Antibodies are complex compounds that contain carbohydrate and protein (produced by the immune system to detect and destroy pathogenic bacteria and microorganisms). It is worth noting that autoantibodies instantly react to even minimal deviations from the norm in the body: they can begin to perceive healthy cells as dangerous, therefore, actively destroying them.
It is for this reason that an analysis for antibodies to thyroid peroxidase (the enzyme through which the thyroid gland synthesizes iodine-containing hormones) allows one to determine the presence of the disease even when they, in fact, have not yet manifested themselves.
Problems with the thyroid gland and disturbances in the levels of the hormones T4, T3, and TSH can cause serious consequences, such as thyrotoxic crisis, hypothyroid coma, and even death. Endocrinologists unanimously say that problems with the thyroid gland are easy to solve if they are diagnosed in a timely manner.
Description
Synonyms (rus): Antibodies to thyroid peroxidase, microsomal antibodies, antibodies to microsomal antigen, ATTPO, ATPO
Synonyms (eng): Anti-thyroid Peroxidase Autoantibodies, Antimicrosomal Antibodies, Antithyroid Microsomal Antibodies, Thyroid Peroxidase Autoantibodies, TPO Antibodies, Thyroid Peroxidase Test, Thyroid microsomal antibody, Thyroperoxidase antibody, TPOAb, Anti-TPO.
Biomaterial: Venous blood
Indicator(s): Autoantibodies to thyroid peroxidase.
Method(s): Enzyme -linked immunosorbent assay (ELISA)
Container type and preanalytical features: Biochemical tube with coagulation activator, 6 ml (red or brown cap)
Thyroid peroxidase is a 105 kDa glycoprotein located on the membrane of thyrocytes. This enzyme is specific to the thyroid gland and is key in the synthesis of thyroid hormones. It catalyzes the reactions of iodination of tyrosine residues to form monoiodotyrosine and diiodotyrosine and the binding of iodinated tyrosines to each other in the thyroglobulin molecule to form triiodothyronine (T3) and thyroxine (T4). Thus, this enzyme is necessary for the normal functioning of the thyroid gland. Antibodies to the enzyme are involved in the destruction of thyrocytes through 2 mechanisms: antibody-dependent cellular cytotoxicity involving NK cells and complement-mediated cytotoxicity. Antibodies to thyroid peroxidase are the main marker of autoimmune thyroid diseases. They are found in 85% of patients with Graves' disease, more than 90% of patients with Hashimoto's thyroiditis, 67% of patients with postpartum thyroiditis and in 10-20% of cases of non-autoimmune thyroid diseases. Thus, the concentration of antibodies in patients with sporadic goiter and thyroid cancer is often increased, which is associated with the concomitant development of thyroiditis. It should be noted that these antibodies are also found in healthy individuals (up to 26% of women, 9% of men), their occurrence increases with age. In patients with subclinical hypothyroidism, the presence of antibodies to thyroid peroxidase indicates a high risk of developing clinical manifestations. Of particular importance is the determination of antibodies to thyroid peroxidase in pregnant women, since these antibodies are able to penetrate the placental barrier and affect the fetal thyroid gland. Thyroid antibodies may also be found in other autoimmune diseases, such as type 1 diabetes.
Reasons for the appearance of antibodies to thyroid peroxidase
Content:
- Reasons for the appearance of antibodies to thyroid peroxidase
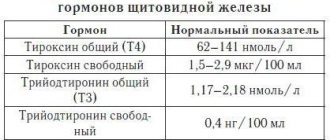
- Characteristic indicators of the presence of excess hormone levels
- Antibody test algorithm
Thyroid peroxidase is a special enzyme of the thyroid gland.
It helps accelerate the process of iodination of tyrosine residues of the thyroglobulin protein, and also activates the fusion of iodotyrosines, known as T4 and T3.
For one reason or another, the body may begin to consider this enzyme as foreign, therefore, antibodies to thyroid peroxidase begin to be produced to destroy the enzyme.
There are a number of reasons that can influence the immune system to begin the active process of producing antibodies to thyroid peroxidase: autoimmune diseases, diseases and injuries of the thyroid gland, genetics, chronic illnesses, sinusitis, anemia, diabetes, iodine overdose or deficiency, previous illnesses of viral etiology, intoxication, radiation.
A frequent increase in the number of antibodies to thyroid peroxidase is observed in women during pregnancy. This phenomenon occurs due to the restructuring of the hormonal and immune systems in order to effectively bear the baby.
During pregnancy, a woman’s thyroid gland begins to work in a special way, since it is obliged to enrich not only her body with the necessary amount of vital elements, but also the body of the developing fetus. Among the main and common causes of increased AT to thyroid peroxidase, the following number of factors are worth noting:
- various pathologies of the endocrine system and thyroid gland;
- systemic lupus erythematosus;
- rheumatism;
- pernicious anemia.
