What is D-dimer
D-dimer is the part of the protein that remains after the blood clot breaks down. It is a breakdown product of fibrin, the fibers of which form a blood clot. D-dimer consists of two D-particles of fibrinogen contained in blood plasma.
The amount of D-dimer in the blood can be determined using a test. If this indicator is excessively high, then the patient has a high risk of thrombosis.
This analysis is not included in the mandatory laboratory tests. It is prescribed only to those who are at risk for thrombosis.
Decoding the results
Increased D-dimer levels
When the level of D-dimer in the blood increases, it is necessary to search for a probable cause, since some conditions accompanied by an increase in its concentration require immediate medical attention.
An increased level of D-dimer as a physiological norm occurs in old age (after eighty years), as well as during pregnancy (gradually increasing in proportion to the gestational age).
- Outside of pregnancy, a high D-dimer may indicate the presence of thrombosis in the veins or arteries. This is usually accompanied by complaints characteristic of thrombosis (pain in the limb, swelling, redness or pallor) or thromboembolism (shortness of breath, chest pain, hemoptysis). In this case, help must be urgent. But in approximately 20-30% of cases, thrombosis is asymptomatic. In this case, your doctor will help you draw up an examination plan and decide on tactics.
- D-dimer often increases in people suffering from obesity, autoimmune diseases (rheumatoid arthritis, systemic lupus erythematosus, etc.), as well as liver disease and cancer. In this case, the increase is most likely secondary, and if there are no signs of thrombosis, observation by your doctor is sufficient.
- Often, D-dimer is elevated in older people (also without signs of thrombosis). Prescribing thinning drugs in this situation is not always necessary, since the risk of bleeding must also be taken into account.
- Since D-dimers are breakdown products of already formed blood clots, their concentration may increase after bleeding or during the period of hematoma resorption.
- The most difficult thing to interpret is the increase in D-dimer due to thrombosis during pregnancy. The same level of D-dimer can be observed both in a patient with thrombosis and in a healthy pregnant woman. Therefore, complaints and the likelihood of thrombosis (the degree of risk, which is calculated on a special scale) are always assessed in parallel.
Normal D-dimer levels
A normal test result indicates that the patient is not at risk of thrombosis. However, in rare cases (no more than 2 per hundred) in the presence of thrombosis, the level of D-dimer remains normal. As a rule, this is due either to the very small size of the blood clot, or to improper storage of the material for the study. Thus, the diagnostic value of the D-dimer test is quite high (98%) and allows its active use to exclude the process of thrombus formation.
Low D-dimer levels
A low D-dimer should not be a concern. If the value is below the lower limit (although most laboratories indicate only the upper limit, which is correct), this can reliably indicate only one thing: you definitely do not have thrombosis.
It makes no difference whether to take a D-dimer test before or after taking thinning drugs, since this indicator is cumulative and reflects the activity of the coagulation and anticoagulation systems retrospectively.
What does D-dimer show in a blood test?
A blood test for D-dimer (also called dedimer) shows whether there are small blood clots in the bloodstream. These clots can clog blood vessels and cause life-threatening conditions:
- deep vein thrombosis;
- heart attack;
- stroke;
- pulmonary embolism.
To assess the risk of such serious diseases, doctors prescribe patients to do a D-dimer test.
Blood from a vein is donated on an empty stomach in the morning. You must not eat 8 hours or smoke 2 hours before the test. You are allowed to drink only water; tea, coffee, juices and other drinks, especially sweetened ones, should be avoided. The result is ready within 2 days.
Sports and medicine
It has been established that among marathon athletes, increased levels of inflammatory and hemostatic markers of cardiovascular risk increase the likelihood of developing acute coronary pathology. There was a twofold increase in the levels of CRP, von Willebrandt factor, D-dimer, leukocyte count, and fibrinolytic activity, which persisted for 4 hours after the end of the competition. The level of fibrinogen decreased immediately after stopping running, but the content of its breakdown product, D-dimer, increased. Consequently, blood clots formed, although this was not clinically evident.
D-dimer: what kind of analysis is it?
Checking the condition of the blood and the possible presence of clots in it is carried out using a blood test. There are two types of tests:
- Quantitative - reveals whether the D-dimer level is elevated or within the normal range. The results show o (increased) or “no” (normal).
- Qualitative - the exact number of D-dimer is indicated in numbers.
