Make an appointment by phone: +7 (343) 355-56-57
+7
- About the disease
- Cost of services
- Sign up
- About the disease
- Prices
- Sign up
Extrasystole is an extraordinary contraction of the heart.
It can occur in the atrium, then it is called atrial.
If an extraordinary, “unscheduled” contraction comes from the ventricular myocardium, then it is called
ventricular.
observes and treats this type of arrhythmia .
Development mechanisms, types
During extrasystole, the conduction system of the heart operates in a “normal” mode.
However, one or more arrhythmic foci periodically turn on. This leads to an extraordinary contraction of the heart - extrasystole (ES). If this is the same arrhythmic focus, then ES is called monotopic
.
With several arrhythmic foci, the extrasystole is polytopic.
If ES occur in a certain rhythm (every second contraction, every third, etc.), then they are called allorhythmias
.
When registering several ES in a row, they are called group.
In this case, restoration of normal (sinus) rhythm can occur both spontaneously, independently, and with the help of medications - antiarrhythmic drugs.
In most cases, ES does not pose a direct threat to health and does not pose a threat to life. This primarily applies to atrial ES.
Ventricular extrasystoles, especially polymorphic
(that is, the morphology of the complex changes), polytopic (coming from different sources) and group (several ES in a row) are considered life-threatening. Because they are the precursor of more serious, life-threatening arrhythmias - such as ventricular tachycardia.
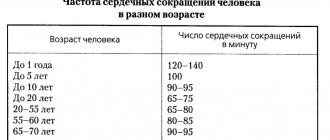
Normally, no more than 200 extrasystoles are recorded per day. A greater number of extrasystoles per day is considered pathological.
Prevention
There is no point in treating extrasystole if the main causes of its occurrence are not removed. This is precisely what prevention is aimed at. To this end, it is recommended to follow the following tips:
- avoid stressful situations, get enough rest;
- Get a good night's sleep - this is an important factor in the body's recovery;
- Despite the fact that heavy physical activity can cause attacks, complete adynamia also negatively affects the heart. Moderate exercise is a good preventive measure;
- limit the consumption of alcoholic beverages, coffee, strong tea;
- stop smoking;
- practice massage and breathing exercises;
- Eat foods high in potassium (banana, avocado, baked potatoes, dried apricots, spinach) and magnesium (wheat bran, cocoa, buckwheat, cashews and almonds).
Following these simple rules will help not only get rid of extrasystoles, but also improve your overall health.
Reasons for development:
1. viral diseases
2. pathology of the gastrointestinal tract:
- gastroesophageal
- reflux disease
- chronic pancreatitis
- ulcerative colitis
3. diseases of the cardiovascular system:
- inflammatory (myocarditis)
- hypertonic disease
- coronary heart disease (myocardial infarction)
- heart defects
- heart failure
4. bad habits:
- smoking
- alcohol abuse
- addiction
5. acute, chronic diseases of the bronchopulmonary system (pneumonia, chronic obstructive bronchitis, bronchial asthma)
6. inflammatory diseases of the ENT organs, oral cavity
7. reduced immunity
8. sleep apnea syndrome
9. exacerbation of any pathology of internal organs
Characteristic symptoms
Typical symptoms and complaints of patients are:
- Feeling of heart failure. Normally, there should be no sensations of heartbeat. If they appear in any form (beats in the heart area, interruptions, trembling, turning over), this should alert you to extrasystole.
- Irrhythmic pulsation of arteries (in the neck, chest, limbs). The pulse becomes intermittent, arrhythmic - between regular rhythmic beats there are extraordinary ones, followed by a pause.
- General weakness, powerlessness, dizziness, fainting. They are accompanied only by frequent extrasystoles, causing circulatory disorders (primarily in the brain).
- A slight feeling of constriction in the chest and lack of air, shortness of breath. With extrasystoles up to 10-15 per minute, they are disturbing during exercise, and with more frequent ones - even at rest.
- Anxiety, restlessness, trembling throughout the body, an unmotivated feeling of fear. This is how multiple extrasystoles appear.
Treatment
Many drugs have been proposed for the treatment of ES.
The main task is to identify and eliminate the cause of the disease. Treatment will be ineffective if the provoking factor persists. Extrasystole refers to “persistent” rhythm disturbances, which are not easy to cope with. If conservative tactics are not effective, the patient is referred to cardiac surgeons to eliminate the arrhythmogenic focus using ablation. Typically, cardiac surgical methods are used if more than 10-15 thousand ES per day persists during therapy.
The essence of pathology
The human heart consists of two functional halves: the upper one is the atria, and the lower one is the ventricles.
Normally, the automatic occurrence of impulses that cause contraction of the heart muscle occurs at the highest point of the heart - the sinus node. These impulses are so strong and frequent that they alternately pass through all sections from top to bottom, suppressing any other nervous stimulation. There is a synchronous contraction (relaxation) of the atria and then the ventricles. While the former are tense, the latter are relaxed and vice versa.
