What's happened
A stroke is a sudden disruption of the normal blood supply to the brain.
Based on the nature of the disorders, there are two main types of stroke: ischemic (often called cerebral infarction) and hemorrhagic (including subarachnoid hemorrhage). This article will talk about ischemic stroke, which is 4 times more common than hemorrhagic stroke.
The word “ischemic” literally means that there is not enough blood flowing to one or another organ - with such a stroke, blood does not flow to the brain due to blockage or severe narrowing of the main arteries. As a result, brain tissue cells die.
Causes and prevention of ischemic strokes
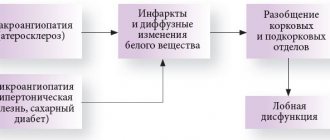
Most often, the cause of a cerebral infarction is the movement of a blood clot through an artery and clogging it in a narrow place. A thrombus is a blood clot that is primarily made up of platelets. With normal vascular patency, platelets are responsible for blood clotting, but with atherosclerosis, cholesterol plaques form, narrowing the lumen of the artery, because of this, the usual blood flow is disrupted, side turbulence is formed, and platelets stick together into clots. Also, the cause of the formation of a blood clot can be an increased level of sugar in the blood: when it occurs, microtraumas form in the walls of the artery due to an increase in blood density, which also disrupts normal blood flow.
The cause of a cerebral infarction can also be a narrowing of the lumen of a large artery by more than half. You can read more about this using the example of carotid artery stenosis (note: link to article). When an artery narrows, the blood supply to the brain does not completely stop, so a person often experiences a so-called minor stroke. A minor stroke is similar in symptoms to a regular stroke. Although the degree of damage is much less, this condition requires immediate medical attention: further deterioration of the condition of the arteries can lead to a stroke with all its consequences.
A person cannot influence the movement of a blood clot through the vessels, but everyone can pay attention to a number of risk factors, eliminate them if possible, in order to prevent the formation of a blood clot and minimize the risk of ischemic stroke.
- It is important to undergo a course of treatment and periodically check your condition with a doctor if you have a chronic disease, such as diabetes mellitus, confirmed atherosclerosis, high blood pressure, or various disorders of the heart and blood vessels.
- Experts strongly recommend giving up tobacco and alcohol.
- It is advisable to maintain an active, mobile lifestyle.
- You need to monitor your diet and avoid a strong imbalance towards fats and fast carbohydrates.
The above points are effective measures to prevent not only stroke, but also many other diseases, proven through numerous studies.
But there are also risk factors that we cannot influence. Among them are old age (over 60 years old) and heredity (if immediate relatives suffered a stroke, or they were found to have serious vascular disorders).
Medical Internet conferences
Introduction. With the development of ultrasound and computer diagnostic methods at the end of the 20th century, the role of cardiocerebral embolism in the structure of ischemic strokes has significantly increased [1]. Currently, more than 20 nosological forms of cardiac pathology have been described - sources of cerebral embolism [2-4]. Cardioembolic strokes (CEI) are characterized by high mortality and a significant incidence of disability in the general structure of ischemic strokes [5,6]. Stroke in young patients always requires the exclusion of cardioembolic origin of the disease. We present our own observation of patient T., 29 years old.
Clinical case. Patient T., 29 years old, was observed by pediatricians since childhood with a diagnosis of congenital heart disease: bicuspid aortic valve. He coped with the loads, surgical treatment was not offered. Since the late 1990s (10-12 years old), he began to notice the appearance of shortness of breath during physical activity (climbing to the 1st floor), which passed at rest. From that time on, he began to notice the appearance of acrocyanosis of the nasolabial triangle. In 2001 (15 years old), due to increasing shortness of breath, which began to occur when climbing several steps, he was examined at the cardiocenter of Samara, where coarctation of the aorta was detected, followed by surgical treatment: a bypass anastomosis of the site of aortic coarctation. After the operation I felt satisfactory. I took Curantil for several months, then, without any reason, I stopped taking it on my own. He coped with the loads satisfactorily, shortness of breath did not bother me. For 2 years after the operation, he was observed by a cardiologist in Samara, where he lived at that time. Then he was not treated or examined. Shortness of breath did not bother me, and blood pressure did not increase.
