The high prevalence of arterial hypertension (AH) among patients of different ages is still a serious and not fully resolved medical problem. What to do - mortality associated with the consequences of hypertension remains high. This explains the interest of ordinary citizens in diseases of the heart and blood vessels, forcing them to look for answers to the question of what to do.
There is increasing interest in a relatively new term: isolated systolic hypertension (ISAH). Moreover, patients are interested in both the features of the course of the pathology and what to do, as well as the reasons why the “upper” pressure is high and the “lower” pressure is low. What to do is the second most common question in this topic.
The concept of systolic and diastolic pressure
To figure out what to do, it is useful to have an understanding of blood pressure and why it is usually measured in two quantities.
- The so-called “upper” blood pressure is called systolic, since it is noted at the moment of systole. This is the period of time when the heart, filled with blood, begins to release it into the arteries. Naturally, the heart muscle contracts at this moment, and the heart valve opens.
- The process opposite to systole is the “absorption” of a new portion of blood by the heart at the time of diastole, when the heart muscle becomes relaxed.
Let's talk about normal blood pressure in order to understand the abnormality of the situation when the “upper” pressure is high and the “lower” pressure is low, and what to do about it.
The optimal blood pressure levels are known - these are the notorious 120 over 80, at which a person is considered extremely healthy. But in some cases, a person can be considered healthy at both higher and lower blood pressure values. Deviations are allowed within 30 mmHg. Art.
Phases of the cardiac cycle. Systole and Diastole.
Blood pressure: deviations from the norm, measurement methods, treatment and prevention of diseases
Blood pressure has such a huge impact on our health and well-being that it is important to monitor it, especially in adulthood.
Blood pressure is one of the main indicators of the body’s condition, and its measurement is a mandatory part of a comprehensive health examination. Even a slight deviation from the norm can be risky. It should be noted that problems with blood pressure occur at different ages, both in elderly and very young people.
Why is the “lower” pressure low and the “upper” normal?
When we talk about optimally acceptable deviations in blood pressure, we mean approximately the same high or low systolic and diastolic values. The difference between these values should normally remain approximately the same - about 40 mmHg. Art.
- This difference is called pulse pressure, and in some cases its value is a prognostic predictor (factor) of the development of cardiac or brain pathologies.
- Deviations from the norm for this value (pulse difference) are also permissible - up to 10 units in both directions.
- An indicator of normality, such as the percentage ratio of pulse pressure to systolic pressure, also serves as a guide. Normally, the pulse difference should not be low (less than 25% of SBP).
Why is the “lower” pressure low and the “upper” normal? Such a discrepancy in indicators is observed in a rare condition - isolated diastolic hypotension (low DBP), clinical cases of which are so infrequent that it is difficult to describe them based on medical archives. What to do? To date, no drug has been invented that can individually influence one of the low blood pressure indicators. Even the awareness of doctors regarding the conclusion of the special program of the Ministry of Health regarding isolated pathologies of blood pressure remains extremely low. Therefore, at the nearest clinic, when asked what to do, you will most likely be offered symptomatic therapy.
ABPM indicators in practical and research cardiology.
Akselrod A.S., Head of the Department of Functional Diagnostics, Cardiology Clinic of the MMA named after. THEM. Sechenov
The physiological interpretation of most indicators of 24-hour blood pressure monitoring (ABPM) is still widely debated in the literature today. It is customary to divide ABPM indicators into standard and additional. As a rule, it is the standard indicators that are presented in most registrars, since the main practical conclusions necessary for the selection of antihypertensive therapy are based on them.
Standard ABPM indicators
Standard indicators of ABPM include the following:
- average values of systolic (SBP), diastolic (DBP), average and pulse (PAP) blood pressure, as well as average heart rate for 24 hours, day and night;
- hourly average blood pressure and heart rate values;
- maximum and minimum values of blood pressure and heart rate for different periods of the day;
- daily index (degree of decrease in systolic and diastolic blood pressure at night);
- “pressure load” indicators: hypertension time index (TI), measurement index, hypertension area index (AI);
- variability of systolic, diastolic, mean and pulse blood pressure and heart rate.
Standard ABPM indicators are calculated automatically by the software and, most often, provided to the user in the form of a table (Figure 1).
Rice.
1. Standard indicators of ABPM: average values of systolic (SBP), diastolic (DBP), average and pulse (PBP) blood pressure, average heart rate per day, day and night; maximum and minimum values of blood pressure and heart rate for different periods of the day; daily index (degree of decrease in systolic and diastolic blood pressure at night, “day-night difference”).
Average values of systolic, diastolic, average and pulse blood pressure, average heart rate
per day, day and night.
Average blood pressure values
during the day, night and daytime (Figure 1) are presented in all recorders. The blood pressure level reflects the value of peripheral resistance.
