Coronary angiography
MITRAL VALVE SURGERY – MITRAL COMISSUROTOMY
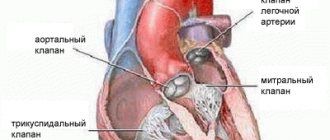
The mitral valve (bicuspid valve) of the heart is the valve between the left atrium and the left ventricle of the heart. It is represented by two connective tissue plates that prevent, during left ventricular systole, regurgitation (backflow) of blood into the left atrium.
Various pathological processes, both acquired and congenital, can cause valve dysfunction.
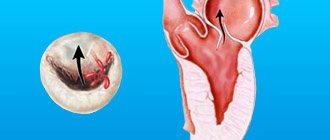
Mitral commissurotomy is a method of surgical treatment of congenital or acquired pathology of the mitral valve. MITRAL COMISSUROTOMY is a surgical operation whose purpose is to dissect the adhesions of the petals of the mitral heart valve (commissures).
Mitral commissurotomy is performed to treat mitral stenosis, a pathological narrowing of the mitral valve of the heart (between the left atrium and ventricle). The operation is performed on all patients with mitral stenosis, with the exception of the first stage of the disease, when the body’s own compensatory mechanisms allow it to easily cope with the resulting disorders.
There are two types of mitral commissurotomy:
Closed
Open
CLOSED MITRAL COMISSUROTOMY
Closed mitral commissurotomy is a surgical separation of the fusions of the left atrioventricular orifice in case of its stenosis.
This operation is performed on a closed heart without the use of artificial (extracorporeal) circulation from a left- or right-sided thoracotomy approach.
After transesophageal echocardiography has excluded the presence of a thrombus in the left atrial appendage, a purse-string suture is placed on it, the heart cavity is penetrated and a digital inspection is performed, thus assessing the condition of the mitral valve, determining the degree of its stenosis (narrowing) and the mobility of the leaflets.
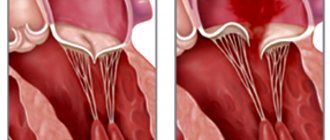
Loose adhesions can be separated manually, dense adhesions - only with the help of special instruments (dilators, commissurotomes), which expand the narrowed mitral orifice to a diameter of 3.5-4 centimeters.
In order to reduce the risk of embolism of the arterial vessels of the brain, it is recommended to apply pressure on the carotid arteries at the time of performing this manipulation.
The inability to perform an adequate closed commissurotomy is considered a reason to switch to extracorporeal circulation and perform open surgery.
Since the 1950s, since the introduction of artificial blood circulation into practice, closed mitral commissurotomy has been replaced by prosthetics.
The use of closed commissurotomy is now considered justified only when it is not possible for one reason or another to perform artificial circulation. Closed mitral commissurotomy is sometimes performed in pregnant women with severe mitral stenosis.
With closed commissurotomy, there is a high probability of mitral regurgitation and embolism, especially in the case of atrial thrombosis and the presence of valve calcification.
OPEN MITRAL COMISSUROTOMY
Open mitral commissurotomy is an operation that involves performing a median sternotomy and switching to extracorporeal circulation with so-called bicaval cannulation.
Open mitral commissurotomy is used when there is mild damage to the patient’s valve apparatus in the absence of massive calcification.
The surgeon enters the left atrium from its posterior surface in the area of the interventricular groove. After the mitral valve is exposed, they begin the commissurotomy itself, first of all identifying the area of fusion of the leaflets, and then cutting this area in the direction from its free end to the fibrous ring. Then the chordae tendineae are carefully separated and the incision continues longitudinally to the papillary muscles.
In this case, small calcium deposits can be locally removed, while being careful not to damage the valve apparatus in any way.
Finally, the left atrium incision is sutured and artificial circulation is stopped.
Unlike closed commissurotomy, the open technique allows for more reliable removal of blood clots from the atrium and dissection of existing adhesions.
Open mitral commissurotomy gives excellent long-term results, but is associated with the risk of developing restenosis or valve insufficiency. Only a small proportion (no more than 7%) of all patients subsequently require mitral valve replacement.
MITRAL VALVE – MITRAL COMISSUROTOMY
Ichilov Hospital / CARDIAC SURGERY / Mitral valve – Mitral commissurotomy
Mitral valve (bicuspid valve) of the heart
- valve between the left atrium and left ventricle of the heart. It is represented by two connective tissue plates that prevent, during left ventricular systole, regurgitation (backflow) of blood into the left atrium.