Specialized secondary education, worked as a designer. He has been smoking 20 cigarettes a day since he was 15 years old. Denies smoker's cough. Denies alcohol abuse and drug use.
On December 27, 2015, patient T. was transported by ambulance to the intensive care unit (ICU) of the Regional Clinical Hospital (RCH) in Saratov with impaired speech and movements in the left upper and lower extremities. From the medical history, it is known that he considers himself sick since the end of October 2015, when he began to notice the appearance of nasal congestion and an increase in body temperature to 37.50C. The patient regarded nasal congestion as sinusitis, and was treated independently at home with vasoconstrictor drugs and antibacterial drugs (i.m. Cefazolin). Against this background, he noted a slight improvement in the form of a decrease in body temperature and a decrease in nasal congestion. However, from the end of November 2015, he began to notice the appearance of pain in the knee and ankle joints, which occurred during movement and went away with rest; he also began to notice the appearance of heaviness in the right hypochondrium; he took Essentiale on his own. On 12/27/15, the patient went to bed, woke up and noted a speech disorder, lack of active movements in the upper and lower extremities on the left. An ambulance was called, he was hospitalized in the district hospital, then was transferred to the OKB, to the ICU with a diagnosis of cerebral infarction. Ultrasound of the abdominal organs: hepatosplenomegaly. According to magnetic resonance imaging (MRI) of the brain: MRI shows an ischemic stroke in the area of the right middle cerebral artery, dislocation syndrome. To verify the source of the embolism, transthoracic echocardiography (Echo-CG) was performed on December 30, 2015 ( Fig ). Conclusion: condition after surgical treatment of congenital heart disease: Coarctation of the aorta. Bypass surgery using a vascular prosthesis. Dilatation of the ascending aorta is aneurysmal. UPS. Bicuspid aortic valve. Combined aortic disease: slight aortic stenosis, closer to moderate, to moderate aortic regurgitation. Many hyperechoic structures on the aortic valve leaflets. The dimensions of the heart cavities and global contractility of the LV myocardium were within normal limits. Left ventricular FI 63%. MPAP 41 mmHg. Slight hypertrophy of the left ventricular myocardium. Mild to moderate mitral regurgitation. To moderate tricuspid regurgitation. Considering the structural changes in the aortic valve leaflets, it is most likely that there is a history of infective endocarditis. In connection with the examination data in the ICU, the patient was consulted by a cardiologist and diagnosed with infective endocarditis. Antibacterial therapy was started on December 31, 2015 (Ceftriaxone + Gentamicin). Against this background, the body temperature was in the range of 37.0-37.8 0C, cardialgia, heaviness in the right hypochondrium, and joint pain were not bothered. From the ICU, the patient was transferred to the neurology department with stroke, where antibacterial therapy was continued (Ceftriaxone +, Gentamicin, which was canceled on January 12, 2015, Editsin 2 g/day was prescribed, but after the 1st administration an allergic reaction like urticaria was noted , in connection with which Editsin was canceled). Laboratory tests revealed positive markers of chronic viral hepatitis C, blood cultures did not test for sterility of growth, ESR - 39 mm/h, hemoglobin - 96 g/l. Examined by a speech therapist: pseudobulbar dysarthria, spastic-paretic form. Examined by a neuropsychologist: syndrome of damage to the basal ganglia of the brain on the right. On the background of antibacterial therapy, from January 11, 2016, the body temperature returned to normal. Cardialgia, joint pain, heaviness in the right hypochondrium do not bother me. Hospitalized in the cardiology department for continued treatment and examination with a diagnosis of cerebral infarction, cardioembolic origin, in the territory of the right middle cerebral artery on 12/27/15. Central prosoparesis on the left. Left-sided hemiplegia. Right basal ganglia lesion syndrome. Infectious endocarditis of the native aortic valve. ACHD, bicuspid aortic valve. CHD, coarctation of the aorta. Bypass surgery using a vascular prosthesis in 2001.
