Superficial injuries to the skin and mucous membranes are the most common, with damage to the smallest vessels - capillaries. You need to know how to stop capillary bleeding, since it is not always harmless. Extensive tissue defects can lead to significant blood loss, and proper care and stopping the bleeding will avoid complications associated with it.
Author of the article / Site experts Shulepin Ivan Vladimirovich, traumatologist-orthopedist, highest qualification category
Total work experience over 25 years. In 1994 he graduated from the Moscow Institute of Medical and Social Rehabilitation, in 1997 he completed a residency in the specialty “Traumatology and Orthopedics” at the Central Research Institute of Traumatology and Orthopedics named after. N.N. Prifova.
Signs of capillary bleeding
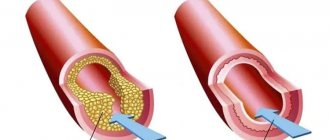
Capillaries are the most numerous and smallest blood vessels. They are located between arterioles and venules, connecting them, and also form multiple branching networks adjacent to tissue cells. Arterial blood, saturated with oxygen, flows through the capillaries, and it is released through the thinnest walls to the cells of tissues and organs. The speed of blood flow in the capillaries is extremely low (about 1 mm/sec), its movement is uniform, not pulsating.
These properties of capillaries determine the signs of bleeding when they rupture:
- the entire damaged surface bleeds;
- blood is bright scarlet;
- There is no pulsation, the blood flows out evenly.
Damage to capillaries always occurs with any injury due to their large number. The most typical examples: if you cut your finger shallowly, as well as abrasions, bruises and hematomas after bruises, hemorrhages under the membranes of the eyes, bleeding from the nose and gums.
Bleeding is divided into types according to the damaged vessel and is distinguished:
· Arterial, which occurs when an artery is damaged and is characterized by a pulsating and flowing outflow of scarlet blood
· Venous, characterized by a smooth flow of blood of a dark red color, occurring with deep tissue damage
Capillary or scarlet bleeding throughout the wound, which is observed when small vessels are damaged
· Parenchymal, characteristic of injury to the liver, spleen or lung. With such bleeding, scarlet and dark red blood is released simultaneously throughout the wound
· Mixed, which is characterized by a combination of different types of bleeding: capillary and venous, arterial and venous, etc.
Depending on the nature of the damage, external bleeding is also distinguished, that is, flowing outward, and internal, when the bleeding itself is not visible, and the blood flows into the abdominal cavity.
Possible complications and consequences
Most capillary bleeding is characterized by insignificant blood loss, its spontaneous, rapid stop and a good prognosis. They can be dangerous in case of large blood losses, because the amount of arterial blood carrying oxygen decreases. Hypoxia develops - oxygen starvation of tissues, which can lead to dysfunction of all organs and systems.
The following reasons can lead to such consequences:
- extensive wound surfaces - scalped skin wounds, mucous membrane defects, extensive burns;
- decreased blood clotting (hemophilia, thrombocytopenia);
- oncological diseases;
- high blood pressure;
- vascular diseases.
There are also bleedings from the capillaries of internal organs - lungs, gastrointestinal tract, kidneys, uterus, they are extremely dangerous.
Diagnosis of bleeding
Diagnosis of external bleeding is not difficult. With arterial bleeding, the blood is scarlet and flows out in a pulsating stream. With venous bleeding, the blood is dark and flows evenly. With capillary bleeding, it is released in the form of “dew” or small drops.
Difficulties may arise when recognizing internal bleeding.
Depending on the intensity of bleeding, it can manifest itself in two main syndromes: acute blood loss syndrome and chronic anemia syndrome.
With rapid blood loss, acute blood loss syndrome occurs. It manifests itself with weakness, sweating, pallor of the skin and mucous membranes. Patients' blood pressure decreases and tachycardia occurs. In blood tests, hemoglobin and hematocrit decrease. In acute blood loss, a decrease in hemoglobin below 80 g/l and hematocrit below 25% can lead to death.
Chronic blood loss can occur with heavy menstruation, hemorrhoidal bleeding, disintegrating tumors of the colon or stomach, etc. With chronic blood loss, the symptoms are more smoothed out, because the body has time to adapt to it. Patients complain of weakness and increased fatigue. The skin is pale, hair and nails become brittle. Hemoglobin can drop significantly, below 60 and even 40 g/l, with the patient’s condition being relatively satisfactory and blood pressure levels stable. The diagnosis is helped by additional laboratory and instrumental research methods - endoscopy, colonoscopy, bronchoscopy, stool examination for occult blood, etc.
