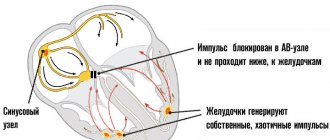
Hypotonia in newborns
Hypotonia, or decreased muscle tone, is usually found at birth or in infancy. If your baby has hypotension, he may be born lethargic, have difficulty sucking at the breast, and get tired quickly when feeding. When examined, such a child’s arms and legs easily extend at the joints; he can spread his hips almost without resistance to an angle of more than 90 degrees. A child with hypotonicity of the muscles of the cervical and shoulder girdle has difficulty controlling the head and has delays in the development of grasping skills and fine motor skills.
As a child with reduced muscle tone gets older, he or she will experience difficulty speaking, have incorrect posture, hypermobility in the joints, and decreased physical endurance.
Causes of hypotension in young children
Hypotension can be caused by congenital diseases of the nervous or muscular system. Sometimes hypotension is the result of birth or neonatal trauma, hypoxia during childbirth, an acquired disease, or an inherited disorder. Also, a decrease in muscle tone may be associated with physiological immaturity of the nervous system. There are situations when the cause of hypotension cannot be determined. Some babies are born with hypotension that is not associated with other diseases or conditions. This is called benign congenital hypotension. These children have minor developmental delays or learning difficulties. Physical and speech therapy can help a child regain tone and develop normally or reduce developmental delays.
It is important to know that hypotension can be caused by dangerous diseases that affect the brain, central nervous system or muscles:
Cerebral palsy
In many cases, these chronic diseases require lifelong care and treatment.
Hypotension can also be caused by genetic diseases:
- Down syndrome
- Prader-Willi syndrome
- Tay-Sachs disease
- Trisomy 13
- Hartnup's disease.
Arterial hypotension. Causes
The cause of persistent low blood pressure may be a person’s congenital constitutional characteristics:
- asthenia;
- disruption of connective tissue formation (dysplasia);
- neuroendocrine imbalance (the consequence of which is disruption of blood circulation regulation).
In this case, they talk about essential (or primary) arterial hypotension.
An acquired decrease in blood pressure, which can be constant or paroxysmal, is usually a consequence or concomitant pathology of a number of other diseases:
- endocrine disorders (diabetes mellitus, hypothyroidism, adrenal insufficiency);
- infectious and tumor diseases, resulting in anemia and cachexia (exhaustion);
- diseases of the nervous system;
- chronic fatigue syndrome;
- amyloidosis;
- heart ailments;
- side effects of medications, etc.
A sharp decrease in blood pressure, even to the point of fainting, may have its own characteristic trigger factors:
- eating;
- transition from horizontal to vertical position;
- emotional and physical overload (although usually in response to them, pressure, on the contrary, increases);
- night sleep.
In psychosomatics, manifestations of hypotension are considered as a consequence of insufficient life tension, pressure, and passive tactics of avoiding emerging difficulties and obstacles instead of actively resolving them.
Muscle hypertonicity in a child
If your newborn baby constantly looks away, clenches his fists, has difficulty moving, and has obvious emotional signs of general discomfort, he may be suffering from hypertension.
Muscular hypertonicity is a condition in which a child's muscles are constantly tense, causing you to be unable to easily bend or straighten your child's legs and arms. If you touch the baby’s muscles, they will be dense to the touch, like those of a well-pumped bodybuilder. It is important to know that hypertonicity is a pathological condition.
In a newborn with hypertonicity, muscle tension can noticeably weaken only during sleep. As your baby grows, you may notice that he or she feels “stiff” and has trouble rotating his or her body or bending his or her limbs. In infants prone to hypertonicity, this condition may be caused by a startle reaction to an unexpected sound, movement or touch. Hypertonicity in fear is characterized by excessive arching of the head and jerky movements of the arms and legs. Sometimes severe fright can lead to a permanent state of hypertonicity.
Children suffering from hypertension will have a delay in physical development due to the fact that tense muscles prevent him from moving normally. As a result, a baby with hypertonicity will learn to crawl and walk much later. If the problem of hypertonicity is not eliminated, the child’s gait will be very unstable, he will spread his legs wide when walking. Also, children with hypertonicity may suffer from congenital hip dislocation and sleep apnea due to impaired muscle function.
