Red blood cell histograms
The erythrocytometric curves recorded using the analyzers do not correspond to the Price-Jones curves, which can be obtained through numerous and lengthy measurements of the diameter of erythrocytes under a microscope (using an ocular micrometer, the diameter of no more than 300 erythrocytes is measured in a blood smear in 4-6 hours of working time). The fact is that the diameter of erythrocytes when the smear dries decreases by 10-15%; in thick smears the diameter of erythrocytes is smaller than in thin smears and, finally, in the direction of the smear the diameter of erythrocytes is greater than across. The conductometric method reflects the volume of cells, so it is impossible to compare the distribution curves of erythrocytes by volume and diameter. The histogram of the distribution of red blood cells by volume has a number of features when compared with that by diameter:
1. The volume distribution curve is much wider; the coefficient of variation when determining volume is 3 times higher than when determining diameter.
2. The distribution curve of erythrocyte diameters is symmetrical (Gaussian curve), and the distribution of cells by volume has a shift to the right, proportional to the coefficient of variation of diameters.
3. If the diameter distribution curve is multimodal (has several peaks), then the histogram of the distribution of red blood cells by volume can be
Interpretation of the values of RDW-SD and RDW-CV indicators in the diagnosis of anisocytosis
Very often, clients of those laboratories where blood tests are carried out using automatic hematology analyzers ask for an explanation of the results of all parameters of a general blood test. The question is logical, since instead of the usual five indicators, patients receive a statement containing from 18 to 22 indicators. Product Manager Svyatoslav Polovkovich has prepared an article that will help doctors and laboratory specialists explain this issue to patients.
Blood, its functions and what are “red blood cells”
Blood is one of the important components of a living organism. It is a liquid tissue consisting of plasma and formed elements. Formed elements include platelets, erythrocytes and leukocytes.
Erythrocytes or “red blood cells” (Red Blood Cells, RBC) are non-nuclear cells that have the shape of a concave disk. The anucleate nature of red blood cells and their shape provide them with the most optimal properties in the process of gas exchange and maintaining osmotic resistance. The normal size of a red blood cell is 7.5-8.3 microns; life expectancy is 90-120 days. Red blood cells have antigenic properties, on the basis of which four main blood groups are distinguished. The cytoplasm of an erythrocyte is 96% filled with hemoglobin. In addition to mature erythrocytes, young erythrocytes—reticulocytes—can normally be found in peripheral blood. These are anucleate cells with a large amount of RNA and ribosomes that have membrane receptors for transferrin. In the reticulocyte stage, up to 30% of the total amount of hemoglobin in an erythrocyte can be produced. The other 70-80% of hemoglobin is synthesized earlier, in the pre-reticular stages of cell differentiation. The reticulocyte loses RNA and the ability to produce hemoglobin when it becomes a mature red blood cell. In the reticulocyte stage, the red blood cell resides for one day in the bone marrow and another day in the peripheral blood.
The circulatory system connects and nourishes all organs, so it is very important to monitor its condition and regularly conduct a general blood test. When performing a general blood test, you should pay attention to the size, color and shape of blood cells. By the deviation of the shape and size of cells from normal, one can judge poikilocytosis and anisocytosis.
Signal message from the hematology analyzer “Anisocytosis”: what indicators to pay attention to
Laboratory specialists often have to answer questions about interpreting hematology analyzer readings. The automatic hematology analyzer itself informs about the patient’s clinical picture. However, at meetings of laboratory technicians, the most asked questions are questions about what indicators are used to make these conclusions, and questions about the interpretation of hematology analyzer indicators. Let's try to explain these aspects using the example of interpreting the values of the RDW-SD and RDW-CV indicators in the diagnosis of anisocytosis.
Blood anisocytosis is an excess of the number of cells of non-standard size. Depending on which blood cells have changed their size, anisocytosis of erythrocytes and anisocytosis of platelets are distinguished.
Anisocytosis of red blood cells in a general blood test indicates that the size of blood particles differs from the standard. The normal size of red blood cells is 7.5-8.3 microns. The presence in the blood of a small number of red blood cells of non-standard size (compared to the total number) is allowed. On average this value is 30%. It is considered normal if 15% of blood cells have a size smaller than the standard one, and 15% of cells have a larger diameter than theirs. Red blood cells with a smaller diameter (<6.9 µm) are called microcytes. Large diameter red blood cells are divided into two groups:
- macrocytes 8 µm
- megalocytes: d>12 µm.
If the blood cells differ significantly in size from the acceptable value, a diagnosis of “Increased anisocytosis of red blood cells” will be made.
Based on the size of cells that predominate in the blood, microcytosis, mixed type and macrocytosis are distinguished. Mixed type anisocytosis occupies an intermediate position between microcytosis and macrocytosis; This type is characterized by the presence of both small and large blood cells in the blood. For example, mixed type anisocytosis with a predominance of microcytes means that the particle sizes in the blood are heterogeneous, but the majority are small in diameter particles.