First aid
First aid for bleeding from the capillaries plays a big role; it can not only reduce it, but also stop it completely. The main task is to compress the blood vessels, and the technique depends on what part of the body the damage is located in. In some cases, a tight pressure bandage is enough, while in others it is impossible to do without applying a tourniquet.
Pressure bandage
Applying a bandage is effective when the bleeding is not very intense, and it is possible to apply pressure to the area of damage: on the head, limbs, torso. First, the wound is treated with hydrogen peroxide, the skin around it is treated with 5% tincture of iodine, a sterile gauze bandage is applied, and it is tightly bandaged. For greater compression, a fabric roller is placed on the bandage. If the bandage stops soaking, the bleeding has stopped.
Applying a compressive tourniquet
A tourniquet may be needed if there is heavy bleeding in various areas of the extremities, when it cannot be stopped with a pressure bandage. It is applied in the middle of the thigh or shoulder above the level of the wound, after wrapping the limb with cloth. The tourniquet is pulled and secured, a note is placed under it indicating the time of application, and the victim is transported to the hospital.
When a tourniquet is not at hand, a strip of thick fabric, a belt, a belt, a tie, a scarf, or a rope will also do. Having wrapped the limb, they make a loop, insert a small stick into it and make a “twist”, which is rotated, increasing the compression.
You can also use this method: bend your leg or arm all the way in the joint located above the bleeding site, after first placing a tight roller on its flexion surface, and fix it well. The wound must be covered with a sterile bandage and bandaged tightly.
Treatment of bleeding
In acute blood loss, the first priority is to stop the bleeding. In this case, a distinction is made between a temporary stop and a final one. Temporary stopping of bleeding includes digital compression of the vessel, application of a hemostatic tourniquet, application of a medical clamp to the bleeding vessel, and a pressure bandage.
Definitive methods of stopping bleeding include ligation of the vessel (in the wound or throughout), application of a vascular suture, and electrocoagulation.
In some cases, temporary methods of stopping bleeding can become permanent (such as a pressure bandage for venous bleeding).
In case of massive blood loss, simultaneously with stopping the bleeding, correction of hemodynamic and water-electrolyte disturbances is carried out - transfusion of plasma-substituting solutions, plasma, red blood cells, administration of drugs that correct blood clotting.
In case of chronic blood loss, along with identifying the source of bleeding and its elimination, correction of blood quality indicators is carried out (prescription of iron supplements, in some cases - transfusion of red blood cells).
Nose bleed
Nosebleeds appear quite often in everyday life and at work. They occur due to rupture of the capillaries of the mucous membrane due to injury, overheating, increased pressure, prolonged stay in a downward position, as well as rhinovirus infections and various internal diseases (vascular, blood, endocrine system).
It’s easy to stop it by following the following algorithm:
- make the patient sit down;
- tilt his head slightly forward;
- firmly hold your nose between your index finger and thumb;
- Apply cold to the bridge of the nose.
If the bleeding cannot be stopped, tamponade must be performed. Moisten strips of a wide gauze bandage with 3% hydrogen peroxide and tightly move one, then the other, nasal passages with them, apply cold to the bridge of the nose.
You cannot lay the patient down or tilt his head back, because blood may flow into the larynx and asphyxia (suffocation).
If the blood continues to flow, you need to go to an ambulance, and then visit a doctor for examination and treatment, if necessary.
First aid for venous bleeding
Blood clots that are bleeding from a vein should not be removed, as this may cause even greater blood loss. As first aid, apply a pressure aseptic bandage made of a strong bandage or fabric. If this method is ineffective, it is recommended to use a tourniquet. Under it, in order to avoid unwanted injury to the skin, there should be cotton wool or other soft material and a note with the time of application. The maximum duration of stay of the tourniquet on the victim’s body is 1 hour in the cold season (winter, autumn) and 2 hours in the warm season. If this time frame is exceeded, there is a risk of tissue anesthesia. Instead of a tourniquet, you can use various available materials - tight belts, ties, short sticks with fabric, twisted towels, etc.
