The first drug with 2000% bioavailability
As long as you wait, your chances of getting rid of hypertension are decreasing!
To learn more…
One of the most serious diagnoses regarding a patient’s unstable blood pressure is stage 3 arterial hypertension. An important role in assessing the patient’s condition is the risk with which the disease occurs. The third degree is the patient’s condition in which blood pressure exceeds 180 to 110 mmHg. Art., in this case, pathological changes that occur in the so-called target organs will be characteristic. The question of what is grade 3 hypertension, risk 4, can be answered based on the number of factors characteristic of each risk.
Arterial hypertension when the disease develops to stage 3 suggests that the diagnosis represents an advanced state of the patient, while therapy has a certain effect, but a complete cure is impossible, and taking medication itself is not enough to quickly alleviate the condition. If at the initial stage of the disease there is almost no symptomatic picture, then stage 3 hypertension, stage 3, risk 4, is characterized by a large number of signs and can, if left untreated, threaten the patient’s life.
Symptoms of stage 3 hypertension
From the second degree, hypertension gradually (benign form) or abruptly (malignant) passes into the third. Symptoms of hypertension at stage 3 become noticeable not only to the patient, but also to others. Among the characteristic signs of the disease, in addition to high blood pressure, headaches, numbness of the limbs, tinnitus, etc.:
- impaired coordination of movements;
- permanent vision problems;
- changes in gait, paresis and paralysis associated with cerebrovascular accidents;
- severe arrhythmia;
- hemoptysis;
- vomit;
- fainting.
Important! Hypertensive crises at this stage are accompanied by clouded consciousness, speech disturbances, and severe pain in the heart area. With each attack the situation gets worse. The well-being of a patient with stage 3 hypertension does not allow him to move normally, fully communicate with others and take care of himself.
Diagnostics
Hypertension stage 3 symptoms and treatment, it is necessary to diagnose it in time and start therapy as soon as possible. To establish an accurate diagnosis, the doctor gives a referral for a comprehensive diagnostic examination, including the following procedures:
- Blood pressure measurement. The method of daily blood pressure monitoring is often used. To do this, a portable device is installed on the patient’s lower back, and a cuff is placed on the shoulder. At certain points in time, the cuff is inflated, and a portable device records the pressure level.
- Blood and urine analysis.
- Assessment of cardiac muscle function. To do this, a physical diagnosis is carried out, during which heart rhythms are listened to with a phonendoscope, as well as an electrocardiogram - the same assessment of the work of the myocardial muscle, only more detailed. Additionally, the doctor may prescribe an ultrasound with Doppler, which will help determine the movement of blood through the vessels.
- Fundus examination. In case of hypertension, the organs of vision are among the first to be affected, therefore, to diagnose the pathology, a referral for an examination of the fundus by an ophthalmologist is required. Stage 3 hypertension is accompanied by changes in the condition of the optic nerve, deterioration of visual acuity, and impaired visual functions.
- Ultrasound of the kidneys. High blood pressure negatively affects the functioning and condition of the kidneys. With persistently high blood pressure, nephores die, which leads to the development of renal failure. Ultrasound will help identify such disorders and confirm a pre-established diagnosis.
How does the development of hypertension affect the body?
Hypertension systematically destroys blood vessels, narrowing the lumens. But its effect on the body is not limited to this. First of all, the disease affects target organs:
Classification of arterial hypertension
- heart;
- kidneys;
- brain;
- eyes.
The disease affects the heart by dilating the left ventricle. At the same time, the elastic properties of the myocardium decrease, the walls thicken, which over time leads to the development of heart failure. The risk of heart attack increases.
The kidneys must be fully supplied with blood. If the pressure is constantly high, the blood supply deteriorates, the kidneys do not receive nutrients, and their functions are impaired. At this stage of hypertension, renal failure is often diagnosed.
The brain suffers no less. Sclerotic changes reduce the tone not only of blood vessels, but also of intervertebral arteries. The brain stops receiving the necessary dose of oxygen and nutrients. Against the background of this condition, memory, attention, and intelligence deteriorate, encephalopathy develops, blood clots form, and the likelihood of a stroke increases.
Many patients of cardiologists are faced with such a complication of hypertension as retinal damage. Vessels burst, visual acuity decreases, and a feeling of chronic fatigue appears with minimal stress on the visual organs.
No ads 1
Causes of stage 2 hypertension
Narrowing of the lumens of blood vessels and slowing of blood flow are traditionally diagnosed in middle-aged and elderly people. But it is not only the passing years that cause the violation. Hypertension occurs against the background of factors contributing to the development of the disease. This:
- heredity (the more close relatives suffer from high blood pressure, the higher the likelihood that you will encounter this problem);
- lack of physical activity (physical inactivity “relaxes” the blood vessels, making them inelastic and fragile, worsens cardiac activity);
- bad habits, which include not only smoking and alcohol abuse, but also excessive consumption of salt, which retains fluid in the body;
- atherosclerosis (such a disease can be not only the cause of hypertension, but also its consequence);
- hormonal changes (pregnancy and menopause are periods during which women most often experience symptoms characteristic of arterial hypertension for the first time);
- endocrine diseases;
- kidney and genitourinary diseases;
- osteochondrosis;
- vascular disorders;
- malignant and benign tumors;
- stress of a regular nature.
