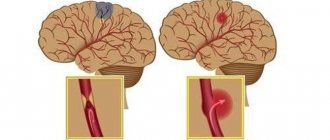
Cerebral infarction or ischemic stroke are both names for a stroke caused by a blockage of a blood vessel in a person's brain.
This is the most common type of stroke among Russians, Ukrainians and Belarusians. A blood clot or fatty plaque forms in the patient's brain and blocks a blood vessel - an embolus.
This is focal necrosis of the brain caused by complete and prolonged ischemia, which affects all tissue elements, neurons, glia and blood vessels.
Ischemic infarctions cause focal neurological deficits in the patient. With embolic infarctions they appear abruptly. In atherothrombotic infarctions, they develop over a period of time, usually several hours. Atherothrombotic infarctions are often preceded by transient ischemic attacks (TIAs).
A TIA is a focal neurological deficit that lasts less than 24 hours and resolves.
Causes of cerebral infarction:
A cerebral infarction (stroke) is mainly caused by a blocked artery (ischemic stroke) or a ruptured blood vessel (hemorrhagic stroke). Our specialists see categories of patients who may experience only a temporary disruption of blood flow to the brain (transient ischemic attack or TIA), which does not cause permanent damage to the brain.
Types of ischemic stroke include:
Approximately 70% of strokes are ischemic strokes. Ischemic strokes occur when arteries to a patient's brain become narrowed or blocked, causing severely reduced blood flow (ischemia). The most well-known ischemic strokes include:
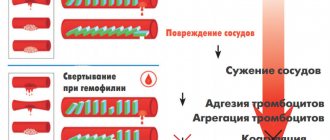
- Thrombotic stroke. A thrombotic stroke occurs when a blood clot (thrombus) forms in one of the arteries that supplies blood to the brain. The clot may be caused by fatty deposits (plaques) that accumulate in the arteries and cause decreased blood flow (atherosclerosis) or other artery diseases.
- Embolic stroke. An embolic stroke occurs when a blood clot forms from your brain - usually in the heart - and travels through the bloodstream to form in narrower arteries in the brain. This type of blood clot is called an embolus.
- Hemorrhagic stroke. A hemorrhagic stroke occurs when a blood vessel in the brain leaks or ruptures. Brain hemorrhage can be the result of many conditions that affect the blood vessels.
These include:
- Uncontrolled high blood pressure – arterial hypertension;
- Weak blood vessel walls (aneurysms);
- A less common cause of hemorrhage is the rupture of an abnormal tangle of thin-walled blood vessels (arteriovenous malformation).
Types of hemorrhagic stroke include:
- Intracerebral hemorrhage. In intracerebral hemorrhage, a blood vessel in the brain bursts and spills into the surrounding brain tissue, damaging brain cells. The brain cells outside the leak are deprived of blood and are also damaged.
- High blood pressure, trauma, vascular malformations, high dose use of blood thinning medications, and other patient factors can cause intracerebral hemorrhage in the brain.
- Subarachnoid hemorrhage. In a subarachnoid hemorrhage, an artery on or near the surface of the brain bursts and enters the space between the surface of the brain and the skull. This bleeding is often signaled by a sudden, severe headache. Subarachnoid hemorrhage is usually caused by the rupture of a small sac- or berry-shaped aneurysm. After a hemorrhage, the blood vessels in your brain may widen and narrow randomly (vasospasm), causing damage to brain cells by further restricting blood flow.
- Transient ischemic attack (TIA). A transient ischemic attack (TIA)—sometimes known as a mini-stroke—is a temporary period of symptoms. A temporary reduction in blood supply to part of the brain causes Thias, which can last only three to five minutes.
Risk factor for cerebral infarction:
- The patient has an unhealthy lifestyle and constant emotional stress (work, relationships with family, financial losses, etc.);
- Overweight or obesity (often our patients are obese due to constant stress);
- Insufficient physical activity;
- Smoking, exposure to secondhand smoke and alcohol;
- Drug use;
- Blood pressure readings above 120/80 millimeters of mercury (mmHg);
- High cholesterol level in the blood (regular laboratory diagnostics of CBC, BAC, OAM);
- Diabetes;
- Cardiovascular diseases;
- Genetic predisposition;
- Age—people aged 55 years and older have a higher risk of stroke than younger people;
- Floor. Men have a higher risk of stroke than women;
- Hormones—use of birth control pills or hormone therapy that includes estrogen.