Thrombosis
It must be remembered that no matter what method of stopping bleeding was used, thrombosis processes occur in the body, which should themselves lead to blockage of damaged vessels. In order not to damage the resulting blood clot or dislodge it, it is recommended to immobilize the wounded limb. The most effective in this sense is splinting. Ideally, if it is possible to use an inflatable splint, it will also reduce bleeding by compressing the blood vessels. But usually you have to make do with an improvised tire made from scrap materials. And, of course, the victim should be taken to a doctor. Even if the bleeding has already stopped, observation by a surgeon is still necessary. The fact is that once bleeding has stopped, it can resume - these are so-called secondary bleedings. This occurs due to the destruction or displacement of a blood clot or due to its melting during suppuration of the wound.
Method for stopping capillary and parenchymal bleeding
The invention relates to surgery and is intended to stop capillary and parenchymal bleeding. Capillary and parenchymal bleeding is stopped by applying supratonal frequency currents to the area of this bleeding. The method allows to increase the effectiveness of stopping capillary and parenchymal bleeding. 3 ill., 1 tab.
The present invention relates to medicine and can be used in various areas of surgery to stop capillary and parenchymal bleeding.
It is known that the search for the optimal tool for ensuring hemostasis during the dissection of biological tissues has been ongoing since the end of the 19th century, when electrocoagulation was invented. However, almost irreparable side effects of this method were quickly identified, the main of which is a large area of tissue damage in the area of application. In the 60-70s of our century, plasma flows and laser radiation began to be used to ensure hemostasis during tissue dissection. Plasma scalpels and coagulators, using various working fluids (argon, helium, hydrogen), provide dissection and coagulation of tissue by achieving a very high temperature of the plasma flow and laser beam. It has been established that plasma flows are most appropriate to use in surgery of parenchymal organs - primarily liver [1]. However, the use of complexes operating on the basis of plasma flows has its drawbacks: the complexity of operating the complex; the need to cool the plasma torch with running water with a high degree of purification; the need for power supply from a 380 V network; filling cylinders with a scarce working fluid - argon. Currently, in surgery, to ensure tissue hemostasis, laser radiation generated by various types of laser scalpels - CO2, YAG-neodymium, etc. is widely used. [2]. Their undoubted advantages include: simultaneous dissection and coagulation of blood and lymphatic vessels with a laser beam; relatively small area of thermal tissue damage; the non-contact nature of the instrument, which is especially important due to the relevance of the problem of HIV infections. We adopted as a prototype a method of hemostasis using laser radiation, which consists of using a laser scalpel [3]. The method allows you to quickly and effectively stop capillary and parenchymal bleeding by achieving a very high temperature in the bleeding area. The disadvantages of the prototype include: the bulkiness of the equipment and the need to equip a special operating room; high cost of equipment; need for water cooling; low degree of mobility of the light guide for a CO2 laser; a fairly large area of thermal damage to tissue. The purpose of the invention: to ensure reliable hemostasis during capillary and parenchymal bleeding. Objectives: to achieve reliable hemostasis with minimal thermal damage to surrounding tissues. The essence of the invention: the effect of hemostasis is achieved by exposing the bleeding area to supra-tonal frequency currents (TSF), which leads to the formation of ozone in the affected area, providing a hemostatic effect. Description: To obtain ozone in the hemostasis area, the principle of a barrier discharge in an oxygen flow is used. In this case, high voltage alternating current is supplied to two electrodes separated by a gas-discharge space. When oxygen is present in the discharge zone, ozone is formed. The ozone concentration is regulated by changing the voltage supplied to the alternating current electrodes. Hemostasis is ensured, for example, using the Ultraton-M-AMP apparatus with a set of modified glass electrodes [4]. The method is intended for bleeding from small-diameter vessels. When using the proposed method, the multicomponent effects of ozone on biological systems should be taken into account. When ozone is administered at therapeutic concentrations, free radical lipid peroxidation is not stimulated; an increase in oxygen tension in the peripheral blood and stimulation of a number of aerobic oxidation enzyme systems in erythrocytes and ischemic tissues are noted [5]. The direct effect of ozone and its derivatives on under-oxidized products of tissue metabolism during chronic hypoxia (lactate, pyruvate, acetaldehyde, urea, creatinine, toxic lipids, medium molecular compounds) contributes to their rapid utilization. The use of ozone during hypoxia restores the microcirculation system in ischemic tissues. As studies have shown [6], ozonation has a pronounced antimicrobial effect against blue-green pus sticks, as well as anaerobic bacteria. When analyzing the results of the clinical use of ozone therapy, a potentiation of the effect of antimicrobial drugs was noted, which in some observations made it possible to restore the sensitivity of microflora to previously ineffective antibiotics. In addition to its antimicrobial properties, ozone has an immunostimulating effect. Under the influence of ozone therapy, the number of circulating neutrophils significantly increases, plasma toxicity decreases, the biocidal potential of the blood increases, the production of formed elements by the bone marrow is stimulated, mainly the humoral component of immunity and especially the phagocytic activity of neutrophils. In addition, ozone causes a significant decrease in the concentration of mediators of tissue damage - cytokines [7]. The method is carried out as follows. If bleeding occurs from biological tissues (skin, subcutaneous fat, liver parenchyma, etc.) during surgical manipulations, a glass electrode is placed over the bleeding area with a gap of 1-2 mm between the instrument and the tissues (for this purpose, a sterile gauze napkin in 1-2 layers) and achieve the occurrence of a corona discharge with the following parameters of the device - the effective value of the output voltage is 2.50.3 kV, the frequency of the sinusoidal output voltage is 223 kHz. To completely stop bleeding, the exposure is usually 7-10 seconds. The main factors leading to hemostasis with this method are: sinusoidal high-frequency current, high-voltage corona discharge, ozone, heat released in the tissues of the body and in the area of corona discharge. Results of the research. The proposed method of hemostasis was tested in experiments in vitro, in vivo and in the clinic. A preliminary series of experiments (N=31) was carried out on the blood of healthy donors, from whom two blood samples were taken from the cubital vein in the morning (800-900) on an empty stomach. The blood was placed in cuvettes of 2 calibrated N-334 electrocoagulographs. One of the samples served as a control, the other was treated with ultratone with an exposure of 15 seconds and a gap between the electrode and the blood sample of 1-1.5 mm (effective output voltage value 2.50.3 kV, frequency of sinusoidal output voltage 223 kHz). After completion of the treatment, electrocoagulograms of both samples were recorded using standard methods. The blood coagulation system was assessed using an N-334 electrocoagulograph according to the method of N.A. Vetlitskaya (1990) [8]. When deciphering electrocoagulograms, the following parameters were determined: 1. Tsv - coagulation time. This is the time from the beginning of the study to the first pulse with minimum amplitude.2. TRF is the time of onset of retraction and fibrinolysis. This is the time from the beginning of the study to the first pulse with increased amplitude following the end of coagulation.3. Am - maximum amplitude, depends on the hematocrit value and corresponds to the liquid state of blood.4. Ao is the minimum amplitude, depends on the degree of density of the clot and reflects the interaction of two systems: coagulation and anticoagulation.5. Arf - amplitude of retraction and fibrinolysis, depends on the degree of retraction and fibrinolysis at a given time, usually determined 10 minutes after the start of this process. It is used to judge the amount of fluid released as a result of clot retraction and fibrinolysis.6. Tps is the lifetime of a dense clot. This is the time from the first pulse with minimal amplitude to the first pulse with increased amplitude of the next one after the end of coagulation.7. SC - degree of coagulation, calculated by the formula: The indicator takes into account the difference between the liquid and coagulated parts of the blood and makes it possible to judge how much liquid blood has coagulated.8. KA is the coagulating activity of the blood, determined by the formula: KA is a sensitive indicator that takes into account all coagulation factors. When calculating, both the density of the clot and the rate of its formation are taken into account. CA characterizes the level of coagulation and quickly responds to developing hypercoagulability or consumption coagulopathy.9. SF—degree of fibrinolysis. The indicator shows what percentage of coagulated blood is subject to retraction and fibrinolysis, determined by the formula: where the difference between the liquid and coagulated parts of the blood and between the coagulated and the part of the blood that has undergone retraction and fibrinolysis is taken into account.10. AF is the fibrinolytic potential of the blood, determined by the formula: The indicator includes not only fibrinolysis, but also retraction, however, it fairly objectively