Obesity is the cause of the development of hypertension (every extra kilogram is a load on the heart, blood vessels, and internal organs)
Consequences of the disease
The forms of the disease are divided according to the degree of risk to the patient’s life. The most severe of them is arterial hypertension of the 3rd degree - the risk of 3 cardiovascular complications (CVD). This means that there are three or more factors influencing the course of the disease. If with stage 2 hypertension the probability of heart attacks and strokes is 20%, then at stage 3 of the disease it increases to 30%.
When diagnosing, the degree of risk of cardiovascular complications is taken into account, which can be used to make a forecast for the next 10 years
Hypertensive crises become prolonged and in some cases end in pulmonary edema, coronary heart disease or cardiac arrest. Accompanying high blood pressure are aggravating syndromes in the form of pathological disorders in the functioning of target organs, diabetes mellitus, atherosclerosis, and heart failure. Often these complications of arterial hypertension become the causes of mortality at the age of 55-65 years.
If stage 3 hypertension (risk 3) progresses to stage 4, the person becomes disabled, unable to lead a normal lifestyle and work.
Important! Hypertension in the fourth stage is called isolated. Treatment of vessels worn out to the maximum is to maintain life, and not to eliminate symptoms that medicine cannot get rid of. A person is unable to care for himself and becomes disabled.
About the reasons
It is important to know!
STILL STRUGGLE WITH ARTERIAL HYPERTENSION INCORRECTLY? The first bioavailable drug with proven effectiveness Read more »
The development of a severe form of hypertension indicates an advanced diagnosis, when therapy was not carried out in the early stages of the disease. This may be due to the absence of clearly expressed symptoms, against which the patient attributes his condition to simple fatigue. Postponing a visit to the doctor with stable illness and even constant slight high blood pressure leads to the progression of hypertension.
Sometimes, having discovered signs of hypertension, a potential patient, instead of visiting a doctor, can try various folk remedies on himself. They, in turn, only alleviate the condition, but do not cure hypertension completely. Hypertension progresses, as a result of which the doctor is often faced with its third stage in the presence of the 4th degree of risk, which requires registration of disability.
The third reason for the appearance of such an advanced stage is not strictly following the instructions of the doctor, who has already made a diagnosis associated with constantly high blood pressure. Hypertension itself is a disease, the chances of cure are minimal, especially when it comes to its progressive forms. However, the patient, feeling an improvement in his condition, stops taking the medication, while this diagnosis requires lifelong therapy according to the regimen prescribed by the doctor. Refusal of it leads to a rapid return of symptoms and a sharp progression of the disease.
The following factors may contribute to increased blood pressure and progression of hypertension:
- A hereditary predisposition that is passed on from parents to children.
- Old age, since progressive hypertension most often appears in pensioners.
- Lack of physical activity, inert lifestyle. Malnutrition, when the diet is not balanced.
- Excess weight, which contributes to problems with blood vessels and blocking of their lumens with cholesterol plaques.
- Problems with the kidneys, resulting in swelling that negatively affects the tonometer readings.
Assessment of the patient's condition
During the examination of a hypertensive patient, an analysis of all health indicators, dietary habits and lifestyle is carried out. The more factors that worsen the condition of the cardiovascular system, the worse the prognosis for recovery. These factors include:
- heredity;
- smoking;
- alcohol abuse;
- physical inactivity;
- stress;
- excess body weight;
- age over 40 years;
- dietary restrictions;
- endocrine disorders;
- diabetes;
- kidney diseases;
- hormonal imbalances;
- pregnancy;
- menopause
If there are no aggravating factors, it is assessed that the disease has a risk of developing cardiovascular disease 1 (up to 15%). Up to three aggravating factors - risk 2 (complications occur in 15-20% of cases). This number of risks is typical for arterial hypertension of 1 and 2 degrees.
Stage 3 hypertension usually carries a risk of 3. This means that the risk of serious problems, including heart attack or stroke, increases to 30%). The diagnosis of “hypertension stage 3, risk 4” is made when, in addition to aggravating factors, there are more than three pathological changes in the functioning of target organs.