In most cases, arithmetic mean blood pressure values are used as average values. The use of the median and mode is currently not widespread due to the overestimation of true blood pressure values. In accordance with the recommendations of the European Society of Hypertension, the normal level of daytime blood pressure should not exceed 135/83 mm Hg. Art., night – 120/70 mm Hg. Art. Blood pressure above 140/90 mmHg is considered elevated. and 125/75 mm Hg. during the day and night, respectively.
Pulse blood pressure
(Figure 1) characterizes the dynamic component of the pressor effect on target organs, and is also an indirect indicator of increased rigidity of large arterial vessels. High pulse pressure (PP) is an independent risk factor for coronary atherosclerosis and left ventricular hypertrophy. Due to the large number of publications on the possibility of using average PP as an independent predictor of coronary complications, many manufacturing companies have included this indicator in the list of standard ABPM indicators. In the absence of automatic calculation of PP in the software, this indicator can be easily calculated as the difference between the average values of SBP and DBP for the studied period of time.
Determination of average heart rate
during the day, daytime and nighttime are traditionally included in the list of standard ABPM indicators (Figure 1). It has been proven that people with tachycardia are predisposed to further development of atherosclerosis and hypertension. That is why a number of large international studies (Framingham, NHANES) have proven a connection between heart rate and cardiovascular mortality (including the risk of sudden death) in all age groups. Currently, the upper normal limit of average heart rate is considered to be 85 beats/min.
Maximum and minimum values of blood pressure and heart rate during the day
(Figure 1), as well as
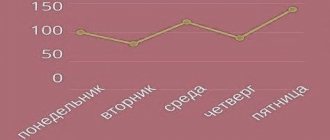
hourly average values of blood pressure and heart rate
(Figure 2) allow us to study in more detail the features of the circadian rhythm of blood pressure and, accordingly, select the most optimal antihypertensive therapy.
Fig.2. Hourly average blood pressure and heart rate values.
Circadian rhythm of blood pressure and circadian index.
Assessing the characteristics of the circadian rhythm of blood pressure is absolutely necessary to decide on the need to prescribe and correct therapy. Therefore, it is of undoubted interest to assess the differences between the values of average daytime and nighttime blood pressure, i.e. severity of biphasic blood pressure rhythm. A healthy person should have a decrease in systolic and diastolic blood pressure at night by 10-20%. The simplest and most widely used method in clinical practice for assessing the circadian rhythm of blood pressure is to calculate the degree of nocturnal decrease in blood pressure - the diurnal index (CI).
The daily index is calculated using the following formula:
SI=100%x (ADd-ADn)/ADd, where ADD is the average BP during the waking period, BPn is the average BP during the sleep period.
Depending on the value of SI, 4 types of daily blood pressure curves are distinguished (Table 1). Table 1. Types of daily blood pressure curves
Why is the “upper” pressure high and the “lower” pressure low?
Almost the same can be applied to the situation when the “upper” pressure is high and the “lower” pressure is low. But in the case of high systolic blood pressure and low DBP, we are talking about a more dangerous condition called isolated systolic arterial hypertension (ISAH).
The diagnosis is made when systolic blood pressure is fixed at 140 mmHg. Art. and above, and diastolic - 90 and below. The condition is most typical in older people (15–20%) from 55 to 80 years old and tends to increase in proportion to age. What to do for patients at risk:
- women;
- patients with diabetes mellitus;
- overweight people?
What to do if the “upper” pressure is high and the “lower” pressure is low, and this indicates a decrease in the elasticity of the arteries and a deterioration in the compensatory response of the vessel walls to cardiac output? Hypertensive patients with low DBP are more at risk of complications associated with heart and brain pathologies, as has been repeatedly demonstrated by the results of the MRFIT (International Risk Factor Trial Study) in Copenhagen and Framingham. Despite the increased interest of international health organizations in isolated hypertension, scientists are not yet ready to accurately answer the question of why the upper pressure is high and the lower pressure is low.
Heart health indicator
The heart muscle constantly pumps blood into the veins and arteries. Passing through them, blood puts pressure on the walls of blood vessels. Thus, blood pressure depends on the work of the heart and the elasticity of the blood vessels.
Pressure is not a constant value; it fluctuates depending on heartbeat cycles. The heart muscle contracts and relaxes approximately 60-80 times per minute. Systolic blood pressure is the maximum pressure recorded at the moment of heart contraction. In the interval between two contractions, when the heart relaxes, the pressure naturally decreases. The minimum pressure is called diastolic.
Blood pressure is measured in millimeters of mercury (mmHg). Systolic blood pressure is always listed first, and diastolic blood pressure is always listed second. Normal blood pressure is in the range of 110/70-130/85.
In addition to problems with the heart and blood vessels, blood pressure is influenced by a variety of factors - for example, physical activity, stress and addiction to tea and coffee increase blood pressure, and in weather-sensitive people it can fluctuate due to weather changes.
High blood pressure
Blood pressure 135/85-139/89 is considered elevated. If this figure reaches 140/90, then we can already talk about hypertension.