reflects the fibrinolytic potential. FP, calculated according to the proposed formula, takes into account both the strength of the clot, the rate of its lysis, and the amount of lysed fibrin over the studied period of time. 11. GP - hemostatic potential, is determined by the formula: Hemostatic potential is the end result of the interaction of two systems: coagulation and anticoagulation, as a result of which the blood remains liquid. Of the 11 main parameters, from our point of view, only the most informative ones were selected: coagulation time (TCv) , coagulation activity (CA) and degree of coagulation (DC), reflecting the coagulation link of the hemostasis system; fibrinolytic potential (FP) and degree of fibrinolysis (DF) - fibrinolytic link; hemostatic potential (HP) is an integral indicator reflecting the ratio of the coagulation and anticoagulation systems of the blood. The results of the studies are presented in the table and figures 1, 2. As preliminary studies have shown, ultraton significantly activated the blood coagulation system with simultaneous inhibition of fibrinolysis. Further studies were carried out in an in vivo experiment on 11 mongrel dogs that underwent cholecystectomy. Ultrasound hemostasis was carried out when making a laparotomy wound, as well as for hemostasis of the gallbladder bed. Satisfactory results were obtained with minimal thermal damage to the treated tissues. No side effects were noted. And finally, the method was tested in the clinic on 48 patients (18 patients for hemostasis of the gallbladder bed when performing cholecystectomy, 30 patients when performing various surgical procedures on soft tissues (primary surgical treatment of wounds, opening of abscesses, phlegmons, etc.)), where satisfactory results were also obtained. For a comparative assessment of the degree of thermal damage to the liver when stopping bleeding from the gallbladder bed using electrocoagulation and ultraton in 18 patients after cholecystectomy, the activity of glutamate dehydrogenase in the blood serum was studied (GlDH) is an enzyme marker of hepatocyte damage (Fig. 3). Enzyme activity was determined by the change in extinction (E) of NADH2 at 340 nm per unit time. β-ketoglutorate and ammonium salts were used as a substrate. The method is based on spectrophotometric measurement of GLDG activity using the optical Warburg method. As studies have shown, patients using electrocoagulation experienced a significant increase in GLDG activity, especially on the 5-7th day of the postoperative period. During this period, the inflammatory reaction in the liver burn area moves from the alteration phase followed by necrosis into the regeneration phase, accompanied by activation of lysosomal enzymes and rejection of the necrosis area. During this period, against the background of uncompensated tissue hypoxia, the activity of the processes of the tricarboxylic acid cycle and the concentration of its substrates decrease. Competitive relationships arise between labilizers and stabilizers of lysosomal membranes; against the background of increasing decompensation, membrane permeability becomes sufficient for hydrolases to enter the cytoplasm and interact with the substrate, which can also be subcellular structures. The permeability of cytoplasmic membranes for macromolecules (proteins, enzymes) increases with their massive release into the bloodstream, which leads to hyperenzymemia. As the body is freed from necrotically altered tissues, the inflammatory reaction subsides, GLDG activity begins to decrease and by the end of the observation period (8th day) approaches the initial values. In the experimental group, where ultratone was used for hemostasis, such pronounced hyperenzymemia was not observed. The maximum value of GLDG was noted on the 6th day of the postoperative period (4.380.94 mmkmol/mlmin), which is 3.8 times higher than the norm (in the control group this figure was 31.293.5 mmkmol/mlmin, which is 27.8 times higher than the norm ).Example. Patient V., 25 years old, (case history 3170) was admitted for treatment to the Krasnodar Clinical Department Hospital of the North Caucasus Railway on August 11, 1997 with a diagnosis of cholelithiasis. Stricture of the terminal part of the common bile duct. Mechanical jaundice. Chronic calculous cholecystitis in the acute stage. On August 13, 1997, an unsuccessful attempt at endoscopic papillosphincterotomy was made at the Regional Diagnostic Center - it was not possible to penetrate the large duodenal papilla due to the stricture of the terminal part of the common bile duct. On August 15, 1997, an operation was performed: cholecystectomy, transduodenal papillosphincterotomy, sphincteroplasty, drainage of the common bile duct according to Pikovsky. During the operation, moderate bleeding was observed from the gallbladder bed, which was effectively stopped by using the Ultraton installation. The postoperative period was without complications, the patient was discharged in satisfactory condition for outpatient treatment. Thus, stopping capillary and parenchymal bleeding using ultraton allows one to achieve complete hemostasis with minimal thermal damage to surrounding tissues. One of the advantages of the proposed method is also its bactericidal, immunostimulating and anti-inflammatory effect due to the production of ozone, which allows, in parallel with hemostasis, the prevention of postoperative purulent complications. Due to the portability of the installation and ease of operation, the method is publicly available and can be widely used in clinical practice. References: 1. Andreev A.L., Rybin E.P., Uchvatkin V.G. and others. The first experience of using a plasma scalpel in laparoscopic operations. - Mat. VIII All-Russian Congress of Surgeons (abstracts of reports). - Krasnodar. 