Quantitative analysis is more informative and provides doctors with more information about the condition of the patient's bloodstream. During the treatment of hemostasis, the analysis is carried out several times. If the indicator decreases, it means that the blood clot is dissolving and the patient is recovering. But high-quality analysis is cheaper and therefore more accessible to patients.
The test result will allow the doctor to accurately determine the risk of cardiovascular and cancer diseases in a particular patient.
Orthopedics and traumatology for the elderly
Elderly individuals (over 60 years of age) are characterized by changes in the ratio of coagulation, anticoagulation and fibrinolytic systems. Most often they are expressed by shifts towards hypercoagulation. Such patients pose a great risk in terms of endoprosthetics of large joints. In all groups of patients after hip replacement surgery during anticoagulant therapy, the data obtained indicate the development of changes towards hypercoagulation.
Assessment of plasma D-dimer level is one of the sensitive and informative tests for determining the degree of risk of developing thrombotic complications and the effectiveness of anticoagulant therapy.
Indications for analysis
Doctors order a D-dimer blood test for a variety of symptoms and medical history. The test result will allow you to monitor the patient’s condition and prescribe appropriate treatment.
List of indications:
- tendency to thrombosis, disseminated intravascular coagulation syndrome;
- chest pain;
- rapid heartbeat;
- sudden shortness of breath, breathing problems;
- hemoptysis;
- cough;
- cyanosis of the skin and mucous membranes;
- abdominal pain, nausea, vomiting;
- muscle pain;
- sharp pain in the leg or arm;
- change in color of an arm or leg (pallor, blueness, blackening);
- swelling of the limb;
- varicose veins of the legs;
- decrease in daily urine output;
- bleeding from gums;
- pregnancy;
- after injury;
- coronavirus infection COVID-19;
- control during treatment with anticoagulants.
During pregnancy, the risk of blood clots increases, so to monitor a woman’s health, she periodically undergoes a D-dimer test.
With these diseases and conditions, the patient should carefully monitor his well-being and consult a doctor in case of any ailments.
Content
- Problems caused by thromboembolism
- Normal d-dimer values
- Causes of increased d-dimer levels
- Interpretation of tests for d-dimer
Blood clotting is a complex process, the purpose of which is to protect a living organism from blood loss.
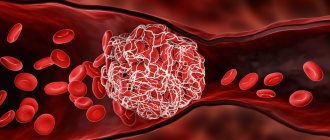
In the event of damage to a blood vessel, a primary thrombus, a blood clot that closes the damage, forms on average within 3 minutes. A blood clot consists of a polymer protein called fibrin and blood cells: red blood cells, platelets and white blood cells. Fibrin is formed from fibrinogen under the action of a substance called thrombin. Once thrombin acts on fibrinogen dissolved in the blood, it turns into insoluble fibrin. Fibrin thickens the blood at the site of injury, platelets and other cells settle on it. After 10 minutes, the clot thickens - this process is called retraction. The bleeding has stopped.
It would seem like an ideal mechanism. But every mechanism can have problems. Sometimes blood clots form in the lumen of intact vessels. If such a clot gets into the arteries, blood circulation may be impaired. Impaired circulation will lead to ischemia and tissue death. This is how thromboembolism develops, a condition in which blood clots enter the arteries of vital organs.
What should the normal indicator be?
The normal level of D-dimer in blood plasma is 250 ng/ml. this indicator confirms that the patient is not at risk of thrombosis. In pregnant women, this figure can reach 1000 ng/ml or more, i.e. grow 3–4 times.
Normal D-dimer levels in pregnant women:
- up to 450–500 ng/ml in the 1st trimester;
- up to 900–920 ng/ml in the 2nd trimester;
- up to 1450–1500 ng/ml in the 3rd trimester.
If a pregnant woman, on the contrary, has a low level, she is urgently referred to a hematologist, who will prescribe medications. A decrease in dedimer during pregnancy is a sign of long-standing problems with blood clotting that arose long before pregnancy. With good treatment, childbirth proceeds normally.
Rumyantseva, md.
This article was written based on materials from a lecture and article by phlebologist Evgeniy Ilyukhin; the original article can be found at the link.
This article deals with a complex topic, but its relevance is growing, as is the level of panic around high D-dimer levels during pregnancy. So, let's try to figure it out:
- what is D-dimer,
- what are its normal values during pregnancy,
- who needs to be tested for it,
- in what situations treatment is required.
What is D-dimer?
