Anemia of pregnancy is a series of anemic conditions that occur during pregnancy, complicate its course and usually disappear soon after childbirth or after its interruption. Since the prevalence of anemia in pregnant women is much higher than in non-pregnant women, it is logical to assume that most of these anemias are associated with pregnancy itself. The classification of anemia of pregnant women in ICD-10 (this is code O 99.0) into a separate section emphasizes the peculiarity of this group of anemias, which lies in the existence of physiological and pathophysiological changes characteristic of pregnancy that contribute to the development of anemia.
The most common consequences of anemia in pregnant women are miscarriages, premature births, intrauterine growth retardation and an increased risk of having low birth weight newborns. The development of anemia in the 1st and 2nd trimesters of pregnancy is associated with a twofold increase in the risk of preterm birth.
Most researchers believe that fetal iron stores are independent of maternal iron levels. The transfer of iron from the mother through the placenta is regulated by the needs of the fetus, occurs even against a concentration gradient, and mainly occurs in the 3rd trimester of pregnancy. This is why the development of iron deficiency is possible only in premature babies.
These adverse effects of anemia in pregnant women are usually associated with hemoglobin levels <90 g/l. With a hemoglobin level of 90-110 g/l in the second half of pregnancy, the prognosis for the woman and child is favorable. At the same time, an increase in Hb concentration above 120 g/l in this period of gestation is fraught with a high risk of complications (in particular preeclampsia).
Any pregnancy leads to an increase in plasma volume, which averages 1250 ml. This is approximately 1.5 times the plasma volume of non-pregnant women. This condition is one of the main reasons for the relative decrease in Hb levels in pregnant women.
Today, the lower limit of normal Hb concentration in pregnant women is considered to be 110 g/l, Hb from 90 to 110 g/l is grade 1 anemia, from 70 to 90 g/l is grade 2 anemia, <70 g/l is anemia 3 tbsp.
According to WHO, 35-75% of pregnant women in the world are diagnosed with anemia every year. In domestic obstetric practice, the prevalence of iron deficiency in pregnant women is considered to be high.
Anemia in pregnant women is multifactorial in nature, and iron deficiency is an important, but not the only, cause of anemia during pregnancy.
FORMS OF ANEMIA.
| Purchased | Hereditary |
| 1. Iron deficiency 2. Posthemorrhagic 3. Folate deficiency 4. Anemia of inflammation 5. Hemolytic 6. Aplastic or hypoplastic | 1. Thalassemia 2. Sickle cell 3. Anemia in other hemoglobinopathies 4. Hemolytic anemias outside of hemoglobinopathies |
The most common types of anemia in pregnant women include iron deficiency anemia (IDA) and folate deficiency anemia, and less common types include aplastic, megaloblastic, hemolytic anemia and thalassemia.
Factors such as frequently recurring bleeding during placenta previa predispose to the development of IDA in pregnant women; anemia that existed in the patient's mother during pregnancy and the patient's prematurity, as well as seasonality and associated changes in food composition (vitamin deficiency in the winter-spring period).
Anemia of inflammation - in recent years, the number of women with urogenital infections (colpitis, cervicitis, bacterial vaginosis, pyelonephritis, etc.) has been increasing, which often occur latently. Moreover, about 30% of pregnant women with urogenital infections approach childbirth in a state of anemia, despite repeated correction with iron supplements. This anemia is defined as “hypochromic anmia without iron deficiency” with normal or increased iron stores in the body.
Complaints of anemia during pregnancy are usually rarely detected, as a rule, in the presence of concomitant pathology. The most typical complaints are weakness, dizziness, increased fatigue, and in more severe cases shortness of breath, anxiety and disturbances of consciousness.
Examination and outpatient treatment of patients with anemia in pregnancy is carried out in accordance with the Order of the Ministry of Health of the Russian Federation dated November 1, 2012. No. 572n.
Outpatient examination:
1) General clinical blood test performed once a month with leukocyte formula, reticulocyte and platelet counts.
2) ECG in each trimester.
3) Biochemical blood test (total protein, serum iron, ferritin, transferrin, total and direct bilirubin).
4) Consultation with a general practitioner (hematologist) and further dynamic observation (1-2 times a month).
5) Clarification of the diagnosis and resolution of the issue of the possibility of continuing pregnancy at a period of up to 10 weeks.
6) Bone marrow puncture (as prescribed by a hematologist).
7) CTG and Doppler in dynamics.
Outpatient treatment:
1) A diet rich in proteins, iron, vitamins and follates.