Mitral commissurotomy
- a surgical operation, the purpose of which is to dissect the adhesions of the petals of the mitral valve of the heart (commissures).
Mitral commissurotomy is performed to treat mitral stenosis, a pathological narrowing of the mitral valve of the heart (between the left atrium and ventricle). The operation is performed on all patients with mitral stenosis, with the exception of the first stage of the disease, when the body’s own compensatory mechanisms allow it to easily cope with the resulting disorders.
There are two types of mitral commissurotomy:
Closed
Open
CLOSED MITRAL COMISSUROTOMY
Closed mitral commissurotomy
- this is the surgical separation of the fusions of the leaflets of the left atrioventricular orifice in case of its stenosis.
This operation is performed on a closed heart without the use of artificial (extracorporeal) circulation from a left- or right-sided thoracotomy approach.
After transesophageal echocardiography has excluded the presence of a thrombus in the left atrial appendage, a purse-string suture is placed on it, the heart cavity is penetrated and a digital inspection is performed, thus assessing the condition of the mitral valve, determining the degree of its stenosis (narrowing) and the mobility of the leaflets.
Loose adhesions can be separated manually, dense adhesions - only with the help of special instruments (dilators, commissurotomes), which expand the narrowed mitral orifice to a diameter of 3.5-4 centimeters.
In order to reduce the risk of embolism of the arterial vessels of the brain, it is recommended to apply pressure on the carotid arteries at the time of performing this manipulation.
The inability to perform an adequate closed commissurotomy is considered a reason to switch to extracorporeal circulation and perform open surgery.
Since the 1950s, since the introduction of artificial blood circulation into practice, closed mitral commissurotomy has been replaced by prosthetics.
The use of closed commissurotomy is now considered justified only when it is not possible for one reason or another to perform artificial circulation. Closed mitral commissurotomy is sometimes performed in pregnant women with severe mitral stenosis.
With closed commissurotomy, there is a high probability of mitral regurgitation and embolism, especially in the case of atrial thrombosis and the presence of valve calcification.
OPEN MITRAL COMISSUROTOMY
Open mitral commissurotomy
- an operation that involves performing a median sternotomy and switching to extracorporeal circulation with so-called bicaval cannulation.
Open mitral commissurotomy is used when there is mild damage to the patient’s valve apparatus in the absence of massive calcification.
The surgeon enters the left atrium from its posterior surface in the area of the interventricular groove. After the mitral valve is exposed, they begin the commissurotomy itself, first of all identifying the area of fusion of the leaflets, and then cutting this area in the direction from its free end to the fibrous ring. Then the chordae tendineae are carefully separated and the incision continues longitudinally to the papillary muscles.
In this case, small calcium deposits can be locally removed, while being careful not to damage the valve apparatus in any way.
Finally, the left atrium incision is sutured and artificial circulation is stopped.
Unlike closed commissurotomy, the open technique allows for more reliable removal of blood clots from the atrium and dissection of existing adhesions.
Open mitral commissurotomy gives excellent long-term results, but is associated with the risk of developing restenosis or valve insufficiency. Only a small proportion (no more than 7%) of all patients subsequently require mitral valve replacement.
In Israeli cardiology clinics, patients receive high-quality medical care from highly qualified cardiac surgeons who select an individual approach to each patient.
Heart valve replacement surgery has become common in cardiac surgery clinics in Israel, thanks to modern operating rooms and highly trained surgeons. Valve replacement is performed not only on adults, but also on children.