More precisely, D-dimers.
D-dimers are fragments of fibrin that breaks down, which, in turn, is the basis for the formation of blood clots. In the blood coagulation system, the formation and splitting of fibrin threads constantly occurs, and an increase in the level of D-dimer indirectly indicates a potentially increasing possibility of thrombus formation (at least, this is how an increase in the level of D-dimer is interpreted when prescribing therapy during pregnancy). During pregnancy, the level of D-dimer in the blood increases, and of course, everyone is concerned with the question of what increase can be considered normal, and when is it time to start sounding the alarm and take active action?
Why is everyone so afraid of “blood clotting” during pregnancy?
Fear is associated with an increased risk of venous thromboembolic complications (VTEC) in principle during pregnancy and the postpartum period, in the context of which D-dimer is considered. Deep vein thrombosis and pulmonary embolism (common name - VTEC) during pregnancy are not a horror story, but very real serious pathologies that can lead to the most severe consequences, including death, in a pregnant woman/who has recently given birth. VTE occurs with a frequency of 1.9 cases per 1000 pregnancies! Experts know that the postpartum period is more dangerous than the pregnancy period in terms of the development of VTEC.
All that remains is to figure out whether it is possible to equate the increasing level (and which one) of D-dimer and the risk of VTEC.
D-Dimer Level Units
When talking about D-dimer, we are talking about its concentration, or rather about their concentration (D-dimers). That is, the weight of D-dimers in a certain volume. Accordingly, these can be any units of weight and any units of volume. And any “combinations” of them. Usually weight is indicated in ng, mg, mcg. Volume: in ml or l. Accordingly, you can see the following entry:
300 ng/ml = 300 µg/l = 0.3 µg/ml = 3.0 mg/l
There are also "D-Dimer Units", DDU, and "Fibrinogen Equivalent Units", FEU. The difference is simple, 1 FEU mass = ½ DDU. So 600 ngFEU/ml = 300 ngDDU/ml.
In total, from the many options for units of measurement, we have the following correspondences:
300 ng/ml = 300 μg/L = 3.0 mg/L = 0.3 μg/ml = 600 ng FEU/ml = 600 μg FEU/L = 0.6 μg FEU/ml
As you can see, there are many options for units of measurement, so you need to be very careful when comparing results obtained at different times in different laboratories.
There is another bottleneck in determining D-dimer levels: different tests have different sensitivity and reproducibility.
This means that if we measure the D-dimer level (in the same units!) with different devices in the same patients, we will get different values with a very large scatter! That is, we can trust the obtained values only with a very large assumption.
What are normal D-dimer levels during pregnancy?
Are there normal D-dimer levels for pregnant women?
If you search on the Internet, you can find a huge number of resources with tables of norms by trimester. Particularly credible is the fact that such signs are on the websites of large laboratory networks. The only problem is that even in large laboratories, the norms for D-dimer during pregnancy differ by 2 times (in the same units of measurement!). Who to believe? Let's see what major international studies say about this.
It turns out that there can be no talk of any reference values for the D-dimer level.
The main reasons for this are as follows:
1) Different tests give a colossal spread of values. In different tests in the first trimester, D-dimer values differ by 2 times, and at week 36 - by 5 times!
2) Figures for the concentration of D-dimers during a normal pregnancy can significantly exceed the pseudonorms that are replete with the Internet and which are given in completely official laboratory forms (for example, studies show normal values of 4.6 μg FEU / ml, while in one of the largest According to Russian laboratory networks, the upper limit for the 3rd trimester is 1.23 μg FEU / ml).
So, it seems obvious that:
- no reference for D-dimer,
- tests are inaccurate
- It can increase during pregnancy, and to very high values.
Is it possible to “knock down” D-dimer during pregnancy?
It's no secret that doctors often suggest playing it safe (and this applies not only to D-dimer). Since we do not know which levels of D-dimer are “dangerous”, if it increases significantly, it is often proposed to “bring down” its level by prescribing low-molecular-weight heparins (Fraxiparin, Clexane, etc.).
Let's figure out whether it is possible to “knock down” the D-dimer?
It turns out that before birth, neither prophylactic nor even therapeutic doses of heparins have a significant effect on D-dimer levels.
Considering all of the above, it is difficult to imagine where the cunning prescriptions of heparins in the most bizarre doses in courses of several days or weeks “under the control of D-dimer” come from!
What do domestic and international recommendations say?