No ads 2
The conclusion of the Expert Council demonstrates the relevance of introducing a new risk category for cardiovascular complications - an extreme risk category. The studies on the basis of which this risk category is identified are presented. The extreme category of risk for patients includes the following: a combination of clinically significant cardiovascular disease caused by atherosclerosis with type 2 diabetes mellitus or familial hypercholesterolemia, a cardiovascular complication in a patient with cardiovascular disease caused by atherosclerosis, despite optimal lipid-lowering therapy and/or achieved low-density lipoprotein cholesterol level ≤1.5 mmol/l. The Expert Council's opinion describes the management of such patients, emphasizing not only the need to achieve target levels of low-density lipoprotein cholesterol, blood pressure and glycosylated hemoglobin, but also the use of drugs proven effective in reducing cardiovascular risk.
Introduction
Mortality from cardiovascular diseases (CVD) is much higher than that from infectious and oncological diseases. The World Health Organization (WHO) estimates that 17.5 million people worldwide died from CVDs in 2012, accounting for 31% of all global deaths. Of this number, 7.4 million (42%) died from coronary heart disease (CHD), 6.7 (38%) million from stroke. According to WHO estimates, by 2030, about 23.6 million people will die annually from CVDs. The annual overall mortality of the population is, according to various sources, 1.2–2.4%, while cardiovascular mortality (CVM) is 0.6–1.4%, the incidence of non-fatal myocardial infarction (MI) is from 0.6 (according to the RITA-2 study) to 2.7% (according to COURAGE). At the same time, in very high-risk patients, the annual mortality rate increases to 3.8%, while in persons with hemodynamically insignificant atherosclerosis of the coronary arteries, the mortality rate is at the level of 0.63% (data from the REACH registry). CVD is the leading cause of death in the Russian Federation, contributing 57% to overall mortality. CVD is also the most common cause of hospitalization and disability in the Russian population. The economic damage from CVD in the Russian Federation is about 3% of the country's gross domestic product. The mortality curve from CVD in the Russian Federation has a wave-like shape: from 1991 to 1994 it increased from 621 to 836 cases per 100 thousand population, then there was a decline to 747 cases in 1998, after which the mortality rate increased again to 927 cases in 2003. From then to the present, there has been a relatively stable trend towards a decrease in mortality from CVD, which in 2013 amounted to 698.1 cases, in 2014 – 653.7 per 100 thousand population. However, these indicators are still among the highest in the world, exceeding similar indicators in developed countries by 4–6 times [1]. Therefore, an important point remains the individualization of approaches to the correction of risk factors depending on the severity of the disease. In this regard, it is advisable to introduce a fifth risk category, which will make it possible to justify and carry out the most intensive treatment using drugs that have proven their influence on achieving not only certain parameters and indicators, but also significantly reducing the risk of cardiovascular complications ( MTR). It is proposed to call such a group an extreme risk group (ER). Thus, patients can be divided into five risk categories - low, moderate, high, very high and extreme.
Rationale for introducing the ER category
As is known, the category of very high CVD risk includes a fairly broad category of patients, among which there are patients with the presence of several pathologies, each of which falls under this category [2]. There is no doubt that their combination significantly increases the risk of complications. This dictates the need to identify an additional category, which is proposed to be defined as the ER group. This will make it possible to introduce more stringent requirements for the control of risk factors for these patients, which should have a positive effect on the incidence of cardiovascular events and mortality in this most severe category.
Indeed, at present, both a patient with IHD and a patient who has a combination of IHD with type 2 diabetes mellitus (T2DM) and circulatory failure can be classified as a very high risk category. However, the cardiovascular risk (CVR) in the second case is undoubtedly much higher. In particular, the combination of T2DM with CVD significantly worsens the prognosis. In this regard, recently in the treatment of T2DM there has been a transition from a “glucocentric” approach to more global tactics, with the main goal of reducing the incidence of cardiovascular events [3]. It is not so much the absolute levels of fasting plasma glucose and the level of glycosylated hemoglobin (HbA1c) that become important, but the safety of the drugs used in a particular case and their ability to reduce the incidence of cardiovascular events. This approach is similar to what was previously proposed to combat arterial hypertension: what is important is not so much the antihypertensive effect of therapy itself, but its effect on cardiovascular risk [4]. In 2021, the National Atherosclerosis Society (NSA) proposed stricter low-density lipoprotein (LDL) cholesterol targets. In very high-risk patients, the target LDL level should be 1.5 mmol/L or lower [2]. This LDL level can also be one of the target indicators of therapy for patients with ER.
The ER category was officially identified in the 2021 guidelines by the American Association of Clinical Endocrinologists and the American College of Endocrinologists (AACE) [5].
In these recommendations, patients with the following conditions are classified as ER:
- Progression of CVD caused by atherosclerosis, including unstable angina in patients with LDL levels less than 1.8 mmol/l.
- Clinically significant CVD in patients with diabetes, chronic kidney disease (CKD) stage 3–4. or with heterozygous familial hypercholesterolemia (heFH).
- Development of CVD in men under 55 years of age or women under 65 years of age.