- Cardiac surgery in Israel
- Human heart - structure and functions
- Heart and circulatory system
- Heart – Coronary arteries – Developmental anomalies
- Coronary arteries - Atherosclerosis
- Thoracic aorta – Aneurysm
- Abdominal aorta – Aneurysm
- Hypertrophic cardiomyopathy (HCM)
- Heart valve diseases
- Heart defects
- Heart – Congenital defects
- Diagnosis of congenital heart defects
- Atrial septal defect
- Ventricular septal defect
- Aortic valve stenosis
- Aortic valve insufficiency
- Mitral valve stenosis
- Mitral valve insufficiency
- Transposition of the great vessels
- Heart – Endocarditis
- Cardiac surgery patient – Examinations
- Examinations – Coronary angiography
- Outpatient coronary angiography
- CT Coronary Angiography and Interventional Coronary Angiography
- Examinations – Endovascular ultrasound diagnostics of coronary arteries
- Examinations – Cardiac catheterization
- Treatment of heart diseases
- Direct myocardial revascularization - history of development of methods
- Cardiac surgery – Minimally invasive surgeries
- Cardiac surgery – X-ray endovascular surgery
- Cardiac Surgery – Radiofrequency Ablation
- Cardiac Surgery – Arrhythmia and Pacemakers
- Cardiac surgery – Coronary angioplasty
- Cardiac surgery – Balloon angioplasty
- Cardiac surgery – Excimer laser angioplasty
- Cardiac Surgery – Percutaneous Coronary Interventions
- Coronary arteries – Stenting
- Stents - types
- Coronary stenting – Coronary stent restenosis
- Cardiac surgery – Coronary artery bypass grafting (CABG)
- Coronary artery bypass grafting (CABG) – Minimally invasive methods
- Coronary artery bypass grafting – Venous grafts
- Coronary artery bypass grafting – Radiation shunts
- Coronary artery bypass grafting (CABG) – Complications
- Coronary artery bypass grafting (CABG) – After surgery
- Coronary surgery – Operations without the use of a heart-lung machine
- Coronary artery bypass grafts – Balloon angioplasty of bypass grafts
- Coronary artery bypass grafts – Stenting
- Measures to prevent distal embolization
- Surgeries on the coronary arteries - Rehabilitation after surgery
- Heart valve pathologies - Treatment methods
- Heart valve surgery – Preoperative preparation
- Cardiac surgery – Anesthesia manual
- Surgeries on heart valves - Progress of the operation
- Heart defects – Open surgeries
- Cardiac surgery – Operations with a heart-lung machine
- Heart defects – Minimally invasive surgeries
- Heart valves – Artificial heart valves
- Kava filters
- Aortic valve – Open replacement
- Aortic valve – Ross operation
- Treatment of aortic stenosis – Minimally invasive techniques
- Aortic valve – Transcatheter implantation
- Aortic valve – Endovascular replacement
- Aortic valve – Non-stented artificial aortic valves
- Mitral valve – Mitral valve replacement
- Mitral valve – Mitral commissurotomy
- Tricuspid valve - Surgical interventions
- Infective endocarditis – Heart valve replacement
- Heart valve replacement – Prevention of postoperative complications
- Heart valve replacement – Anticoagulants after surgery
- Heart valve surgery - Life after surgery
- Heart Disease – Stem Cell Treatment
- Diseases of the cardiovascular system – Stem cell treatment
- Atherosclerosis – Stem cell treatment
- Hypertension – Stem Cell Treatment
- Atrial fibrillation – Stem cell treatment
- Angina – Stem Cell Treatment
- Dilated Cardiomyopathy – Stem Cell Treatment
- Myocarditis – Stem cell treatment
- Cardiosclerosis – Stem cell treatment
- Heart Failure – Stem Cell Treatment
- Coronary heart disease – Stem cell treatment
- Ischemic stroke – Stem cell treatment
- Hemorrhagic stroke – Stem cell treatment
- Myocardial infarction – Stem cell treatment
- Congenital heart defects – Stem cell treatment
- Cardiology Center MC Souraski (Ichilov Hospital)
- Pediatric cardiology and cardiac surgery MC Ikhilov
- Implantation of the Tiara valve at Ikhilov MC
- Professor Keren Gad – cardiologist
- Professor Bernard Belassin – cardiologist
- Dr. Bella Koyfman – cardiologist
- Dr. Amir Kramer – cardiac surgeon
- Professor Sammy Whiskin – cardiologist
- Professor Hilton Miller – cardiologist
- Professor Arie Roth – cardiologist
- Professor Gideon Uretsky – cardiac surgeon
- Professor Shmuel Banai – cardiac surgeon
- Dr. Rafael Rosso - cardiologist
- Dr. Nahum Nesher – cardiac surgeon
- Dr. Itzhak Hertz – cardiologist
- Dr. Yehuda Levy – cardiologist
- Cardiological diagnostics in Israel
- Heart valve replacement in Germany
- 1. Povetkin S.V., Zabelina I.V. Possibilities of transthoracic echocardiography in the diagnosis of congenital heart defects (clinical observations)//SonoAce-Ultrasound. 2010. No. 20. P. 14-16 Context: ...Congenital anomalies of the aortic valve account for up to 8.0% of all congenital heart defects [1, 2].