Let's move on to the guidelines (recommendations). First, let's look at the place of D-dimers in guides on the use of reproductive technologies, and then in sections of various guidelines on pregnancy and VTEC.
Is it recommended to determine the level of D-dimer and prescribe any treatment if it increases in the main documents on reproductive technologies (IVF, etc.)?
- 2007. Russian Association of Human Reproduction. Assisted reproductive technologies (ART) (recommendations for doctors).
There is no mention of D-dimer and heparins.
- 2012 ACCP 9th edition.
No mention of D-dimer.
- Routine VTE prophylaxis is not recommended
- For moderate to severe ovarian hyperstimulation syndrome (OHSS), it is recommended to prevent VTEC with low-molecular-weight heparins for 3 months after resolution of OHSS (No D-dimer control!)
- 2014. Russian clinical guidelines “Prevention of venous thromboembolic complications in obstetrics and gynecology” (approved by the President of the Russian Society of Obstetricians and Gynecologists on May 15, 2014)
No mention of D-dimer.
To be fair, it is worth quoting from another document that goes against all existing domestic and foreign recommendations. Separately, I would like to note that not a single provision in this document is supported by references to studies/justifications, etc. And even in the general list of references for this document there is not a single study directly or indirectly related to D-dimer!
- 2015. Diagnosis, treatment and prevention of ovarian hyperstimulation syndrome (OHSS). Clinical recommendations.
“The basis for the prevention of thrombotic complications in OHSS is the elimination of hemoconcentration. Antithrombotic therapy is indicated when laboratory signs of hypercoagulability appear. The indication for the prescription of low molecular weight heparins is an increase in the concentration of D-dimer in the blood plasma ... "
“Observation rules for OHSS. The study of IPT, MHO and APTT does not provide information to assess the risk of thrombotic complications. The most informative levels are D-dimer, AT III, and fibrinogen.”
“When OHSS manifests itself and an effective therapeutic dose is selected, hemostasiological monitoring is carried out at least twice a week, and when symptoms regress, once a week or every 10 days. The duration of therapy with low molecular weight heparins is determined by the normalization of D-dimer levels and during pregnancy can exceed 30 days.”
“Dynamic monitoring during pregnancy is indicated. Control of thrombinemia according to coagulogram data. The administration of low-molecular-weight heparins is stopped when the standard D-dimer values are reached.”
Fortunately, today these recommendations are not available on the Ministry of Health website.
D-dimer in recommendations for VTEC.
Well, now a blitz on the place of D-dimer not only in sections on reproductive technologies, but in general in various major recommendations regarding the prevention of VTEC during pregnancy.
- 2012 ACCP 9th edition.
No mention of D-dimer.
- 2012. American Thoracic Society Clinical Practice Guideline. Evaluation of Suspected Pulmonary Embolism in Pregnancy.
These recommendations are out of the ordinary. The fact is that they propose not to look not only at an increased level of D-dimer, but believe (unlike others) that a low D-dimer (within the reference range for non-pregnant women) during pregnancy does not exclude the presence of thrombosis.
- 2014. ESC guidelines on the diagnosis and management of acute pulmonary embolism.
Data on the usefulness of D-dimer in pregnancy are conflicting, the authors say. And they suggest keeping it in mind in some cases when you want to avoid radiation exposure when diagnosing suspected VTEC. An auxiliary drug of little significance with a low level of evidence.
- 2015. Reducing the Risk of Venous Thromboembolism during Pregnancy and the Puerperium from RCOG. (The Royal College of Obstetricians and Gynecologists (RCOG) Green-top Guideline No. 37a).
No mention of D-dimer.
- 2016. Diagnosis of pregnancy-associated venous thromboembolism position paper of the Working Group in Women's Health of the Society of Thrombosis and Haemostasis (GTH)
Probably the most balanced of recommendations. Authors' summary:
- Available tests are divided into moderate and highly sensitive. The test result depends significantly on the test used.
- There are no “proven” elevated D-dimer thresholds at different stages of pregnancy.
- The use of threshold values for non-pregnant women allows us to exclude clinically significant VTEC during pregnancy.
- 2017. Department of Women's Reproductive Health, Northwestern State Medical University named after. I.I. Mechnikov, St. Petersburg. Interdisciplinary expert council. Recommendations (protocol) “Management of pregnant women at risk of thrombosis and pregnancy complications due to activation of hemostatic system disorders”
- Generally compliant with RCOG 2015
- D-dimer mentioned 1 time
Authors' summary: "Anamnestic data, including a woman's obstetric, medical and family history, are leading in assessing the risk of obstetric complications ... ... compared with coagulation screening tests, including determination of D-dimer concentrations."
