorption. Prescribed doses of Q10: 30 to 150 mg/day. The recommended duration and frequency of use of Q10 is 2 months, 2 times a year.