2. Bockeria L.A., Muratov R.M., Shatakhyan M.P. and others. Early results of orthotopic implantation in the pulmonary position of frameless xenopericardial conduits in adult patients // Thoracic and cardiovascular surgery. 2009. No. 1. Context: ...Congenital anomalies of the aortic valve account for up to 8.0% of all congenital heart defects [1, 2].
3. Dzemeshkevich S.L., Stevenson L.W., Aleksi-Meskhishvili V.V. Aortic valve diseases. M., 2004. 328 p. Context: ...In general, the share of aortic valve pathology is 30-35% of the number of patients with valvular heart defects, ranking second in prevalence after mitral valve defects, leading to severe disability and mortality [3, 4].
4. Shmatov D.V., Astapov D.A., Nazarov V.M. Immediate results of aortic valve replacement in patients with aortic stenosis and left ventricular systolic dysfunction // Circulatory Pathology and Cardiac Surgery. 2010. No. 4. P. 17-18 Context: ...In general, the share of aortic valve pathology is 30-35% of the number of patients with valvular heart disease, ranking second in prevalence after mitral valve defects, leading to severe disability and mortality [ 3, 4].
5. Karaskov A.M., Astapov D.A. and others. Long-term results of aortic valve replacement with frameless bioprostheses Kemerovo-AB-Mono, Kemerovo-AB-Composite, Kemerovo-AB-Neo // Circulatory pathology and cardiac surgery. 2011. No. 4. P. 25-27. Context: ...In addition, many years of experience in the surgical treatment of congenital and acquired aortic defects does not allow us to classify this type of operation as a radical type of intervention, since about 70% of patients require repeated interventions on average 6 years after surgery, and the frequency of late deaths reaches 8. 3% [5, 6].
6. Boriskov M.V., Efimochkin G.A., Gorbatykh Yu.N., Sinelnikov Yu.S. Valvular aortic stenosis in children: anatomical variants, indications and timing of surgical intervention, correction methods, results, development paths // Circulatory Pathology and Cardiac Surgery. 2009. No. 2. P. 73-77 Context: ...In addition, many years of experience in the surgical treatment of congenital and acquired aortic defects does not allow us to classify this type of operation as a radical type of intervention, since about 70% of patients require repeated interventions on average after 6 years after surgery, and the incidence of late deaths reaches 8.3% [5, 6].
7. Karaskov A.M., Demin I.I., Zheleznev S.I. and others. Ross procedure in patients with severe systolic dysfunction of the left ventricle // Pathology of blood circulation and cardiac surgery. 2013. No. 1. P. 6-7.
8. Thomson JDR Management of valvar aortic stenosis in children//Heart. 2004. Vol. 90(1). R. 5-6. Context: ...At the same time, one cannot fail to mention its disadvantages - the need to use artificial circulation in decompensated patients is characterized by a higher risk; increased complexity of future reoperation due to resternotomy [8].
9. Alsoufi B., Karamlou T., McCrindle Bw, Caldarone CA Management options in neonates and infants with critical left ventricular outflow tract obstruction//Eur. J. Cardiothorac. Surg. 2007. Vol. 31(6). R. 1013-21. Context: ... In this regard, research into the effectiveness of different methods of surgical correction of aortic valve stenosis in pediatric patients seems relevant and significant, since surgical intervention remains the only effective treatment method and currently does not have a worthy alternative [9].
10. McElhinney DB, Lock JE, Keane JF Left heart growth, function, and reintervention after balloon aortic valvuloplasty for neonatal aortic stenosis//Circulation. 2005. Vol. 111(4). R. 451-8. Context: ... Endovascular transluminal balloon valvuloplasty of the aortic valve for many years remained the preferred method of treating valvular aortic stenosis, mostly in newborns and children of the first year of life, because it was characterized by such advantages as: relative safety of the procedure; exclusion of median sternotomy, taking into account the likelihood of reoperation; eliminating the negative impact of extracorporeal circulation [10].