With supraventricular extrasystole, cardiac activity is structured in such a way that exciting impulses arise not only in the sinus node: additional (abnormal) foci located in the upper half of the heart become their generators.
The occurrence of an extraordinary impulse forces the heart to perform an additional contraction, preventing the heart muscle from resting and filling with blood at the moment when it should be relaxed.
If supraventricular extrasystole occurs frequently (more than 5–6 times per minute), then it:
- redistributes blood flow;
- disrupts blood circulation throughout the body, provokes heart failure;
- overstrains and depletes the myocardium.
Only extrasystoles that occur in the sinus node up to 5-6 times per minute are a normal variant. If their frequency is the same, but the source is an additional focus in the supraventricular zone of the heart, this is a pathology. And although more than 95% of patients with single ventricular extrasystoles do not have any symptoms, the likelihood of further deterioration is extremely high (60–70%).
How is extrasystole diagnosed?
Having analyzed the patient’s complaints, the doctor proceeds to an objective examination, through which pulsation of the jugular vein (presystolic) and arrhythmic cardiac activity are detected. Auscultation reveals a change in the sound of the 1st tone and a bifurcation of the 2nd.
Next, it is necessary to conduct instrumental studies. Initially, an ECG and Holter monitoring are advisable. They record unscheduled ventricular contraction, atypical QRS, absence of P before the extrasystole.
The bicycle ergometry used helps to determine the cause through physical activity. With the idiopathic type, extrasystoles decrease after exercise. If cardiac changes are present, the load only provokes the formation of extrasystole.
If necessary, TEE, rhythmocardiography, and echocardiography are recommended. When there is ventricular extrasystole, its treatment is determined after examination, otherwise fibrillation is likely.
Lead tactics
Functional extrasystole does not interfere with the normal course of pregnancy and gestation. We usually do not identify any contraindications to natural delivery. A woman can give birth to a healthy baby at term and avoid complications.
Extrasystole associated with organic damage to the heart or other organs, endocrine disorders and other conditions requires mandatory observation by a specialist. The management tactics for a woman will depend on the severity of the underlying disease.
All pregnant patients, regardless of the severity and form of extrasystole, are under the supervision of a therapist and cardiologist until delivery. If the condition of the woman and fetus is stable, a control examination (ECG) is carried out before birth. If the patient's condition worsens or complications of gestation develop, additional examination is indicated.
Indications for caesarean section for extrasystole are rare. They are usually associated with concomitant pathology or complications of pregnancy. In a planned procedure, the operation is performed at 37-39 weeks, in an emergency - at any time.
Have you encountered such a phenomenon as extrasystole during pregnancy? What did the doctor recommend to you in this situation?
Who has it?
Supraventricular extrasystole (SE) occurs in 60-70% of people . Normally, it can also occur in clinically healthy patients.
The presence of supraventricular extrasystole (SVES)
does not mean that a person is sick.
SE is more often registered in adults and older children , since young children are not yet able to describe their sensations and do not really understand what is happening to them.
In newborns and young children, supraventricular extrasystole is detected during an ECG during medical examination, general examination, or in connection with an alleged disturbance in the functioning of the heart (congenital defects, a sharp deterioration in the child’s condition in the absence of external factors).
Forecast
If the cause is established and appropriate treatment measures are taken, the consequences of 80–90% of supraventricular extrasystoles are not severe or fatal. They are cured either completely or reduce their severity.
For this, in 80–85% conservative treatment is sufficient (taking medications for years in the form of courses of several weeks or months during an exacerbation), in 15–20% surgery is required. The latter method is 95% effective. But even it cannot help with pathology that causes irreversible changes in the heart.
In 70–80%, single extrasystoles (less than 5 times per minute) are eliminated only by diet and lifestyle correction.
Not contacting a specialist or not following his recommendations, even in the presence of rare extrasystoles, is the wrong decision. Sooner or later everything will end with the progression of the disease. Don't let this happen and stay healthy!
Diagnostics and its methods
Most often, the primary diagnosis is an electrocardiogram. Most often, extrasystole is detected during a medical examination and requires a more thorough study of the heart.
Sometimes, if the patient already has symptoms of some kind of heart problems after physical activity, then diagnostic procedures are used that measure the heart rate after physical activity.
In addition to these methods, there is also a classic examination by a doctor, where he measures the patient’s pulse and listens to the work of the heart.
- Why ventricular extrasystole occurs, symptoms and treatment of pathology
conclusions
Extrasystole is an extraordinary generation of an impulse followed by a contraction of cardiomyocytes. Extrasystoles are sometimes harmless, but in other cases they can provoke atrial fibrillation, the consequence of which will be sudden death.
The army will perceive a cardiological conclusion about the presence of polymorphic, paired or group extrasystoles negatively and will deny the man the opportunity to serve.
Prevention of extrasystole - a healthy lifestyle (physical exercises during sedentary work are required).