In table 1 presents the gradation of risk categories and treatment tactics proposed in these recommendations.
As follows from the table. 1, the definition of risk categories is somewhat different from that presented in the 2021 NOA Recommendations. Taking into account their existing Russian recommendations for the correction of lipid metabolism disorders and based on a number of clinical studies described below, the following definition of ER for the Russian population is advisable: combination of clinically significant CVD caused by atherosclerosis with T2DM and/or FH, CVS in a patient with CVD caused by atherosclerosis, despite optimal lipid-lowering therapy and/or achieved LDL level ≤1.5 mmol/l. In this case, CVD caused by atherosclerosis should include ischemic heart disease, ischemic stroke or transient cerebrovascular accident, and ischemia of the lower extremities.
Thus, with the introduction of the ER category, the classification of cardiovascular risk categories takes on the following form (Table 2).
As you can see from the table. 2, ER patients are required to achieve a target LDL level of ≤1.5 mmol/L. However, there is reason to believe that a target LDL level of ≤1.3 mmol/L would be more optimal. At the moment, the evidence base for a very low target LDL level is only developing, which does not allow it to be recommended as mandatory.
In order to facilitate the work of doctors, it is advisable to develop an electronic application for mobile devices, in which, after the doctor fills out the appropriate fields, the risk category will be displayed, target LDL levels and a description of therapeutic tactics will be given.
In addition to changing the treatment tactics for these patients, the identification of an ER group may make it possible to influence the preferential drug provision for patients included in this group.
Treatment tactics for patients with ER
Patients in this group are required to correct risk factors: arterial hypertension, physical inactivity, abdominal obesity; quitting smoking, using a Mediterranean or Nordic diet. Monitoring of Lp(a) levels is recommended, with a target HbA1c level of <7%.
Patients with a total cholesterol level greater than 7.5 mmol/l and/or an LDL level greater than 4.9 mmol/l must exclude the presence of FH.
For this purpose, it is advisable to use the Dutch criteria. In addition, if FH is suspected, cascade screening with examination of first- and second-degree relatives is required [6]. If a familial disorder of lipid metabolism is suspected, if possible, a genetic examination of the patient should be performed using NGS (Next Generation Sequences) technology to exclude mutations in the genes encoding the production of LDL receptors, LDL receptor modulator protein, apoB, PCSK9. If a mutation is detected in cascade screening cancers in first-degree relatives of the index patient, genetic analysis should be performed using SNP (Single Nucleotide Polymorphism) technology.
When choosing antihypertensive therapy for patients with ER, the target blood pressure (BP) level should be ≤130/80 mmHg. Art. (and not lower than 120/80 mm Hg), but only if achieving such a blood pressure level is possible without significant side effects of antihypertensive therapy [7].
For patients with ER, the mandatory requirement is to achieve a target LDL level of ≤1.5 mmol/L, an optimal level of ≤1.3 mmol/L. Its achievement is expected by increasing lipid-lowering therapy, namely statin therapy (atorvastatin or rosuvastatin) in maximum tolerated doses in combination with ezetimibe, in some cases, a combination with PCSK9 inhibitors is possible as a third component. Achieving the target LDL level in this group of patients is a priority, so it is necessary to use the entire available arsenal of lipid-lowering drugs. When choosing statin drugs, preference should be given to original statins. In case of CKD with GFR<60 ml>
There is evidence that a target LDL level of ≤1.3 mmol/L may be preferable for patients with ER, but the evidence base for such a recommendation is currently insufficient.
Below is data on this issue.
In the case of a combination of ER with T2DM, empagliflozin and/or liraglutide should be used as antihyperglycemic therapy along with metformin. When T2DM is combined with chronic heart failure (CHF), preference is given to empagliflozin; when proven CVD is combined with T2DM, empagliflozin or liraglutide is preferred; when CVD, T2DM and obesity are combined, liraglutide is preferred.
IMPROVE-IT, FOURIER and ODYSSEY Outcomes: clinical studies supporting the need for more intensive LDL-lowering in ER patients
One of the first studies to demonstrate the benefit of greater LDL-C reduction in individuals with very high ER was the IMPROVE-IT trial. Patients who had undergone ACS were included, and the effects of lipid-lowering therapy with statins alone and combination therapy with a statin and ezetimibe were compared. The primary endpoint was cardiovascular death, myocardial infarction, unstable angina, and PCI. In the intensive control group, the LDL value was 1.369 mmol/l. After treatment for 7 years, the Kaplan-Meier survival analysis showed that the incidence of the end point in the intensive therapy group was significantly lower compared to conventional therapy - 32.7 versus 34.7%. The relative risk (RR) decreased by 6.4% (RR=0.936, 95% confidence interval [CI] - 0.89-0.99; p=0.016). The absolute risk reduction was 2%. An analysis from a subgroup of patients with diabetes (27% of all included in the study) demonstrated a decrease in RR by 14.4% (RR = 0.856, 95% CI - 0.779–0.939) in the intensive therapy group and only 2.3% in the standard treatment group (RR=0.977, 95% CI – 0.915–1.044; p=0.023). Dividing patients into other subgroups (depending on smoking, hypertension, history of PCI, creatinine level) did not demonstrate a significant difference when performing subanalyses [10].