To indicate the degree of heterogeneity, there is a special index - RDW (“red cell distribution width”) or erythrocyte anisocytosis index. That is, RDW demonstrates heterogeneity in the size of the red blood cell population in the sample being studied.
There are two types of indicators - RDW-CV and RDW-SD. The first, RDW-CV, shows the percentage distribution of cells by size. The second, RDW-SD, is their standard deviation, which is the difference in size between the smallest and largest red blood cells in a blood sample.
The determination of the RDW-CV index is carried out automatically by a hematology analyzer using a special formula, which takes into account the average volume of erythrocytes MCV of blood and the standard deviation from MCV. The indicator calculated in this way is usually expressed as a percentage. The RDW-CV norm is 11-15%. RDW-CV is directly related to the mean red cell volume MCV, so if most of the cells in the population are small (as in microcytosis), the RDW-CV will remain within the normal range. RDW-CV is less sensitive to the presence of small populations of microcytes, macrocytes, or reticulocytes, but better reflects overall changes in red blood cell size in macrocytic or microcytic anemia.
You can also find the RDW-SD indicator in the blood test results. This indicator is determined using a different method and does not depend on the average volume of red blood cells. The RDW-SD definition is a direct measurement of the width of the red blood cell histogram at 20% of the height of the curve; the height of the RBC histogram is taken as 100%. RDW-SD is measured in fl (femtoliters) and reflects the difference between the maximum and minimum volume of red blood cells in the test sample. Normal RDW-SD is 35-60 fl. RDW-SD is a more sensitive indicator when small numbers of macrocytes and microcytes appear in the red blood cell population, as it measures the lower part of the red blood cell volume distribution curve. Also, this indicator will change more quickly with reticulocytosis, since a broadening of the base of the erythrocyte histogram will be observed.
Clinical value of RDW value in making a diagnosis
Interpretation of the RDW value in test results is always carried out in parallel with the assessment of the mean erythrocyte volume (MCV), since quite often the width of the distribution of erythrocytes remains normal in the presence of a homogeneous cell population with microcytosis or macrocytosis.
If RDW in a blood test is elevated, the following pathological conditions can be assumed in the patient:
- Iron-deficiency anemia
- Immune hemolytic anemia
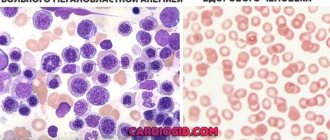
- Megaloblastic anemia (with a lack of vitamins B9 and B12)
- Hemoglobinopathy
Elevated RDW values are also common in patients with liver disease and patients who have undergone blood transfusion. In addition, the anisocytosis index may be erroneously overestimated if cold agglutinins are present in the test sample. It is also worth noting pathologies in which RDW does not change. These include: beta thalassemia, anemia in severe chronic diseases, sickle cell anemia, acute hemorrhagic and aplastic anemia, spherocytosis.
It is important that conducting research on an automatic hematology analyzer is more accurate, since the width of the distribution of red blood cells can increase even before changes in red blood cells appear, and the value of hemoglobin, that is, an increase in the anisocytosis index, can be called an early marker of anemia. It is worth noting that during the treatment of iron deficiency anemia, the RDW indicator not only does not decrease, but also increases, while the histogram changes noticeably (two peaks appear on the distribution curve). This is due to the fact that young cells appear that differ in size from mature red blood cells. If drug therapy is effective, the anisocytosis index normalizes, but it is the most recent of all erythrocyte indices to normalize.
offers automatic hematology analyzers from the European manufacturer DIATRON. These analyzers measure, in addition to other standard indicators, the distribution width of red blood cells (RDW) in two versions: RDW-CV and RDW-SD, which fully shows the heterogeneity of the size of the red blood cell population in the test sample. A wide range of DIATRON analyzers is represented by analyzers of various capacities (from 30 to 80 tests per hour), with various technical characteristics (small sample module, auto-puncture function, auto-loading, etc.). This allows us to fully meet the needs of laboratories of various sizes and specializations (primary medical care centers, family doctors, pediatrics, oncology, etc.). The company offers an individual approach to each client in terms of payment, delivery and service. We provide warranty and post-warranty service.
Analysis for RDW in MedArt
The medical laboratory is equipped with modern high-precision equipment, high-quality reagents, all necessary consumables and qualified personnel. Our clients can rest assured of the reliability: if all preparation recommendations are followed, the results obtained will be 100% accurate. rdw in the blood test is reduced
Our team performs the work quickly, efficiently and with due understanding. Since there are people who are catastrophically afraid of any medical intervention, including blood sampling, we try to provide all our clients with the most comfortable and calm atmosphere, while performing all hematological studies at the highest level and providing accurate results.
With us, you can take a general blood test in a calm and comfortable environment and get a reliable result in the shortest possible time at an affordable price, without waiting in line for long hours, and then endlessly visiting doctors in an attempt to find out the result. We care about each of our clients and strive to do our work with the highest quality possible.