If the cause of the imbalance in enzyme levels is pregnancy, the number of antibodies will return to normal on their own eight months after birth.
Interpretation
The norm is the level of antibodies to thyroid peroxidase not exceeding 34 IU/ml. This result can be obtained in the absence of autoimmune damage to the thyroid gland, and the disease is controlled during the therapy. A result of >34 IU/mL in most cases indicates the presence of an autoimmune thyroid disease such as Graves' disease or Hashimoto's thyroiditis. A slight excess of the threshold level may indicate the presence of a concomitant autoimmune disease - type 1 diabetes, rheumatoid arthritis, etc., as well as the development of thyroiditis in non-autoimmune thyroid disease. A consistently high level of antibodies or their increase during therapy is a sign of its ineffectiveness.
Anti-TPO (antibodies to microsomal thyroid peroxidase)
Thyroid peroxidase (TPO) is an enzyme responsible for the production of thyroid hormones. It provides the formation of the active form of iodine by oxidizing iodide to synthesize triiodothyronine (T3) and thyroxine (tetraiodothyronine, T4). TPO synthesis is regulated by thyroid-stimulating hormone (TSH). Thyroid peroxidase is a common antigen - in some cases, the body perceives it as a foreign agent and forms antibodies to it - antibodies to microsomal thyroid peroxidase (anti-TPO) .
In what cases is anti-TPO antibody testing usually prescribed?
Testing for antibodies to thyroid peroxidase (anti-TPO) is the most informative test for determining autoimmune thyroid diseases.
The test is prescribed to patients with signs of thyroid dysfunction, as well as with pathological test results for TSH, free T4 and free T3.
To get a more complete picture of the condition of the thyroid gland, you can take a test for antibodies to TPO along with a test for TSH and other thyroid hormones, or take a comprehensive test - “Thyroid examination, screening”, which, in addition to hormones, also includes antibodies to thyroglobulin.
What do the test results mean?
If the level of antibodies to TPO is within the normal range, then most likely the symptoms of thyroid dysfunction are associated with another, non-autoimmune cause. However, a certain percentage of patients do not have antibodies in the initial stages of the disease; they may appear later. Therefore, your doctor may refer you for re-testing after some time.
Most often, elevated levels of antibodies to TPO are observed in patients suffering from Hashimoto's thyroiditis. With this disease, the presence of high antibodies accounts for about 90% of cases, which confirms its autoimmune origin. Antibodies are also found with a frequency of 60% -80% in Graves' disease.
Patients with other autoimmune diseases (such as adrenal insufficiency, rheumatoid arthritis, type 1 diabetes) may have antibodies to thyroid peroxidase. The test results can also be used by endocrinologists when deciding on treatment for a patient with subclinical hypothyroidism.
About 5% of healthy people have antibodies to thyroid peroxidase. The prevalence of these antibodies is generally higher in women and tends to increase with age. The presence of antibodies to thyroid peroxidase indicates an increased risk of developing thyroid disease in the future. Patients with anti-TPO antibodies without visible thyroid dysfunction require regular evaluation as they are significantly more likely to develop thyroid disease in the future.
Test deadlines.
Typically, the TPO antibody result is ready in 1-2 days.
How to prepare for the analysis?
No special preparation is required. You can read more in the “Preparation” section.
Bibliography
- Lapin S.V. Totolyan A.A. Immunological laboratory diagnosis of autoimmune diseases. Publishing house "Man", St. Petersburg - 2010.
- Tietz Clinical guide to laboratory tests. 4th ed. Ed. Wu ANB- USA, WB Sounders Company, 2006, 1798 p.
- Conrad K, Schlosler W., Hiepe F., Fitzler MJ Autoantibodies in Organ Specific Autoimmune Diseases: A Diagnostic Reference/PABST, Dresden – 2011.
- Conrad K, Schlosler W., Hiepe F., Fitzler MJ Autoantibodies in Systemic Autoimmune Diseases: A Diagnostic Reference/PABST, Dresden – 2007.
- Gershvin ME, Meroni PL, Shoenfeld Y. Autoantibodies 2nd ed./ Elsevier Science – 2006.
- Shoenfeld Y., Cervera R, Gershvin ME Diagnostic Criteria in Autoimmune Diseases / Humana Press – 2008.
- Czarnocka, B., Eschler, D. C., Godlewska, M., & Tomer, Y. Thyroid Autoantibodies. / Autoantibodies, 365–373 - 2014
- Weetman, A. P. (2014). Thyroid disease. / The Autoimmune Diseases, 557–574 - 2014.
- Test system manufacturer's instructions
Diseases of the thyroid gland during pregnancy. What's new.