The FOURIER study examined the effects of pain-intensive lipid-lowering therapy in individuals with very high ER. The additional effect of adding evolocumab to standard lipid-lowering therapy was studied. The primary endpoint was MI, cardiovascular death, stroke, PCI, and unstable angina. 27.5 thousand patients were included, the duration of the study was 2.2 years, the study was placebo-controlled. In the evolocumab group, the mean LDL level was 0.775 mmol/L. Against this background, 9.8% of patients in the evolocumab group and 11.3% in the comparison group reached the end point. Thus, intensive lipid-lowering therapy allowed an additional 20% reduction in risk (95% CI – 0.73–0.89). It was after this study that AACE proposed to distinguish the ER category and use lower target LDL levels [11].
In addition, in 2010, the CTT (Cholesterol Treatment Trialists') Collaboration conducted a meta-analysis of 26 clinical trials, including 169,138 patients. Groups of patients with ACS, stable coronary artery disease, T1DM (337 patients), T2DM (5414 patients), and CHF were considered. All cases demonstrated an additional 24% reduction in risk for every 1 mmol/L reduction in LDL levels. In addition, it has been shown that the lower LDL levels are reduced, the greater the risk reduction. Even for individuals with an initial LDL level <2.0 mmol/l, a decrease of every 1 mmol/l reduces the risk of significant cardiovascular events by 29%, in individuals with an initial LDL level <1.8 mmol/l - by 37% [12]. In another 2014 meta-analysis, which included 38,153 patients, patients were divided into groups depending on the achieved LDL level: 1.3 mmol/L, 1.9; 2.6; 3.2; 3.9 mmol/l. Compared with a level of 3.9 mmol/l in the group of patients with an LDL level of 1.3 mmol/l, the reduction in the relative risk of cardiovascular events was 0.44 (95% CI - 0.35–0.55). When comparing a group of patients with LDL levels of 1.3 and 1.9 mmol/l, the reduction in RR was 0.81 (95% CI - 0.70–0.95). Thus, when the LDL level reaches <1.3 mmol/l, non-HDL cholesterol <1.9 mmol/l, and apoB <50 mg>
Similar results were shown by the ODYSSEY Outcomes study (the number of included patients was 18,924) [14]. Treatment with alirocumab demonstrated a reduction in the RR of cardiovascular events regardless of baseline LDL-C. There was a significant reduction in absolute risk in the group of patients who achieved LDL levels ≥2.5 mmol/L of 3.4% for the primary composite endpoint and 1.7% for overall mortality. The reduction in RR was 15%.
Features of treatment of patients with ER in combination with T2DM
Empagliflozin is the first antihyperglycemic drug to demonstrate in a large, prospective, multicenter, double-blind, phase III EMPA-REG Outcome study (NCT01131676) not only safety, but also the benefits of use - reducing the incidence of cardiovascular events and improving outcomes associated with heart failure (HF) in patients with T2DM and established cardiovascular diseases and high cardiovascular risk.
The EMPA-REG Outcome study was conducted at 590 clinical centers in 42 countries and included 7020 patients (71% of them men) with T2DM and confirmed CVD, the average follow-up duration was more than 3 years. Patients were divided into two groups and received empagliflozin or placebo in addition to standard therapy, which included drugs with proven ability to reduce the incidence of cardiovascular events. The primary composite endpoint included incidence of cardiovascular death, nonfatal MI (excluding silent MI), and nonfatal stroke (3P-MACE); The secondary composite endpoint also included hospitalizations due to HF. The study continued until at least 691 patients experienced standardized assessment events that met the primary endpoint.
The EMPA-REG Outcome study demonstrated a 14% reduction in the rate of achievement of the primary endpoint 3P-MACE (p=0.038). At the same time, the results for each of the components of the combined point were different: overall mortality decreased by 32% (p<0.001), CVD - by 38% (p<0.0001), the frequency of non-fatal MI decreased significantly by 13% (p=0 ,22), the frequency of non-fatal stroke, on the contrary, tended to increase (by 24%; p=0.22), and the overall frequency of death from non-cardiac causes only tended to decrease (by 16%; p=0.29). At the same time, a decrease in mortality in the empagliflozin group was observed at the early stage of the study (<3 months) and was noted in all subgroups of those examined.