Arterial hypotension. First aid
With the development of a hypotensive crisis and fainting, it is important:
- Place the person in the feet-over-head position. If this happens in transport and there is nowhere to put it, you can lower your head down below your knees.
- Unbutton your clothes and, if possible, provide access to fresh air.
- If the person is conscious, calm him down and give him water to drink.
- You can rub your ears and massage the collar area and fingertips (the endings of many of the body’s energy channels are located here).
- In case of prolonged fainting, call an ambulance.
Make an appointment
Causes of hypertension in children
Hypertonicity can be hereditary in nature and caused by mutations in a specific genetic sequence. Such mutations negatively affect the production of glycine in the child's body, which helps reduce the stimulating effect of neurons on muscle fibers in order to ensure their relaxation after tension. When something interferes with the functioning of glycine, the body's ability to control muscle relaxation is weakened.
To diagnose hypertonicity (for example, in order to distinguish hypertonicity from epilepsy), a neurologist may prescribe to a child:
- Electromyography (EMG), which will examine electrical impulses in the muscles.
- Electroencephalography (EEG) can be used to assess a child's brain activity and its effect on muscle tone.
- Molecular genetic testing can determine the presence of specific mutations in the GLRA1 and SLC6A5 genes.
Arterial hypotension in children
A persistent decrease in blood pressure in childhood may be asymptomatic and reflect compensated physiological features. But much more often, this condition affects the quality of life, resulting in increased fatigue, low performance, poor attention and ability to concentrate (which affects interest in learning new things), weather sensitivity, etc. And in general it forms an asthenic psychophysiological type. Often in this case, the child is diagnosed with “neurocirculatory dystonia” or “vegetative-vascular dystonia” of the hypotensive type.
In adulthood, there is a risk of this disease transitioning into a phase of persistent increase in blood pressure and a number of complications from the cardiovascular system.
Treatment of hypertension in children
To treat hypertension, your doctor may prescribe:
medications, physiotherapy, massage and osteopathy, aquatherapy. Consultation with a family psychologist is also important. Learning how to cope with emotions and disappointments and how to remain calm will be an important factor in creating a positive psychological climate in your child's environment.
- Massage and stretching exercises can significantly relax the muscles and provide relief to the child.
- Aquatherapy in warm water also promotes better muscle relaxation and overall calming of a child with hypertension. Aquatherapy sessions can be performed as early as 3 weeks of age.
- Thanks to the course of treatment, education of the child and parents, the child, as he grows up, will learn to cope with any restrictions and will be able to lead a full life.
Arterial hypotension. Treatment
Standard treatment of secondary hypotension involves treatment of underlying diseases and compensation for disorders of the cardiovascular system. Particular attention should be paid to the selection and dosage of medications that can cause a decrease in blood pressure.
In the treatment of primary hypotension, priority is given to non-drug methods: physical exercise (swimming, walking), massage, correction of daily routine and nutrition, position during work and sleep. Patients diagnosed with “neurocirculatory dystonia” or “vegetative-vascular dystonia” of the hypotensive type are called people with a “narrow comfort zone”, for whom it is vital to find their own individual rhythm of life and, if possible, to go beyond it as little as possible.
Arterial hypotension is a systemic health disorder. And in its treatment, holistic methods with an individual approach to a person can be successfully applied - acupuncture, homeopathy, osteopathy, herbal medicine.
Within the framework of the psychosomatic approach, the most important component of the treatment of hypotension is the activity of the patient himself. The main thing for a person is to want and be able to achieve something, overcome it, implement it. Even following the doctor’s recommendations in itself has a healing effect, since it involves the free will and energy of the person himself.
Dystonia
Muscular dystonia is a disorder characterized by impaired motor activity of the child and abnormal development of muscle tone. Muscular dystonia can be caused by genetic disorders or birth trauma that leads to hypoxia of the child's brain or cerebral hemorrhage.
Other causes of acquired dystonia in infants may include:
- infections
- side effects of certain medications the mother took during pregnancy
- toxic effects on the fetus
The disorder is caused by impaired or immature connections between the nervous system and muscles. With dystonia against the background of general hypotension, when performing passive movements, individual muscles in the child become spastic (strongly contracted). In a child, this looks like a “combination” of hypertonicity of some muscles with hypotonicity of others, which leads to the appearance of writhing movements. This condition can appear after strong experiences, excitement, feelings of fear, in an unfamiliar environment, with sharp sounds or when touching a child with cold hands.