2) Preparations containing iron (in accordance with the Order of the Government of the Russian Federation of December 26, 2015 N 2724-r, which contains a list of vital and essential drugs for medical use for 2021) - these are oral preparations of 3-valent iron - iron 3 hydroxide polymaltosate (maltofer, fenyuls, ferrum lek). It is not recommended to stop taking iron supplements after normalization of hemoglobin levels.
3) Treatment of the underlying and concomitant diseases.
Indications for hospitalization:
1) Deterioration of the pregnant woman’s condition, lack of effect from outpatient treatment of pregnancy complications.
2) Planned hospitalization for delivery at 38-39 weeks.
Prevention of anemia in pregnant women.
To maintain a normal iron balance during pregnancy, you need to:
1. iron reserves in the woman’s body were adequate at the beginning of pregnancy;
2. The pregnant woman's diet contained sufficient amounts of bioavailable iron to ensure a high level of intestinal absorption in the 2nd half of pregnancy.
The daily iron requirement of a pregnant woman is estimated to be 27 mg. Lower intake levels in women with insufficient iron stores may lead to anemia. Iron absorption is significantly enhanced in the presence of ascorbic acid. Therefore, it is most beneficial to consume foods containing iron in combination with foods fortified with vitamin C.
WHO recommends 60 mg of iron per day for all pregnant women in areas where the prevalence of IDA is less than 20% and 120 mg in areas where it exceeds this value.
Prevention of iron deficiency during pregnancy planning is an ideal form of preventing IDA in pregnant women.
Primary prevention of IDA in pregnant women is aimed at reducing the prevalence of iron deficiency during pregnancy and preventing the adverse consequences for the woman and fetus that it can cause.
Statistical data on the incidence of anemia in pregnant women in the antenatal clinic of the State Budgetary Institution RO “City Clinical Maternity Hospital No. 2” for 3 years.
| Year | Finished pregnancy | Anemia in pregnant women | % |
| 2013 | 1792 | 475 | 26,5 |
| 2014 | 1803 | 382 | 21,2 |
| 2015 | 1782 | 462 | 26 |
Statistical data on the incidence of anemia for 6 months. 2015 and 6 months. 2021
| Finished pregnancy | Anemia in pregnant women | % | |
| 6 months 2015 | 845 | 155 | 18% |
| 6 months 2021 | 1118 | 250 | 22,3% |
If we analyze the given rates of anemia in pregnant women over the past 3 years, we can say the following: in 2013. and in 2015 The percentage of this pathology among pregnant women remained approximately at the same level; in 2014, there was a slight decrease in this indicator to 21.2%.
Management of patients with anemia during pregnancy in residential complex No. 2.
1. We conduct examinations of patients with anemia in pregnant women in accordance with the Order of the Ministry of Health of the Russian Federation dated November 1, 2012. No. 572n.
2. When a diagnosis of anemia in pregnant women is made, the patient is referred for consultation to a general practitioner.
3. For anemia of 2-3 degrees. and uncorrectable anemia 1 tbsp. The woman is referred for a consultation to a hematologist.
4. As part of the Birth Certificate program, we prescribe free oral iron supplements to patients with anemia during pregnancy.
5. In accordance with the order of the Ministry of Health of the Russian Federation dated January 21, 2009. No. 54 “On providing adequate nutrition to pregnant women, nursing mothers, and children under 3 years of age in the Ryazan region” we issue certificates to receive monthly monetary compensation before childbirth for pregnant women diagnosed with stage 2-3 anemia.
In order to prevent anemia in pregnant women during preconception preparation, taking into account the level of initial hemoglobin, patients are prescribed iron supplements.
And also, as part of classes at the “School for Pregnant Women,” women from early stages of pregnancy are taught about the need for a nutritious, balanced diet during pregnancy in order to prevent anemia.
Hemoglobin norms during pregnancy
If in normal conditions the hemoglobin norm for women under 40 years of age is 120-140 g/l, then for expectant mothers the threshold norm values are slightly lower. Hemoglobin levels decrease during pregnancy for natural reasons. Blood volume in women at this time increases by more than 30%. Iron consumption increases as the placenta forms and grows, and the fetal circulatory system forms and develops.
The lower limit of normal hemoglobin during pregnancy is 110 g/l. At a level of 109 g/l, the pregnant woman is already diagnosed with a mild degree of anemia and is prescribed iron supplements.
Hemoglobin in the range of 89-70 g/l indicates moderate anemia, and below 70 g/l - severe anemia. Pregnant women with severe anemia require hospital treatment.
How to increase hemoglobin?