When examined in the cardiology department: the condition is serious. Position active. Consciousness is clear. The skin is of normal color, warm, dry. Rash: no. Spider veins: no. Scars: in the 5th intercostal space from the left sternal line to the anterior axillary line. Skin turgor is normal. The mucous membranes are pink. Subcutaneous tissue: moderately developed (height 172 cm, weight 65 kg). Edema of the lower extremities – no. Lymph nodes: not palpable. Joints: active, full passive mobility. Acropachia, most pronounced on the upper extremities ( Fig. 2 ). A catheter was installed in the area of the right subclavian vein. Respiratory rate 18 per minute. On percussion there is a clear pulmonary sound above the lung parenchyma; on auscultation, breathing is harsh. Heart sounds are rhythmic, muffled, in the area of the projection of the aortic valve there is moderate systole-diastolic murmur, I tone>II tone at the apex of the heart (2:1). Heart rate = pulse = 64 per minute, the same in both arms, satisfactory qualities. Blood pressure 90/60 mm Hg. Art. Palpation of the abdomen is painless. The liver is palpated, the edge has a dense elastic consistency, slightly rounded, percussion dimensions according to Kurlov are 12x10x9 cm, the spleen is palpated, percussion its dimensions: 7x12 cm. The kidney area is not visually changed. Palpation in the projection of the bladder is painless. The symptom of tapping in the lumbar region is negative on both sides. Tendon reflexes: D=S. There are no pathological reflexes. Sense organs: decreased vision.
Data from the examination results: Hemoglobin - 100 g/l, erythrocytes - 3.14x1012 per l, leukocytes 7.6x109 per l, ESR - 38 mm/hour. Total cholesterol - 5.0 mmol/l; LDL - 3.8 mmol/l, ALT 16 u/l, AST 15 u/l. Blood test for HIV infection dated 12/31/15: negative. ECG: Sinus rhythm with heart rate 70 per minute. Horizontal position of the electrical axis of the heart. Violation of intraventricular conduction. Complete block of the right bundle branch. ( Fig. 3 ). Holter ECG monitoring: sinus rhythm, sinus arrhythmia (at night). Average heart rate is 71 beats per minute. The circadian index is 1.17. Paroxysm of unstable supraventricular tachycardia (1 episode). Rare (94) single, paired (5), aberrant (72) daytime supraventricular extrasystoles. Rare (45) single, bigeminy type in one episode, monotopic ventricular extrasystoles of the daytime type. No ST segment deviations were recorded. Consultative appointment with a neurologist on January 21, 2016: clear consciousness, communicative, oriented. Speech and swallowing are not impaired. FMN – pupils OD=OS, photoreaction preserved, no nystagmus. The face is asymmetrical, the nasolabial fold on the left is smoothed, the left corner of the mouth is slightly lowered. The tongue is deviated to the left. Tendon reflexes S>D. Left-sided hemiplegia. Left-sided hemihyposthesia. The Babinski sign on the left is positive. There are no meningeal symptoms. Ultrasound of the abdominal organs: hepatosplenomegaly.
Final diagnosis:
Main: Infectious endocarditis of the native aortic valve. UPS. Coarctation of the aorta. Bypass surgery using a vascular prosthesis in 2001. Combined aortic disease: moderate stenosis, moderate insufficiency. Relative mitral insufficiency stage II. Relative tricuspid insufficiency grade III. Pulmonary hypertension stage I Mild anemia. Hepatosplenomegaly. Dyslipidemia.
Cerebral infarction, cardioembolic origin, in the territory of the right MCA from 12/27/15. Central prosoparesis on the left. Left-sided hemiplegia. Syndrome of damage to the basal ganglia of the brain on the right. Placement of the subclavian catheter on the right 12/28/15, removal 01/25/16.
Sop.: Retinal angiopathy OU. Chronic viral hepatitis C.
Donkey: Dislocation syndrome. Single ventricular and supraventricular extrasystole. Paroxysm of unstable supraventricular tachycardia.
Treatment was carried out: Cereton 1200 mg/day, Mexidol solution 600 mg/day, cancelled, Cefogram solution 4 g/day IV drops + tab. Tavanik 500 mg/day, physiotherapeutic treatment. During treatment, stable normalization of temperature, hemodynamic stability, improvement in general condition, leukocyte level, ESR in the blood test were within normal limits. In a stable condition of moderate severity, he was transferred to a district hospital to continue treatment. It is recommended to continue combination antibacterial therapy for up to 6 weeks.