I hope that all of the above is convincing enough not to assess the risk of VTEC and not prescribe heparins during pregnancy based on D-dimer values.
How to assess the risks of VTEC during pregnancy and the postpartum period?
Fortunately, there are convenient algorithms for this:
Risk assessment and tactics for preventing VTEC during pregnancy:
|
prenatal prevention required |
|
consider the need for prenatal prevention |
|
|
Risk assessment and tactics for preventing VTEC in the postpartum period:
|
postpartum prophylaxis required |
|
postpartum prophylaxis is required for at least 10 days |
|
|
As you can see, when deciding on the need for thromboprophylaxis (prescribing heparins during pregnancy and the postpartum period), the level of D-dimer in the blood does not matter.
Specific medications and dosages are prescribed only by the attending physician!
Summary - basic provisions for D-dimer during pregnancy and the postpartum period:
- During pregnancy, the concentration of D-dimers increases.
- There are currently no norms or reasonable reference values for the concentration of D-dimers at different stages of pregnancy.
- High D-dimer values do not indicate an increased risk of developing VTEC.
- The use of prophylactic and therapeutic doses of low molecular weight heparins does not affect the level of D-dimers.
- The risks of developing VTEC during pregnancy and the postpartum period are assessed not by current indicators of the hemostatic system (including D-dimer), but mainly by anamnestic data.
Note. Information has now emerged and is being discussed that may lead to the recognition that routine screening for some thrombophilias is advisable.
- Drug prevention of VTEC with courses depending on hemostasis indicators is a pointless and potentially dangerous practice.
Sources
- This article was written based on materials from a lecture and article by phlebologist Evgeniy Ilyukhin, the original article can be found at the link
- Heit J. a, Kobbervig CE, James AH, Petterson TM, Bailey KR, Melton LJ Trends in the incidence of venous thromboembolism during pregnancy or postpartum: a 30-year population-based study. //Ann. Intern. Med. 2005. Vol. 143, No. 10. P. 697–706.
- Silina N., Golovina O., Smirnova O., Nikolaeva A., Papayan A. Comparison of the results of determining the level of d-dimer by various methods in women with a normal pregnancy // Journal of Obstetrics and Women's Diseases. 2011. Vol. 6. P. 74–79.
- Szecsi PB, Jørgensen M., Klajnbard A., Andersen MR, Colov NP, Stender S. Haemostatic reference intervals in pregnancy // Thromb Haemost. 2010. Vol. 103, No. 4. P. 718–727.
- Wang M., Lu S., Li S., Shen F. Reference intervals of D-dimer during the pregnancy and puerperium period on the STA-R evolution coagulation analyzer // Clin Chim Acta. Elsevier BV, 2013. Vol. 425, No. August 2011. P. 176–180.
- Murphy N., Broadhurst DI, Khashan AS, Gilligan O., Kenny LC, O'Donoghue K. Gestation-specific D-dimer reference ranges: A cross-sectional study // BJOG An Int. J. Obstet. Gynaecol. 2015. Vol. 122, No. 3. P. 395–400.
- Gong JM, Shen Y., He YX Reference Intervals of Routine Coagulation Assays During the Pregnancy and Puerperium Period // J Clin Lab Anal. 2021. Vol. 30, No. 6. P. 912–917.
- Momot A.P., Molchanova I., Batrak T., Belozerov D., Trukhina D., Kudinova I., Maksimova N., Fadeeva N., Serdyuk G., Romanov V. Reference values of parameters of the hemostatic system during physiological pregnancy and after delivery // Problems of reproduction. 2015. No. 1. P. 89–97.
- Patel JP, Patel RK, Roberts LN, Marsh MS, Green B., Davies JG, Arya R. Changes in thrombin generation and D-dimer concentrations in women injecting enoxaparin during pregnancy and the puerperium // BMC Pregnancy Childbirth. 2014. Vol. 14, No. 1. P. 384.
- Di Nisio M., Porreca E., Di Donato V., Tiboni G. Plasma concentrations of D-dimer and outcome of in vitro fertilization // J Ovarian Res. 2014. Vol. 7, No. 1. P. 58.