It is believed that you can increase hemoglobin by eating apples and meat. Unfortunately, this is unlikely. A balanced diet with the obligatory inclusion of animal products: red meat, liver, eggs, as well as iron-rich plant foods is indeed the basis for the prevention of anemia. But it is unlikely that it will be possible to cure it only with the help of “correct” food: iron from foods is not completely absorbed, and what is absorbed does not meet the needs of the pregnant woman’s body.
It is important!
In addition, iron from food is absorbed worse if the expectant mother drinks strong tea and coffee, eats chocolate, rice, and corn.
All these products, as well as calcium from milk and fermented milk products, interfere with the absorption of iron. A therapeutic diet is a mandatory step to treat anemia, but it alone will not be enough. Low hemoglobin during pregnancy can lead to serious consequences, as mentioned above.
Therefore, even with a mild degree of anemia, a pregnant woman is prescribed iron supplements in the form of tablets and multivitamins, which help iron to be absorbed. If a woman does not tolerate such drugs well or there is no effect from them, as well as in case of severe anemia, the medicine is administered to her intravenously.
Thus, anemia is a common complication of pregnancy:
- hemoglobin of 109 g/l and below indicates the development of iron deficiency in the expectant mother;
- signs of anemia may be subtle, since they are similar to the symptoms of toxicosis, the diagnosis is made only by the results of a blood test;
- anemia is dangerous for both mother and child; in the worst case, a miscarriage may occur, premature birth may occur, and postpartum hemorrhage may develop;
- hemoglobin is increased with the help of a proper diet, as well as by taking iron supplements: in the form of tablets or intravenously.
(0 ratings; article rating 0)
Share Share Share
How does anemia manifest during pregnancy?
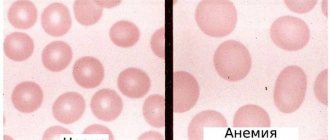
Anemia is a condition in which the number of red cells in the blood decreases - red blood cells, and therefore hemoglobin. The insidiousness of anemia during pregnancy is that its symptoms can easily be mistaken for manifestations of toxicosis: increased fatigue, drowsiness, pale skin, lack of appetite, memory loss, irritability, shortness of breath, sometimes tinnitus - fits perfectly into the picture of pregnancy, doesn’t it? In this case, a mild degree of anemia can be completely asymptomatic.
That is why, to monitor hemoglobin levels, a woman is given a general blood test three times during pregnancy. And if anemia is confirmed, then more often to monitor the dynamics.
Treatment options
During pregnancy, correction of iron protein levels is not always carried out. If the excess of the norm is insignificant, the indicator does not require reduction. Treatment is carried out in case of pronounced clinical symptoms or in the presence of other diseases that affect the state of hemoglobin. All deviations in blood flow are perceived as a symptom of other diseases. To treat pregnant women, gentle methods are used - diet correction, traditional medicine. Medicines are used as a last resort.
Therapeutic diet
A high hemoglobin level is the reason for following a special diet. A woman is recommended to drink a lot of clean water throughout the day. The liquid helps normalize the rheological properties of blood. Red meat and products made from it are excluded from the diet. This is necessary to reduce exogenous sources of iron-containing protein production. Instead, they eat white meat. It contributes to the gradual normalization of hemoglobin levels.
To reduce the concentration of iron-binding protein, adhere to the following recommendations:
- The menu is varied. It includes products containing beneficial microelements, except iron.
- Drink a lot of clean water. The required volume of liquid is calculated at the rate of 30 ml for every 1 kg of body weight.
- Fried and fatty foods are excluded from the menu. The diet is supplemented with fruits and berries.
- Products are boiled or stewed, excluding frying.
If the hemoglobin level is slightly exceeded, a therapeutic diet is sufficient for correction. Gradually, the woman’s condition returns to normal. If symptoms threaten, drug treatment is necessary.
What is anemia?
Anemia in medicine is a decrease in the level of hemoglobin in the blood. Hemoglobin is needed to transport oxygen throughout the body, so when it decreases, the body begins to suffer, the following is observed:
- increased fatigue and weakness;
- insomnia;
- rapid heartbeat and shortness of breath;
- hair loss and brittle nails;
- inflammation and bleeding of gums, etc.
In the early stages, a person may ignore the problem, or explain everything by fatigue or stress. But the matter could be much more serious!
Anemia can be primary (congenital) or acquired. The root cause may be blood loss (including long-term hidden blood loss in small portions, for example, with a peptic ulcer of the stomach or intestines), impaired absorption of iron, and impaired hematopoiesis.