Myocardial infarction and hemorrhagic alveolitis in systemic lupus erythematosus
Despite the well-known symptoms of systemic lupus erythematosus (SLE), each case of this disease is unique. The course of the disease is characterized by periods of exacerbations and remissions that occur while taking medications. Discontinuation of treatment is usually accompanied by exacerbation of SLE at varying intervals. The disease can begin with damage to one or more organs or progress at lightning speed, ending in death in a short period of time.
The main causes of death during the first year after the onset of the disease are the activity of SLE (damage to the kidneys, central nervous system - CNS) or the addition of an infection. Subsequent deaths may be caused by cardiovascular accidents, chronic renal failure and malignant neoplasms [1]. The use of glucocorticosteroids can reduce the incidence of deaths resulting from SLE activity.
We describe a patient with SLE in whom disease activity caused the development of disseminated intravascular coagulation (thrombohemorrhagic stage) and death in the first year after the onset of SLE.
Patient K., 18 years old, was admitted to the hospital of the Institute of Rheumatology of the Russian Academy of Medical Sciences in October 2003 with complaints of hemorrhagic rashes on the skin, pain in the right elbow, wrist and metacarpophalangeal joints of the right hand, swelling of these joints, hair loss, weakness, shortness of breath with physical activity.
The onset of the disease at the end of December 2002 was characterized by the appearance of erythema on the face, the development of arthritis of the small joints of the hands, low-grade fever, and a sharp decrease in body weight (in 2 months, I lost 6 kg). In January 2003, she was hospitalized in the rheumatology department of one of the hospitals in Moscow, where changes in urinary sediment (proteinuria, erythrocyturia and leukocyturia), anemia, increased antibodies to DNA and antinuclear factor (ANF, titers unknown) were detected, which allowed diagnose SLE. From the moment of diagnosis, she constantly received prednisolone (PZ - 35 mg/day), and after consultation at the Institute of Rheumatology (April 2003) also Plaquenil (400 mg/day). Despite the therapy, changes in urine tests (trace proteinuria and microhematuria) and immunological disorders persisted, and therefore cyclophosphamide - CP (total 1.2 g) was prescribed. Stop injections of CP and reduce the dose of PZ to 20 mg/day. provoked an exacerbation of SLE: in September 2003, a hemorrhagic rash appeared on the skin of the legs, and then throughout the body, painful aphthae in the mouth, arthritis and arthralgia recurred again, fever, and weakness began to increase. An episode of severe abdominal pain, nausea, and tarry stools occurred on September 30, and a decrease in hemoglobin to 81 g/l was noted. At the place of residence, the development of food toxic infection was excluded, rehydration therapy was carried out, after which the patient was sent to the Institute of Rheumatology. A brief history diagram is presented in Fig. 1.
Prevention
Knowing your risk factors for stroke, following the advice of highly trained professionals, an annual comprehensive body check-up and a healthy lifestyle are the best steps you can take to prevent stroke. If you have had a stroke or transient ischemic attack (TIA), these steps may help prevent another stroke.
The help you receive in the clinic plays a significant role in stopping the acute period of a cerebral infarction.
The risk factors for possible complications after an attack will depend on how qualified and prompt assistance a team of neurologists, cardiologists, neurosurgeons, rehabilitation therapists and physiotherapists will provide you.
Many stroke prevention protocols are the same as cardiovascular disease prevention protocols. Basic recommendations for a healthy lifestyle include:
- Constant blood pressure monitoring. This is one of the most important things you can do to reduce your risk of stroke. If a patient has already had a stroke, lowering blood pressure may help prevent a subsequent TIA or stroke.
- Exercise, manage stress, maintain a healthy weight, and limit sodium, alcohol, and tobacco. In addition to recommending lifestyle changes, our doctor may prescribe medications to treat high blood pressure, as well as a vitamin and mineral supplement and fish oil.
- Reduce the amount of cholesterol and saturated fat in your diet. Eating less cholesterol and fat, especially saturated fat and trans fat, can reduce plaque in the arteries.
- Quitting tobacco use. Smoking increases the risk of stroke for smokers and nonsmokers exposed to secondhand smoke. Quitting tobacco use reduces the risk of stroke.