The incidence of hospitalization for HF decreased by 35% (p=0.002), incl. by 37% among patients who did not have HF at baseline, and by 28% among patients with HF diagnosed at baseline. The rate of hospitalization or death due to HF decreased by 39%, the number of new cases of HF (according to the criteria established in the study for HF, in particular HF with left ventricular ejection fraction <35%) - by 30%; the frequency of composite outcomes (hospitalization for HF or prescription of loop diuretics) – by 37%.
Thus, the EMPA-REG Outcome study demonstrated not only the cardiovascular safety of empagliflozin, but also its clear protective cardiovascular effects in the form of a reduction in the incidence of cardiovascular events and improvement in indicators characterizing the course of HF in patients with T2DM [15].
The effect of the glucagon-like peptide analogue liraglutide on cardiovascular system was demonstrated in the placebo-controlled LEADER study. Primary composite outcome: cardiovascular death, nonfatal MI, nonfatal stroke. 9340 patients were included, and the follow-up period was 3.8 years. The primary end point was recorded significantly less often in the liraglutide group - 608 (13.0%) out of 4668 patients than in the placebo group - 694 (14.9%) out of 4672 patients (RR = 0.87, 95% CI - 0 .78–0.7; p<0.01 for noninferiority; p=0.01 for superiority). CV risk in the liraglutide group was 4.7%, in the placebo group – 6.0%; p=0.007, mortality from any cause was also lower in the liraglutide group – 8.2 versus 9.6% in the placebo group (p=0.02). The incidence of MI, stroke and HF was also lower in the liraglutide group [16].
Conclusion
Due to the fact that the first manifestation of CVD may be cardiovascular death, it is extremely important to identify patients at high risk levels not only at the stage of the appearance of clinical symptoms, but also before their manifestations occur. It should be emphasized that the danger is not the degree of steno behind the coronary or carotid arteries, but the condition of the atherosclerotic plaque. However, at the present stage of development of cardiology, there are no reliable non-invasive methods that allow them to identify unstable atherosclerotic plaques. Therefore, it is not important to assess the patient’s risk category to determine treatment tactics. Among the risk factors for cardiovascular disease, 4 main ones should be highlighted: hypertension, dyslipidemia, smoking, T2DM/impaired glucose tolerance.
There are two main multidirectional errors in identifying patients with coronary artery disease – overdiagnosis and underestimation of the degree of risk. Frequent reasons for an unreasonable diagnosis of coronary heart disease are the presence of pain in the chest without proof of its ischemic origin, advanced age and changes in the final part of the ventricular complex on the electrocardiogram (ECG). Underestimation of the risk stems from the fact that treatment, as a rule, is started only in the presence of hemodynamically significant stenosis. In addition, PCI is unjustifiably widely used. However, it has been shown that in stable CAD, endovascular treatment does not affect the prognosis [17] and does not in all cases affect the quality of life [18].
To increase the effectiveness of the fight against special forces, it is advisable to make the following adjustments:
- if there are risk factors or if there is a suspicion of CVD caused by atherosclerosis, it is necessary to determine the risk category;
- when diagnosing IHD, one should be guided by the data of instrumental methods confirming the presence of myocardial ischemia: myocardial perfusion scintigraphy or stress echocardiography. Detecting coronary artery disease using ECG at rest and 24-hour ECG monitoring is impractical;
- When identifying patients with HF, it is necessary to measure the level of natriuretic peptide in the blood in addition to chest x-ray and echocardiography. This is especially relevant for patients with HF with preserved ejection fraction;
- in the presence of CVD caused by atherosclerosis, the prescription of lipid-lowering therapy is mandatory, regardless of the initial LDL level.
- For patients with T2DM, statin therapy is mandatory, regardless of the initial LDL level. When choosing antidiabetic therapy, drugs that reduce the risk of cardiovascular complications should be used;
- electric pacemakers should be widely used, incl. with the function of cardioverter-defibrillators, in cases where this meets the requirements of the recommendations [19].
Thus, the introduction of an additional risk category should promote greater attention to patients with ER and more strict and frequent monitoring of their lipid profile, HbA1c, and blood pressure. Patients in this category require close attention to the correction of risk factors and adherence to prescribed therapy, and careful instrumental monitoring, in particular, duplex scanning of extracranial arteries and arteries of the lower extremities. In the case of diabetes, it is advisable to manage their patients jointly by a cardiologist and an endocrinologist. Acceptance of this risk category will increase the motivation of both patients and their doctors, which should help reduce the risk of developing cardiovascular events.