Murzaeva Irina Yurievna
Endocrinologist, Preventive medicine
May 28, 2018
May 25th was World Thyroid Day.
I would like to note it somehow. Therefore, this article is dedicated to the “hero of the occasion thyroid gland” and the most important event in a woman’s life - pregnancy. :) I will present you with updated data on this topic.
Therefore, this article is dedicated to the “hero of the occasion thyroid gland” and the most important event in a woman’s life - pregnancy. :) I will present you with updated data on this topic.
Believe me, it will be interesting.
- of absolute hypothyroxinemia has been reintroduced into practice , that is, in the 1st trimester of pregnancy 0-12 weeks with a clear two-fold decrease in free T4 levels, with normal TSH - this condition is an indication for adjustment with L-Thyroxine drugs. A decrease in T4 St. in the 2nd and 3rd trimester - is physiological.
- IVF protocol , against the background of stimulation of ovulation with gonadotropin preparations, subclinical hypothyroidism (associated with a sharp increase in the level of blood estrogen), especially when carrying antibodies to TPO and TG, and this condition is also an indication for correction with L-Thyroxine preparations.
- To diagnose AIT in a woman during pregnancy, it is necessary to take blood samples only for TSH, T4 and T3, but also take blood samples for all types of antibodies - antibodies to TPO and TG .
- The issue of prescribing L-Thyroxine drugs during pregnancy with a TSH level above 2.5 is decided in favor of L-Thyroxine in the presence of positive antibodies to TPO and TG in the blood, or in the absence of these, and a normal T4 blood level - the patient can remain under observation without administering L-Thyroxine drugs ( in the absence of a history of thyroid disease in the past and the TSH level reaching no higher than the upper reference value characteristic of a given laboratory) Previously, this point in pregnancy management was considered much more strictly - with a TSH level above 2.5, L-Thyroxine preparations were given to everyone.
- Dedicated to gynecologists Not a single study has indicated any indication for termination of pregnancy if a woman has uncompensated or manifest hypothyroidism, even with a TSH of -100 mIU/ml. The main thing is to immediately prescribe a full replacement dose of L-Thyroxine during the identified period. And do not titrate it, as is done outside of pregnancy.
- Iodine preparations are indicated for all women during pregnancy and lactation, even with AIT (especially since the woman is “under the cover” of L-Thyroxine) at an average dose of 300 mcg/day.
- In the 1st trimester of pregnancy, to determine absolute hypothyroxinemia, determination of free T4 is indicated, and in the 2-3rd trimester, total T4 and total T3.
- The appearance for the first time during pregnancy of an increased titer of antibodies to TPO and TG with a normal TSH is a risk factor for postpartum thyroiditis.
- For pregnancy and outside of it, subclinical hypothyroidism is a condition in which TSH is in the range of 4-10, and manifest hypothyroidism is when TSH is above 10 mIU/ml.
- TSH levels for compensation with LThyroxine already with existing and treated hypothyroidism, 1st trimester - TSH = 0.1-2.5, 2nd trimester TSH = 0.2-3.0, 3rd trimester 0.3-3.5 mIU/ml.
- The dose of L-Thyroxine replacement for manifest hypothyroidism is 2.3 mcg/kg body weight. Outside of pregnancy, 1.6-1.8 mcg/kg of weight.
 With subclinical hypothyroidism during pregnancy, 1.2 mcg/kg of weight.
With subclinical hypothyroidism during pregnancy, 1.2 mcg/kg of weight. - An overdose of L-Thyroxine during pregnancy is not a cause of miscarriage; there is no need to be afraid of large replacement doses.
- After childbirth, the dose of L-Thyroxine that was before pregnancy is maintained.
- After childbirth, if subclinical hypothyroidism is diagnosed for the first time during a given pregnancy, L-Thyroxine is discontinued.
- Pregnancy - after surgery for thyroid cancer without RIT, it can be planned after 6-8 months. provided that euthyroidism is achieved with hormone replacement therapy. With the implementation of RIT, planning is allowed after a year.
- If thyroid cancer is detected during pregnancy and there are no indications for emergency removal of the thyroid gland (only after childbirth), suppressive doses of L-Thyroxine are indicated during this pregnancy.
- When a nodular goiter is diagnosed for the first time , blood sampling for hormones and always calcitonin (a marker of thyroid cancer) is indicated.
- DTZ and pregnancy nothing new has appeared DTZ (diffuse toxic goiter) is not an indication for pregnancy and the best way to treat it during pregnancy is Tyrozol , in maximum doses of 30 mg/day.
 With subclinical hypothyroidism during pregnancy, 1.2 mcg/kg of weight.
With subclinical hypothyroidism during pregnancy, 1.2 mcg/kg of weight.