- Diabetes control.
- Maintaining a healthy weight. Excess weight contributes to the development of other risk factors for stroke, such as high blood pressure, heart disease and diabetes.
- A diet rich in fruits and vegetables. A diet containing five or more daily servings of fruits or vegetables may reduce the risk of stroke.
- Exercise can lower blood pressure. It will also help you lose weight, control diabetes and reduce stress.
Indications and contraindications for surgical treatment of stroke
Not all cases of the disease require aggressive tactics and surgical intervention. Examination by specialists and data from instrumental diagnostic methods allow an adequate assessment of the patient’s general condition.
Contraindications to surgical treatment of stroke are:
- severe concomitant diseases;
- old age over 65-70 years;
- large volume of hematoma;
- depressed consciousness - coma.
Depending on the indications, our consultants will be able to select the best specialized hospital for the victim.
Principles of disease diagnosis
The gold standard for making a diagnosis is computed tomography (CT). In the early period after an attack (1-3 days), this method of neuroimaging is more informative than MRI. Fresh hemorrhagic material, including 98% hemoglobin, appears on CT as a high-density, well-defined, bright inclusion against the background of darker brain tissue. Based on a computed tomogram, the epicenter zone, volume and shape of the formation, the level of damage to the internal capsule, the degree of dislocation of brain structures, and the state of the cerebrospinal fluid system are determined.
With the onset of the subacute phase (after 3 days), the red cells of the hematoma along the periphery are destroyed, in the center the iron-containing protein is oxidized, and the focus becomes lower in density. Therefore, along with CT scan, MRI is mandatory within 3 days and later. In subacute and chronic forms, the MR signal, in contrast to CT, better visualizes a hematoma with derivatives of hemoglobin oxidation (methemoglobin), which passes into the isodense stage. Angiographic examination methods are used in patients with an unknown cause of hemorrhagic stroke. Angiography is primarily performed on young people with normal blood pressure readings.
For adequate management of patients after an attack of intracerebral hemorrhage, an ECG and X-ray of the respiratory organs are required, and tests for electrolytes, PTT and APTT are taken.
Types of surgery
Neurosurgeons distinguish several methods by which a hematoma can be removed:
- Direct surgery. The hematoma is removed by encephalotomy, then careful hemostasis is performed. When suturing, microsurgical techniques are usually used.
- Puncture-aspiration method. Fibrinolytics are administered. This method is effective if the hemorrhage is of medium size and the patient is in a stable condition.
- Endoscopic method. Modern method of surgical treatment. During surgery, endoscopic technology is always used. Using an endoscope, they penetrate into the hematoma cavity, after which a set of specific manipulations is carried out. Surgical treatment of hemorrhagic stroke is excluded in case of unstable hemodynamics.
After surgery, the patient should remain under observation. The rehabilitation period is long and difficult, can last up to two months. Special conditions are required for the patient’s recovery (a set of procedures in a rehabilitation center).
Recovery points after hemorrhagic stroke
Complications for the patient mainly depend on the location of the hemorrhage that occurs, as well as its volume. Today there are the following groups of possible threatening consequences:
- Motor disorders. The appearance of severe weakness and paresis in a person, the patient’s inability to accept and maintain a sitting position. This may be paralysis of one side of the body, high muscle tone or spasms that occur, which seriously complicates self-care, requires mandatory assistance and causes a lot of inconvenience to the person.
- Impaired sensitivity is, for example, numbness of the limbs, a feeling of “insects under the skin” and burning, the inability to control the hands, leading to various everyday problems.
- The appearance of speech pathologies after a stroke is confusion of speech and the inability to correctly pronounce individual sounds or loss of the ability to maintain a conversation. There may be loss of skills such as recognizing the meaning of words, counting, reading, telling time by a clock, and understanding calendar periodicity.
- Problems with swallowing when eating food and various liquids, and in some cases, complete loss of the ability to eat independently.
- Disorders of the excretory system: the appearance of urinary and stool incontinence, problems with the intestines and urinary system that arise on an ongoing basis.
The patient often develops acute and chronic psychological and mental disorders in the form of depression, excessive emotional temper or apathy. Sometimes partial amnesia occurs: the inability to recognize familiar people or objects, the understanding of performing simple everyday actions disappears.