Conclusion. The difficulty of diagnosing cardioembolic stroke is clearly demonstrated in this clinical case. One of the difficulties in diagnosing infective endocarditis and CES, as its complications, is its manifestation, which often leads specialists into diagnostic confusion. It is worth noting that the information content of the classical diagnostic method - transthoracic echo-CG in this case is quite low, which is associated with the impossibility of optimal visualization and assessment of the extent of damage to the aortic valve and vascular prosthesis after surgical treatment of aortic coarctation according to transthoracic echo-CG only. It is recommended to use a transesophageal sensor, which increases the sensitivity of the method to 90-93%. Also in this clinical situation, significant damage to the aortic valve dictates the need for cardiac surgery as the main method of treating this condition. The patient was consulted by a cardiac surgeon, and after stabilizing his condition, he was recommended to go to a cardiac surgery center for aortic valve replacement.
The presented clinical observation proves the difficulties of diagnosing IE, while simultaneously demonstrating that the joint well-coordinated work of cardiologists and neurologists can save the lives of young patients.
Symptoms of ischemic stroke
Almost never a cerebral infarction is asymptomatic. You may have already come across actively distributed reminders on the timely recognition of a stroke: after all, it is very important to call an ambulance and provide medical assistance to the patient as early as possible - the earlier assistance is provided, the less brain damage.
The main symptoms of ischemic stroke are:
- dizziness,
- loss of orientation in space,
- vomit,
- convulsions,
- impaired coordination, speech, vision, writing, reading, swallowing,
- inability to move individual limbs and/or perform simple manipulations such as raising two arms at the same time, brushing teeth, or turning pages of a book.
The symptoms are extremely varied. They depend primarily on which particular part of the brain was deprived of blood supply - then exactly the function for which this part is responsible will be disrupted.
At the same time, all the symptoms do not appear; you may notice one or more - and this is a good reason to immediately call an ambulance.
Clinical picture
Computed tomography of the brain. Hypertensive subcortical hematoma in the right frontal lobe
Computed tomography of the brain of the same patient 4 days after surgery - removal of an intracerebral hematoma of the right frontal lobe
If symptoms of acute cerebrovascular accident appear, you should immediately call emergency help in order to begin treatment as early as possible.
Symptoms
Stroke may manifest as cerebral
and
focal
neurological symptoms.
General cerebral symptoms
strokes are different. This symptom may occur in the form of impaired consciousness, stupor, drowsiness, or, conversely, agitation; a short-term loss of consciousness may also occur for several minutes. A severe headache may be accompanied by nausea or vomiting. Sometimes dizziness occurs. A person may feel a loss of orientation in time and space. Possible vegetative symptoms: feeling of heat, sweating, palpitations, dry mouth.
focal symptoms appear
brain damage. The clinical picture is determined by which part of the brain is affected due to damage to the blood vessel supplying it.
If a part of the brain provides the function of movement, then weakness in the arm or leg develops, including paralysis. Loss of strength in the limbs may be accompanied by a decrease in sensitivity in them, impaired speech, and vision. These focal stroke symptoms are mainly associated with damage to the area of the brain supplied by the carotid artery. Muscle weakness (hemiparesis), speech and pronunciation problems, decreased vision in one eye and pulsation of the carotid artery in the neck on the affected side are characteristic. Sometimes there is unsteadiness of gait, loss of balance, uncontrollable vomiting, dizziness, especially in cases where the blood vessels supplying the areas of the brain responsible for coordinating movements and a sense of body position in space are affected. “Spotty ischemia” occurs in the cerebellum, occipital lobes and deep structures and brain stem. Attacks of dizziness in any direction are observed when objects rotate around a person. Against this background, there may be visual and oculomotor disturbances (strabismus, double vision, decreased visual fields), unsteadiness and instability, deterioration in speech, movements and sensitivity.
Diagnostics
Diagnosis of a stroke is quite complex, because to identify the cause and assess brain damage, and therefore the consequences of a stroke, the doctor will need a large amount of data.
To visualize the condition of the brain vessels, CT or MRI can be used, depending on the situation. A fairly informative study on the state of blood flow will be angiography - an X-ray examination using a contrast agent injected into the vessels.
In addition, the doctor may prescribe blood and urine tests; test for glucose and cholesterol levels; conduct an ultrasound examination.