About the authors
Expert Committee Presidium: I. Sergienko, M. Shestakova, S. Boystov Expert Committee: A. Ametov (Moscow), M. Antsiferov (Moscow), V. Kukharchuk (Moscow), D. Zateyschikov (Moscow), M. Ezhov ( Moscow), V. Gurevich (Moscow), A. Galyavich (Kazan), M. Voevoda (Novosibirsk), D. Duplyakov (Samara), O. Barbarashh (Kemerovo), Yu. Khalimov (St. Petersburg), G. Arutyunov (Moscow), Yu. Karpov (Moscow), M. Bubnova (Moscow), L. Drozdova (Moscow), N. Sonicheva-Paterson (Spain), A. Ansheles (Moscow), I. Samorodskaya (Moscow), N. Koziolova (Perm), O Drapkina (Moscow)
Bibliography
1. Sergienko I.V., Ansheles A.A., Kukharchuk V.V. Dyslipidemia, atherosclerosis and coronary heart disease: modern aspects of pathogenesis, diagnosis and treatment. 3rd ed., revised. and additional M., 2018.
2. Diagnosis and correction of lipid metabolism disorders for the purpose of prevention and treatment of atherosclerosis. Russian recommendations. VI revision. Atherosclerosis and dyslipidemia. 2017;3(28):5–23.
3. Dedov I.I., Shestakova M.V., Mayorov A.Yu. Algorithms for specialized medical care for patients with diabetes. 8th issue. Diabetes. 2017;20(1S):1–112.
4. Whelton PK, Carey RM The 2021 Clinical Practice Guideline for High Blood Pressure. JAMA. 2017;318(21):2073–74.
5. Jellinger PS, Handelsman Y, Rosenblit PD, et al. American Association of Clinical Endocrinologists and Ame55555rican College of Endocrinology Guidelines for Management of Dyslipidemia and Prevention of Cardiovascular Disease. Endocr Pract. 2017;23(Suppl. 2):1–87.
6. Watts GF, Gidding S, Wierzbicki AS, et al. Integrated guidance on the care of familial hypercholesterolaemia from the International FH Foundation. Int J Cardiol. 2014;171(3):309–25.
7. de Boer IH, Bakris G, Cannon CP Individualizing Blood Pressure Targets for People With Diabetes and Hypertension: Comparing the ADA and the ACC/AHA Recommendations. JAMA. 2018;319(13):1319–20.
8. de Zeeuw D., Anzalone DA, Cain VA, et al. Renal effects of atorvastatin and rosuvastatin in patients with diabetes who have progressive renal disease (PLANET I): a randomized clinical trial. Lancet. Diabet Endocrinol. 2015;3(3):81–190.
9. Barter PJ, Waters DD Variations in time to benefit among clinical trials of cholesterol-lowering drugs. J Clin Lipidol. 2018 Apr 21. Doi: 10.1016/j.jacl.2018.04.006.
10. Cannon CP, Blazing MA, Giugliano RP, et al. Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes. N Engl J Med. 2015;372(25):2387–97.
11. Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N Engl J Med. 2017;376(18):1713–22.
12. Baigent C., Blackwell L., Emberson J., et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomized trials. Cholesterol Treatment Trialists' (CTT) Collaboration. Lancet. 2010;376(9753):167–81.
13. Boekholdt SM, Hovingh GK, Mora S., et al. Very low levels of atherogenic lipoproteins and the risk for cardiovascular events: a meta-analysis of statin trials. J Am Coll Cardiol 201;64(5):485–94.
14. Institute for Clinical and Economic Review. Alirocumab for High Cholesterol – Preliminary New Evidence Update. March 10, 2018.
15. Zinman B., Wanner C., Lachin JM, et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med. 2015;373(22):2117–28.
16. Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med. 2016;375(4):311–22.
17. Mitchell JD, Brown DL Harmonizing the Paradigm With the Data in Stable Coronary Artery Disease: A Review and Viewpoint. J Am Heart Assoc. 2017;6(11).
18. Al-Lamee R, Thompson D, Dehbi HM, et al. Percutaneous coronary intervention in stable angina (ORBITA): a double-blind, randomized controlled trial. Lancet. 2018;391(10115):31–40.
19. Brignole M., Auricchio A., Baron-Esquivias G., et al. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: the Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Eur. Heart J 2013;34(29):2281–329.
Is this a new procedure for medical examination?
Treatment regimen
The first thing that is recommended for every hypertensive patient is to eliminate factors that increase the risk of complications. It is necessary to quit smoking and drinking alcohol, engage in acceptable physical activity, lose weight, and pay attention to the treatment of diseases of internal organs and systems.
Stage 3 hypertension can only be treated under strict medical supervision. The treatment regimen is drawn up individually, taking into account age, gender, degree of risk, and the presence of associated complications. In any case, the patient is prescribed medications that can help reduce blood pressure during a crisis, as well as medications taken daily that gradually stabilize the patient’s condition.
The list of medications that must be taken for stage 3 hypertension includes:
- Adrenolytics;
- Diuretics;
- ACE inhibitors;
- Beta blockers;
- Calcium antagonists.
These drugs help stabilize blood pressure, which significantly improves well-being and minimizes the likelihood of another hypertensive crisis.
Important! It is also necessary to treat concomitant diseases - diabetes mellitus, renal failure, endocrine disorders.