11. Brown JW, Rodefeld MD, Ruzmetov M. et al. Surgical Valvuloplasty Versus Balloon Aortic Dilation for Congenital Aortic Stenosis: Are Evidence-Based Outcomes Relevant?//Ann. Thorac. Surg. 2012. Vol. 94. R.146-55. Context: ...However, the method is not without significant drawbacks, including the frequent development of aortic valve insufficiency (up to 15-20% of cases) and its progression; damage to the femoral artery, especially in newborns; early re-intervention, high rate of re-operations [11].
12. Lambert V., Obreja D., Losay J. et al. Long-term results after valvotomy for congenital aortic valvar stenosis in children//Cardiol. Young. 2000. Vol. 10. R. 590-6. Context: ...In addition, this type of intervention avoids complications characteristic of balloon valvuloplasty [12].
13. Justo RN, McCrindle BW, Benson LN et al. Aortic valve regurgitation after surgical versus percutaneous balloon valvotomy for congenital aortic valve stenosis//Am. J. Cardiol. 1996. Vol. 77. R. 1332-8. Context: ...At the same time, according to other authors, the frequency of reoperations reached an average of 38%, varying from 13 to 50% [11-13].
14. Detter C., Fischlein T., Feldmeier S. et al. Aortic valvotomy for congenital valvular aortic stenosis: a 37-year experience//Ann. Thorac. Surg. 2001. Vol. 71. R. 1564-71. Context: ...The incidence of deaths in our study was consistent with the literature, although the results published by different authors vary widely - from 3 to 25%, with an average of 12% [12, 14].
Ichilov Clinic in Israel
Ichilov Clinic in Israel ¦ Cardiac surgery at the Ichilov Clinic ¦ Mitral commissurotomy - Ichilov Clinic
Mitral commissurotomy
- a surgical operation, the purpose of which is to dissect the adhesions of the petals of the mitral valve of the heart (commissures).
Mitral commissurotomy is performed at the Ichilov Clinic (Sourasky) in Israel to treat mitral stenosis, a pathological narrowing of the mitral valve of the heart (between the left atrium and ventricle). The operation is performed on all patients with mitral stenosis, with the exception of the first stage of the disease, when the body’s own compensatory mechanisms allow it to easily cope with the resulting disorders.
Closed mitral commissurotomy at the Ichilov Clinic (Souraski)
Closed mitral commissurotomy is a surgical separation of the fusions of the left atrioventricular orifice in case of its stenosis.
This operation is performed on a closed heart without the use of artificial (extracorporeal) circulation from a left- or right-sided thoracotomy approach.
After transesophageal echocardiography has excluded the presence of a thrombus in the left atrial appendage, a purse-string suture is placed on it, the heart cavity is penetrated and a digital inspection is performed, thus assessing the condition of the mitral valve, determining the degree of its stenosis (narrowing) and the mobility of the leaflets.
Loose adhesions can be separated manually, dense adhesions - only with the help of special instruments (dilators, commissurotomes), which expand the narrowed mitral orifice to a diameter of 3.5-4 centimeters.
In order to reduce the risk of embolism of the arterial vessels of the brain, it is recommended to apply pressure on the carotid arteries at the time of performing this manipulation.
The inability to perform an adequate closed commissurotomy is considered a reason to switch to extracorporeal circulation and perform open surgery.
With closed commissurotomy, there is a high probability of mitral regurgitation and embolism, especially in the case of atrial thrombosis and the presence of valve calcification.
Open mitral commissurotomy at the Ichilov Clinic (Souraski)
Open mitral commissurotomy is an operation that involves performing a median sternotomy and switching to extracorporeal circulation with so-called bicaval cannulation.
Open mitral commissurotomy is used when there is mild damage to the patient’s valve apparatus in the absence of massive calcification.
The surgeon enters the left atrium from its posterior surface in the area of the interventricular groove. After the mitral valve is exposed, they begin the commissurotomy itself, first of all identifying the area of fusion of the leaflets, and then cutting this area in the direction from its free end to the fibrous ring. Then the chordae tendineae are carefully separated and the incision continues longitudinally to the papillary muscles.
In this case, small calcium deposits can be locally removed, while being careful not to damage the valve apparatus in any way.
Finally, the left atrium incision is sutured and artificial circulation is stopped.
Unlike closed commissurotomy, the open technique allows for more reliable removal of blood clots from the atrium and dissection of existing adhesions.
Open mitral commissurotomy gives excellent long-term results, but is associated with the risk of developing restenosis or valve insufficiency. Only a small proportion (no more than 7%) of all patients subsequently require mitral valve replacement.