1995.-P.322-323.2. Kalish Yu.I., Madartov K.M., Khusainov B.R. Principles of the combined use of lasers in the prevention of purulent-inflammatory postoperative complications in abdominal surgery. - Mat. VIII All-Russian Congress of Surgeons (abstracts of reports). - Krasnodar. 1995.- P.490-491.3. Skobelkin OK, Brekhov E.I., Korepanov V.I. Use of laser in surgery. - Surgery. 1983.- 3.-From 15-18.4. The device is recommended for use in medical practice by the commission on new technology of the Ministry of Health of the Russian Federation (protocol 3 of March 15, 1993) and was developed by JSC NPAP Altaymedpribor (Biysk) together with JSC Intelmed. The device is intended for carrying out physiotherapeutic procedures such as local darsonvalization and called ultratonotherapy.5. Kontorschikova K.N. Hypoxia and oxidative processes // Ozone in biology and medicine N. Novgorod. 1992. pp. 50-54.6. Glukhov A.A., Glyantsev V.P., Moshurov I.P. Application of new technologies in the treatment of wound processes // Voronezh Regional Clinical Hospital: specialized medical care: Sat. scientific articles. Voronezh. 1996. pp. 360-364.7. Delvin RB Mckinnon KL, Noah Tel al. // Amcr J. physiol, 1994.- Vol 266.- No 6 Pt. I.-P 1612-1619.8. Vetlitskaya N.A., Levanovich V.V., Engibadze Yu.G., Mamatsashvili V.E. Diagnosis, prevention and treatment of acute coagulopathies in children, methodological recommendations // Tbilisi, 1990, - 20 p.
Claim
A method for stopping capillary and parenchymal bleeding, including a thermal effect on a bleeding vessel, characterized in that the bleeding area is exposed to supra-tonal frequency currents.
DRAWINGS
,
,
,
Internal bleeding
And finally, a few words about internal bleeding. They manifest themselves as hemoptysis, bloody vomiting, blood in the stool, and bloody vaginal discharge. It should be remembered that the blood, under the influence of hydrochloric acid in the stomach, turns black, and signs of bleeding can also include black vomit (the so-called “coffee grounds”) and loose black stools. Generally speaking, it is impossible to stop internal bleeding at the prehospital stage. In such cases, you should immediately call an ambulance. And before the doctors arrive, it is necessary to provide the patient with peace, if possible, to put him to bed. In case of hemoptysis or bloody vomiting, the patient should be given very cold water to drink in small sips and small pieces of ice to be swallowed. You can put ice on the sternum for hemoptysis, in the left hypochondrium for hematemesis, on the anus for heavy hemorrhoidal bleeding, and on the lower abdomen for vaginal discharge. A belt that is too tight should be loosened.
Many people tend to be scared by the sight of blood. In addition, spilled blood has this peculiarity - it always seems to be more than it is; 200-300 ml of blood on clothes and on the floor visually gives the impression of “bloody puddles”. But if you don’t panic, but act clearly and quickly, then in most cases it’s not so difficult to help.
What are the risks of blood loss?
During the Great Patriotic War, a third (and according to some sources, half) of those killed on the battlefield died from blood loss. And in our time, untimely stopping of bleeding is one of the main causes of death in road accidents. And there is not much time allotted to provide assistance. If large arteries are injured - carotid or femoral - a person can die from blood loss within 10-15 minutes.
Blood loss in a volume of up to 500 ml usually does not cause significant disruptions in vital functions; at this stage, the body’s compensatory capabilities are sufficient. But the loss of 1 liter of blood already leads to severe circulatory disorders, and blood loss of 2 liters or more poses a real threat to life. However, these figures are approximate. The severity of the lesion depends on the initial condition of the victim - cold, hunger and fatigue worsen the prognosis. Children and old people endure blood loss more severely than young people, men more severely than women. The combination of painful shock and blood loss significantly aggravates the victim's condition. The rate of blood loss also matters. When large vessels are damaged, when blood is lost very quickly, death sometimes occurs with the loss of 1 liter of blood or even less, since in such cases compensatory mechanisms do not have time to turn on.