- Lian R., Diao L., Xu J., Mo M., Zeng Y. The effect of plasma D-dimer on assisted reproduction technology treatment and outcome // J Reprod Immunol. Elsevier Ireland Ltd, 2021. Vol. 122. P. 44.
- Linnemann B., Bauersachs R., Rott H., Halimeh S., Zotz R., Gerhardt A., Boddenberg-Pätzold B., Toth B., Scholz U., Working Group in Women's Health of the Society of Thrombosis and Haemostasis . Diagnosis of pregnancy-associated venous thromboembolism - position paper of the Working Group in Women's Health of the Society of Thrombosis and Haemostasis (GTH). //VASA. 2016. Vol. 45, No. 2. P. 87–101.
Similar
Facebook comments
What does elevated D-dimer mean?
Even a slight increase in this indicator may indicate probable thrombosis. If the D-dimer reaches 273 ng/ml or higher, it is deadly.
D-dimer is elevated in many diseases:
- cardiac ischemia;
- acute coronary syndrome;
- thrombosis of the pulmonary artery (PE) or deep veins;
- DIC syndrome;
- acute or chronic heart failure;
- infections, injuries;
- sepsis;
- hematomas;
- kidney disease;
- preeclampsia and gestosis in pregnant women;
- coronavirus COVID-19;
- old age (over 80 years);
- malignant neoplasms.
The D-dimer level depends on the size of the clot, as well as the time and duration of taking thrombolytic drugs or anticoagulants.
With a decreased D-dimer level, the patient's risk of bleeding increases, so the patient needs to consult a hematologist and other specialists. Doctors conduct additional examinations and laboratory tests and prescribe an appropriate course of treatment.
obstetrics and gynecology
The level of D-dimer is of great importance in obstetrics and gynecology. Its level gradually increases from the early stages of pregnancy, and by the end of pregnancy it can exceed the initial level by 3-4 times. Even higher levels of D-dimer are determined in women with complicated pregnancy. D-dimer during in vitro fertilization, along with other indicators of hemostasis (PT, TT, APTT, fibrinogen), serves as a marker of the effectiveness of the stimulation cycle (pregnancy).
Clinical data indicate the high importance of assessing the level of D-dimer as a diagnostic criterion and a method of adequacy of therapy for miscarriage.
Oncological diseases
Thrombosis, as a complication, very often develops with:
- ovarian tumors;
- tumors of the pancreas, stomach;
- lung tumors;
- tumors of the rectum and colon;
- tumors of the mammary glands.
Thrombosis has a wide variety of characteristics:
- thrombosis of deep and superficial veins of the lower extremities;
- thrombosis of the subclavian veins;
- thrombosis of the superior vena cava;
- nonbacterial thrombotic endocarditis;
- various forms of internal combustion engines
Migrating, difficult-to-treat thrombophlebitis of the superficial or deep veins may be the first signs of a latent malignant disease, often ahead of the clinical manifestation of tumors. An unmotivated increase in recurrent vein thrombosis in patients with varicose veins should alert doctors to the presence of malignant diseases. The frequency of such manifestations is up to 35%.
D-dimer serves as an early marker of breast cancer metastasis, indicating lymphovascular invasion and tumor involvement of regional lymph nodes. This should be taken into account when determining the optimal extent of breast surgery
.
Problems caused by thromboembolism
Thromboembolism kills hundreds of thousands of people every year. If a blood clot enters the blood vessels of the brain, an ischemic stroke occurs. A blood clot in the coronary vessels of the heart causes an acute heart attack. Pulmonary embolism leads to acute respiratory and heart failure. Acute attention to these diseases is due to their high mortality rate.
When a blood clot forms, a process called fibrinolysis immediately begins. This process is much slower. A substance called plasmin breaks down fibrin into fragments. D-dimer is a fibrin degradation product and is one of these debris. Consequently, d-dimer will be elevated if there is a blood clot in the body.
Increasing values
- The presence of arterial and venous blood clots;
- Acute inflammatory or infectious process;
- Sepsis (severe infection of the body);
- Liver and kidney diseases;
- Oncological processes;
- Extensive hematomas (for example, as a result of a fall, compression, etc.).
Physiological increase in D-dimer concentration:
- normal pregnancy (moderate increase from the 1st trimester);
- pathological pregnancy (critical level of indicator);
- old age (from 80 years);
- recent surgery;
- thrombolytic treatment.