In addition to uncontrolled muscle movement, other symptoms of dystonia include leg cramps, involuntary neck movements, and uncontrolled blinking. Symptoms usually affect only one side of the body and stabilize within five years. However, accidents and injuries can worsen the disease.
The extreme severity of muscular dystonia is observed in children with cerebral palsy, which is a cause of disability.
There is no specific treatment for dystonia. Doctors use a complex of therapeutic measures, including drug and physical therapy, massages, osteopathy, and the help of a psychologist. Mild and moderate dystonia responds well to restorative treatment if it is started in a timely manner and carried out regularly.
The most important thing in the treatment of dystonia: the earliest possible diagnosis and initiation of therapy. The best results are observed if the diagnosis is made in the first months of life.
The problem of arterial dystonia in children is extremely relevant. The greatest attention in pediatrics today is paid to arterial hypertension as a prelude to arterial hypertension in adults. Issues of arterial hypotension in children and adolescents remain in the shadows, although accumulating factual material shows that hypotensive conditions are more common in children than in adults and amount to up to 20.9%.
Hypotension is a symptom that reflects varying degrees of decrease in blood pressure. The term “...tension” most accurately reflects the pressure of liquids in vessels and cavities. The term “...tonia” is used to assess the tone of the smooth muscles of the vascular wall. It is known that a decrease in the tone of precapillaries—arterioles—is most often the main hemodynamic factor in a prolonged decrease in blood pressure. This determines the possibility of using the term arterial hypotension along with the term arterial hypotension.
There are many classifications of hypotonic conditions. In Russia, the classification of N.S. is most widely used in practical medicine, including in pediatrics. Molchanov.
Classification of hypotonic states by N.S. Molchanov
1.Physiological hypotension:
— hypotension as an individual variant of the norm;
— hypotension due to increased training (in athletes);
— adaptive compensatory hypotension of highland residents;
2.Pathological hypotension (primary and secondary)
Arterial hypotension is considered physiological in the absence of clinical manifestations of the disease: there are no subjective complaints or manifestations of autonomic dysfunction.
Primary arterial hypotension develops against the background of vegetative-vascular dystonia syndrome with pronounced clinical symptoms characteristic of vagotonia. It can occur with an unstable, reversible flow. In some children, the disease develops into a pronounced persistent form - hypotension. Hypotonic disease includes a persistent decrease in blood pressure, accompanied by severe symptoms in the form of dizziness, headaches, and orthostatic dysregulation.
Secondary (symptomatic) arterial hypotension occurs against the background of diseases of the cardiovascular system, occurring with heart failure syndrome (myocardial disease, heart rhythm disturbances), endocrine diseases (hypofunction of the adrenal glands, thyroid gland, etc.), pathology of the nervous system, accompanied by increased intracranial pressure , anemia of various origins, while taking medications (antihypertensives, antihistamines, antidepressants, some antiarrhythmic drugs).
Currently, primary arterial hypotension is considered as a multifactorial pathology, in the development of which hereditary predisposition and the complex effect of exo- and endogenous factors are extremely important. Hereditary predisposition to arterial hypotension is revealed when collecting a family history in up to 60.9% of cases, most often on the maternal side. In patients with an asthenic constitution, arterial hypotension is an almost obligatory attribute.
It should be noted that the unfavorable course of pregnancy and childbirth in combination with low blood pressure in the mother during pregnancy forms a negative metabolic memory in the intrauterine patient and autonomic dysfunction with a tendency to lower blood pressure. Most often, arterial hypotension manifests itself in adolescence, which is due to puberty and the personality characteristics of the teenager. Among the exogenous factors predisposing to the development of arterial hypotension, it should be noted chronic psycho-emotional stress (incomplete families, death of loved ones, etc.), foci of chronic infection, unfavorable social conditions, mental fatigue and physical inactivity.