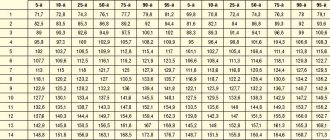
Blood pressure indicators for hypertension
The main manifestation of hypertension is a long-term and persistent increase in blood pressure (BP).
There are systolic (or upper) blood pressure, which shows the level of blood pressure at the moment the heart contracts, and diastolic (lower), which shows the level of blood pressure at the moment the heart relaxes.
Normal blood pressure levels are considered to be 120-134/80-84 mmHg, but data may vary due to emotional shocks, physical activity, changes in air temperature, etc. These fluctuations are normal; they reflect the body’s naturally programmed reaction to changes in living conditions. However, constantly elevated blood pressure in the absence of obvious reasons for this is a significant reason to take care of your health.
Arterial hypertension is indicated by a stable increase in blood pressure (systolic - above 140 mm Hg, diastolic - above 90 mm Hg when measured at a doctor’s appointment; 135/85 mm Hg and above - when measured independently) , confirmed by repeated measurements. To establish a diagnosis of arterial hypertension, two measurements with elevated blood pressure in the absence of physical and emotional stress are sufficient.
Diet for hypertension
At this stage of the disease, a person is forced to change not only his work and rest schedule, but also make adjustments to his usual diet. Without doing this, you will not be able to bring your blood pressure readings to normal levels that are not life-threatening. A sample menu for the day consists of:
- an omelette and a cup of tea with milk for the first breakfast;
- baked apple for second breakfast;
- vegetable soup, a portion of buckwheat with a steam cutlet for lunch;
- mashed potatoes with a piece of boiled fish and rosehip broth for dinner;
- a glass of kefir before bed.
Dried fruits are perfect as a snack; they have a beneficial effect on the condition of the entire cardiovascular system.
When compiling a list of dishes for the week, you must adhere to several rules that are mandatory for hypertensive patients. This:
- Salt is a poison for high blood pressure. You should cook food without it, adding salt directly on the plate if necessary.
- The diet excludes fried, salted, canned, smoked, and spicy foods.
- The basis of the diet is vegetables, fruits, cereals, lean meats and fish, boiled, steamed or baked in the oven.
- Control the amount of food entering your body. It should not exceed 2 kilograms.
- Serving size: no more than 300 g.
- The number of meals is 5-6 times a day.
- Caffeinated drinks are excluded. They should be replaced with decoctions of fruits, berries and herbs, green tea, compote.
- Alcohol in stage 3 hypertension is strictly prohibited. When taking a minimal amount of ethanol, the risk of hypertensive crisis increases.
- You can arrange fasting days on fruits, vegetables, milk.
- To normalize blood pressure, the body must receive magnesium, calcium and potassium, vitamins B, C and P every day.
Such nutrition will help cleanse blood vessels, reduce cholesterol levels in the blood, and lose a few extra pounds.
Hypertension is a dangerous disease, the complications of which kill about 9 million people worldwide every year. This outcome can be prevented by promptly responding to any changes in the body. For example, the prognosis for a diagnosis of stage 1 hypertension is usually favorable, which cannot be said about a disease that has progressed to stage 3 and is burdened with all sorts of complications.
Evidence-based medicine and myths of cardiology
Until the 90s, Russian cardiologists treated based on the opinions or views of different medical schools, which often did not agree with each other on scientific research. When the massive advent of computers helped to introduce the principles of evidence-based medicine everywhere, uniform requirements for conducting scientific research were formulated. When evaluating drugs, double-blind randomized studies have begun to be used, which are highly accurate and impartial. We created a unified knowledge base and assessment of all research conducted in the world that corresponds to a high scientific and technical level. As a result, the efficiency and safety of diagnosing and treating patients has dramatically increased.
A myth that all doctors face, but which is especially dangerous in cardiology, can be expressed in one common phrase: “Don’t take medicine, you’ll destroy your liver.” Medicines are metabolized in the liver and eliminated through the liver or kidneys, but they do not destroy them. Canceling the selected therapy can lead to a sharp increase in blood pressure, cholesterol levels and other indicators. This aggravates diseases from heart attack and stroke to diabetic coma. Surprisingly, patients are not afraid to take dietary supplements (dietary supplements) or alcohol in any quantity.
The second common myth in the practice of a cardiologist is the erroneous opinion about the dangers of cholesterol-lowering drugs - statins. A large number of studies based on the principles of evidence-based medicine confirm the high effectiveness of this group of drugs in preventing the development of atherosclerosis and its consequences (heart attack, stroke, damage to the arteries of the legs, intestines); these drugs are included in all generally accepted recommendations. Statins require constant, simple laboratory monitoring in order to avoid fairly rare side effects. Individual intolerance occurs when using any medicine or even food product. When using statins too, but rarely.