(495) 506-61-01 — urgent organization of treatment in Israel
REQUEST TO THE CLINIC
| Diagnosis of heart diseases - Ichilov Clinic |
| Diseases of the cardiovascular system - causes |
| Diseases of the cardiovascular system - symptoms |
| Prevention of heart disease |
| Heart treatment - heart treatment methods in Israel |
| Minimally invasive heart surgery – Ichilov Clinic |
| X-ray endovascular surgery – Ichilov Clinic |
| Radiofrequency ablation – Ichilov Clinic |
| Artificial pacemaker - Ichilov Clinic |
| Coronary angioplasty – Ichilov Clinic |
| Balloon angioplasty – Ichilov Clinic |
| Excimer laser angioplasty – Ichilov Clinic |
| Percutaneous coronary interventions – Ichilov Clinic |
| Stenting of coronary arteries – Ichilov Clinic |
| Coronary artery bypass surgery – Ichilov Clinic |
| Minimally invasive coronary artery bypass surgery – Ichilov Clinic |
| Heart surgery without the use of a heart-lung machine |
| Surgeries on heart valves - Ichilov Clinic |
| Heart defects - treatment in Israel |
| Heart-lung machine - treatment in Israel |
| Artificial heart valves - treatment in Israel |
| Kava filter - treatment in Israel |
| Aortic valve replacement – Ichilov Clinic |
| Ross operation - heart valve surgery in Israel |
| Aortic valve stenosis - minimally invasive treatment in Israel |
| Transcatheter aortic valve implantation in Israel |
| Endovascular aortic valve replacement in Israel |
| Mitral valve replacement – Ichilov Clinic |
| Mitral commissurotomy – Ichilov Clinic |
| Operations on the tricuspid valve - Ichilov Clinic |
| Infective endocarditis - treatment in Israel |
| After surgery on heart valves - Ichilov Clinic |
| Thoracic aortic aneurysm - treatment in Israel |
| Hypertrophic cardiomyopathy - treatment in Israel |
| Stem cells in the treatment of cardiovascular diseases |
| Atherosclerosis - stem cell treatment in Israel |
| Arterial hypertension - stem cell treatment in Israel |
| Atrial fibrillation - stem cell treatment in Israel |
| Angina pectoris - stem cell treatment in Israel |
| Myocardial dystrophy - stem cell treatment in Israel |
| Myocarditis - stem cell treatment in Israel |
| Myocardiosclerosis - stem cell treatment in Israel |
| Heart failure - stem cell treatment in Israel |
| Cardiac ischemia - stem cell treatment in Israel |
| Brain infarction - stem cell treatment in Israel |
| Hemorrhagic stroke - stem cell treatment in Israel |
| Myocardial infarction - stem cell treatment in Israel |
| Congenital heart disease - stem cell treatment in Israel |
SURGERY
J. Bender
AND
Infectious complications after surgery pose a threat to patients, cause morbidity, affect the workload of hospital staff, and their development leads to increased costs for the hospital and health insurance companies for treatment. Antibiotic prophylaxis has been beneficial for the past 20 years, and there has recently been some agreement that effective prophylaxis can be achieved with a single dose of an appropriate drug (or combination of antibiotics) at the start of surgery. Administration of a single dose reduces the likelihood of the emergence of resistant strains of microorganisms and is cheaper than repeated doses of antibiotics. G. Anderson et al., from two university hospitals in Melbourne, Australia, conducted a prospective study to evaluate the effectiveness and costs of three antimicrobial regimens used to prevent infectious complications after abdominal surgery. 1070 patients were randomly assigned to receive one of three treatment regimens consisting of ceftriaxone (1 g IV) or cefotaxime (1 g IV)—both third-generation cephalosporins—or ticarcillin, a moderately broad-spectrum penicillin, in combination with clavulanic acid (3.1 g of this combination intravenously). Interventions included appendectomy, elective and emergency colorectal surgery, esophagogastroduodenal surgery, small bowel resection, cholecystectomy, and common bile duct examination. Patients undergoing appendectomy or colorectal surgery were given an additional 500 mg intravenous metronidazole, which is effective against anaerobic organisms and protozoa (Trichomonas), if they were randomized to receive one of the cephalosporins. Metronidazole was not added if the patient received ticarcillin plus clavulanic acid after randomization. Wound infections were defined as dangerous when hospital stay was prolonged or reoperation was required; A wound infection was considered minor if it did not affect the length of hospital stay. The following results were obtained: the rate of wound infections was 4.3%. Twenty-one (2%) patients developed a serious wound infection, as expected primarily after colorectal surgery, whereas 25 (2.3%) patients had minor wound infections. There was no difference in the severity of wound infections between the three groups receiving different treatment regimens; The