High blood pressure is a very dangerous condition. As is known, an increase in pressure for every 10 mm Hg. Art. increases the risk of developing cardiovascular diseases by a third. People with high blood pressure are 7 times more likely to develop cerebrovascular accidents (stroke), 4 times more likely to develop coronary heart disease, and 2 times more likely to develop vascular damage to the legs. In addition, hypertension can lead to poor vision and adversely affect kidney function.
What does it mean if there is a big difference between SBP and DBP?
Doctors who are actively involved in the issue of ISAH and what to do about it clearly understand that elevated systolic blood pressure (SBP) has a much greater impact on the development of heart attacks, ischemic heart disease or cerebral strokes than DBP.
- Thus, in the process of observing different groups of patients, it was noticed that increased SBP can increase the risk of developing coronary artery disease by 3.7 times, and increased DBP by 2.8 times.
- With increased SBP, the risk of cerebral stroke increases by 8.2 times, and with increased DBP - only 4.4 times.
- With SBP above 160 and low DBP (less than 90), the incidence of stroke is several times higher than with the same SBP value, but with DBP more than 90 mmHg. Art.
Thus, a direct dependence of the frequency of threatening conditions on the value of pulse pressure was discovered. As can be seen from the above figures, a high pulse difference indicates an increased risk of stroke.
Moreover, it was possible to establish that a high pulse difference has the greatest prognostic value in women with hypertension from 49 to 70 years old.
About the condition when the lower pressure is low and the upper pressure is high, it is known that this means, first of all, a high pulse difference.
A high pulse difference for certain groups of patients is an immutable risk factor for the development of cerebral or cardiac accidents. You can draw your own conclusion - if such an imbalance is detected, you need to be examined and get a doctor’s recommendations for further action.
Rules for measuring blood pressure
To get a reliable picture of a person’s health, it is important to measure blood pressure correctly; it’s not difficult:
- for an hour (at least 40 minutes) do not smoke, do not eat anything spicy, fatty, salty, do not drink strong drinks, coffee, tea;
- do not engage in physical labor;
- the position for measurement should be comfortable, in a sitting position, the hand for tonometry should be on a hard surface;
- two measurements are carried out, with an interval of several minutes;
- the cuff is placed above the elbow to make it comfortable when using a stethoscope.
What to do?
The difficulty of applying therapeutic measures in relation to isolated hypertension lies in the fact that not a single antihypertensive drug has the ability to specifically lower high or increase low blood pressure. Therefore, both doctors and patients were left to their own devices, not knowing what to do.
- Until recently, due to fear of a decrease in DBP, drug therapy was not carried out in most patients with ISAH.
- The answer to the question of what to do if the “upper” pressure is high and the “lower” pressure is low, came down to the use of non-drug methods.
- However, practical experience has shown that low DBP (below 80 mm) does not worsen the prognosis and increase the incidence of complications from the heart and blood vessels, including heart failure.
- Lowering SBP to 140 units and below prevents severe and fatal hypertension, which has become the ultimate goal of ISAH therapy.
Today, treatment of this pathology involves the use of a complex of therapeutic measures, including medicinal and non-medicinal.
Non-drug measures are striking in their simplicity and proven effectiveness.
- Limit sodium chloride (salt) intake. Patients at risk for ISAH (especially postmenopausal women) exhibit high salt sensitivity (up to 50% of cases), which immediately affects the condition of blood vessels. Therefore, limited consumption of this product is often considered a significant factor in lowering blood pressure.
- Restrictions should also be made for cholesterol-containing products.
- The gradual introduction of additional physical activity also helps to stabilize blood pressure, primarily due to weight loss.
- Smoking cessation should be an indispensable condition for success in the treatment of isolated hypertension. This needs to be done as soon as possible.
Medicines
Among medications for pharmacotherapy of ISAH, preference should be given to drugs with a diuretic effect. If their use is for some reason unacceptable, it is worth focusing on calcium antagonists (calcium channel blockers) from the dihydropyridine group, prescribed for ischemic heart disease and arrhythmias.
As additional components of complex drug therapy, angiotensin-converting enzyme (ACE) inhibitors can be added to calcium antagonists and diuretics, with preliminary dosage selection. The most popular combination among cardiologists is Perindopril (2 mg) + Indapamide (0.625 mg).
What to do with other known groups of antihypertensive drugs? They cannot yet be recommended for the treatment of conditions where the upper pressure is high and the lower pressure is low. Today there is no information about their effectiveness specifically in the isolated form of hypertension, and the experience of practical use is limited. In any case, you should ask your doctor what to do with isolated hypertension.
Blood pressure (BP). How to measure blood pressure correctly?
It is known that the total amount of blood in the body is 6–8% of body weight. Using a simple calculation, you can easily find out the blood volume of each person. So, with a weight of 75 kilograms, the blood volume is 4.5 - 6 liters. And all of it is enclosed in a system of vessels communicating with each other. So, when the heart contracts, blood moves through the blood vessels, puts pressure on the wall of the arteries, and this pressure is called arterial pressure. Blood pressure helps move blood through the vessels.