fewest minor complications (virtually none) were observed in the ceftriaxone group; infections were caused mainly by Staphylococcus aureus and colon inhabitants such as Enterobacteriaceae and E. coli. No differences were found in the incidence of postoperative infections of other sites (lungs, urinary tract) between the three groups. The side effects of the antibiotics used were minimal: in the ceftriaxone group there was 1 case of mild thrombocytopenia, which lasted only 1 day; another patient receiving cefotaxime experienced urticaria for a short period of time. Given that there was no difference in the incidence of infectious complications between the three groups, the researchers analyzed treatment costs. They accurately took into account not only the cost of purchasing drugs, but also the cost of necessary treatment for infectious complications that developed in any of the three groups. The cost of purchasing ceftriaxone was twice that of the other two regimens, which cost the same. Costs for treatment of infectious complications were highest in the ticarcillin plus clavulanic acid group, whereas they were similar in the other two groups. The authors concluded that both cephalosporins are equally effective against infectious complications after abdominal surgery. Since the acquisition costs of cefotaxime are lower, it may be the drug of choice for antimicrobial prophylaxis.
Literature:
Anderson G, Boldiston C, Woods S, O`Brien P. A Cost-effectiveness evaluation of 3 antimicrobial regimens for the prevention of infectious complications after abdominal surgery. Arch Surg 1996;131:744-8.
PERCUTANEOUS MITRAL COMISSUROTOMY
N. Mazur N. Mazur
D
This treatment method has been used for about 15 years, which has made it possible to obtain immediate and medium-term results of the intervention, as well as to determine indications for it. Percutaneous commissurotomy (PCT), performed by experienced specialists, is characterized by a low risk of complications. In general, the need for this surgical intervention does not exceed 1%; the proportion of patients in whom this intervention is impossible ranges from 1 to 17%. In case of successful commissurotomy, the area of the atrioventricular opening increases more than 2 times (on average from 0.9 - 1 to 1.9 - 2.4 cm2). The risk of hemopericardium is 0.5 - 7%, embolism - 0.5 - 5%, severe mitral regurgitation - 2 - 19%, hemodynamically insignificant atrial septal defect - 10 - 20%. Other complications (vascular, arrhythmias) are very rare. Immediate improvement is observed when the orifice area increases to 1.5 cm2 or by at least 25% and is manifested by a decrease in pressure in the left atrium, pulmonary artery and a decrease in pulmonary vascular resistance. Long-term 5-year observations showed that the harbingers of an unfavorable outcome are age, an initially high functional class of circulatory failure, the value of vascular resistance of the pulmonary bed, and the area of the atrioventricular orifice after commissurotomy. Indications for PCI are determined by the clinical condition, anatomical changes of the valves and the experience of specialists. Intervention is usually not indicated for patients who do not complain, with the exception of those who require major surgery on other organs, want to give birth to a child, have a high risk of thromboembolism or recurrent supraventricular arrhythmia. The absolute indication for PCI is the impossibility of surgical intervention. It should be preferred in the following cases: with restenosis after surgical commissurotomy; in patients with an increased risk of poor outcome during surgery; in patients with high-grade pulmonary hypertension; in patients with severely impaired left ventricular function; in patients with aortic disease in order to improve their condition before subsequent surgery on both valves; in elderly patients. Anatomical factors that are contraindications for PCI are the following: the presence of a thrombus in the atrium, severe mitral regurgitation, severe aortic heart disease, an atrioventricular orifice area greater than 1.5 cm2. The results are significantly worse if there is valvular calcification. In cases of massive calcification of both leaflets, surgical treatment is preferable. The significant impact of specialist experience on the results of PCCT is demonstrated by data on the frequency of complications depending on the number of procedures performed. For example, if experience is limited to approximately 100 interventions, the need for emergency surgery occurs 4 times more often than if PCI was performed by a specialist who has already performed 1000 procedures. Thus, PCI should be considered as an additional treatment method for patients with mitral stenosis.
Literature:
Vahanian A. Percutaneous mitral comissurotomy. Eur Heart J 1996;17:1465-9.
PERCUTANEOUS TRANSLUMINAL ANGIOPLASTY FOR KAWASAKI DISEASE
S. Berreklouw
A
Orthocoronary artery bypass grafting is the standard therapy for severe coronary artery stenosis associated with Kawasaki disease lesions. Long-term patency of the bypass graft in elderly patients is satisfactory, which cannot be said about young children suffering from this disease. According to previous studies, the short- and long-term patency of saphenous vein grafts after 1 year is 67% and decreases to 55% after 5 to 9 years. Moreover, these shunts have a number of disadvantages: the lumen diameter of native saphenous vein grafts is too small to achieve satisfactory long-term patency in young children, and these shunts have limited ability to expand as the child grows. Currently, shunts from the anterior thoracic artery have found use in coronary artery bypass surgery due to their growth potential. However, the long-term patency of these shunts has not been determined. On the other hand, percutaneous transluminal coronary angioplasty (PTCA) is rarely performed as an alternative treatment for severe coronary stenosis associated with Kawasaki disease lesions. Since 1982, at the institute where T. Ino et al. work, all patients in whom two-dimensional echocardiography reveals a coronary aneurysm or significant dilatation in the acute stage have undergone coronary angiography within 6 months of the onset of Kawasaki disease. As a result, angiographic abnormalities in the coronary arteries were detected in 220 (79%) of 278 patients. The remaining 58 (21%) patients had no visible abnormalities suggestive of coronary aneurysm recurrence or expansion. Of the 220 patients with angiographic abnormalities, 46 had an aneurysm with or without significant stenosis and 174 had dilatation. Ultimately, 5 patients (1 female) aged 2 to 18 years (median 8 years) underwent PTCA for severe coronary artery stenosis. In the acute phase, these patients were diagnosed with Kawasaki disease and were prescribed aspirin and prednisolone (2 patients), aspirin alone (1), aspirin in combination with high doses of gamma globulin (1). There is no information about the treatment prescribed for the fifth patient. All patients received an anticoagulant (aspirin 5–10 mg per day with or without dipyridamole 3–5 mg per day orally) from the time the lesion was first detected until PTCA was performed. The time from the onset of Kawasaki disease to PTCA ranged from 2 to 16 years (median 6 years). Fluoroscopy revealed coronary artery calcification in 2 patients. One patient had three ring-shaped calcifications in the area of three coronary arteries. In another patient, annular calcification was consistent with an aneurysm of the left anterior descending artery. PTCA was considered successful if the degree of stenosis was less than 50% of that before dilatation. Control angiography was performed 6–12 months after the initial one. PTCA was found effective in 4 out of 5 patients. The lesion that was the “target” of PTCA was localized in the middle right coronary artery in 3 patients, and in the proximal left anterior descending artery in 2 patients. In all patients, the stenosis was localized proximal to the aneurysm. PTCA was performed successfully in two right-sided and two left-sided coronary stenoses. In the 4 patients in whom angioplasty was effective, the degree of stenosis decreased from 84 to 33% (p < 0.005). In the fifth patient, who had annular calcification, the percentage of stenosis at PTCA remained unchanged even when the filling pressure was increased to 10 atm. Two-dimensional echocardiography revealed no significant differences in left ventricular wall motion before and after PTCA. 4 patients in whom PTCA was performed successfully underwent control angiography after 6–12 months; the study did not reveal significant restenosis or progression of stenosis. There were no significant complications that could be attributed to the PTCA performed. PTCA was performed in these patients because the stenosis could progress and acute myocardial ischemia could develop after a few years. Criteria for performing PTCA in children with Kawasaki disease, different from those for adults, have yet to be determined. If a pronounced initial thickening is detected, then it is more advisable to use not a conventional angioplasty balloon, but a rotational destructor (rotablator) or an arterectomy catheter. Thus, PTCA can be used as an alternative to coronary artery bypass grafting in patients with coronary artery stenosis due to Kawasaki disease. Conventional PTCA should be performed in patients younger than 8 years of age due to the specific histopathological features of this disease.
Literature:
Ino T, Akimoto K, Ohkubo M, Nishimoto K, Yabuta K, Takaya J, Yamaguchi H. Application of percutaneous transluminal coronary angioplasty to coronary arterial stenosis in Kawasaki disease. Circulation 1996;93:1709-15.