The pathogenesis of arterial hypotension remains insufficiently studied at present. No specific causes of the disease have been established, but there are many theories of the occurrence of the disease: neurogenic, humoral, constitutional-endocrine, vegetative. Today, a violation of the mechanisms of autoregulation of central hemodynamics is considered to be clearly proven - a discrepancy between cardiac output and total peripheral vascular resistance, usually due to a decrease in the latter. It should be noted that as hypotension progresses, total peripheral resistance continues to decrease. In children and adolescents, the most significant mechanism for reducing peripheral resistance is autonomic. The participation of biologically active compounds with antihypertensive properties - prostaglandins, natriuretic peptides, nitric oxide, kinins, etc. - is extremely important in the development of the pathological process.
Arterial hypotension is characterized by an unusually high polymorphism of complaints, an abundance and lability of clinical manifestations, and a striking asthenovegetative syndrome, leading to unsatisfactory environmental adaptation and a decrease in quality of life. The main symptom of arterial hypotension is a decrease in blood pressure. Diagnosis of arterial hypotension is based on the results of 3 measurements of blood pressure using an age-appropriate cuff (Table 1), with an interval of 3-5 minutes. When assessing the results obtained, unified criteria for arterial hypotension (Table 2) and the centile method are used. Arterial hypotension is defined as blood pressure values below the 10th percentile for the corresponding age and gender.
Table 1.
Cuff width for children according to WHO
| Age | Cuff width |
| Up to a year | 2.5 cm |
| 1-3 years | 5-6 cm |
| 4-7 years | 8-8.5 cm |
| 8-9 years | 9 cm |
| 10-13 years | 10 cm |
| 14-17 years old | 13 cm |
Table 2.
Unified criteria for arterial hypotension in children
| Age | Systolic blood pressure (mm Hg) | Diastolic blood pressure (mm Hg) |
| 7-9 years | 80 | 40 |
| 10-13 years | 85 | 45 |
| 14-15 years old | 90 | 50 |
| 16-17 years old | 90 | 55 |
Daily blood pressure monitoring (ABPM) allows you to identify the initial manifestations of arterial dystonia - changes in the circadian rhythm and blood pressure. When assessing the hypotension index (the time of decrease in blood pressure during the day), it is necessary to remember that its value above 25% indicates pathology: with labile hypotension, the index fluctuates between 25-50%, with a stable form -50%.
The clinical picture of arterial hypotension is dominated by psychoneurological disorders in the form of emotional lability, irritability, weather sensitivity, anxiety, various phobias, decreased physical and mental activity, respiratory neurosis in the form of sighs and a feeling of lack of air, poor tolerance of stuffy rooms is common. Patients report dyspeptic disorders in the form of nausea, less often vomiting, aerophagia, complain of spastic abdominal pain, flatulence, intestinal dyskinesia, constipation, often of a spastic nature. Possible cardialgia, a feeling of interruptions in the heart.
Cephalgia deserves special attention, often in the morning, often immediately after sleep. They are accompanied by weakness and malaise. Headaches are paroxysmal, pulsating, intense, and are often localized in the frontoparietal region. Pain is provoked by weather fluctuations and emotional stress. Dizziness occurs when changing body position. Provoking moments, as a rule, are prolonged orthostasis, prolonged stay in a stuffy room.
Criteria for the severity of arterial hypotension are:
- stable nature of arterial hypotension;
— intensity of cardialgia;
— presence and frequency of vegetative crises;
— degree of psychophysical maladjustment;
- orthostatic dysregulation and fainting.
Fainting (syncope) is a common symptom of severe arterial hypotension. Syncope is a sudden short-term loss of consciousness and a violation of postural tone with a disorder of cardiovascular and respiratory activity. Clinical manifestations of fainting are characterized by dizziness, tinnitus, darkening of the eyes, severe weakness, and unpleasant sensations in the abdominal cavity. Then there is a decrease in muscle tone, “sagging to the floor,” pallor, shallow breathing, weakness, and a decrease in blood pressure. After emergency measures are provided or independently, consciousness and correct orientation are restored, skin hyperhidrosis and bradycardia are determined, and dizziness and nausea often persist.
A careful differential diagnosis is necessary between fainting that occurs against the background of arterial hypotension of neurovegetative origin and fainting of another origin - cardiogenic, neurogenic, fainting due to endocrine diseases, etc.
Diagnosis of arterial hypotension includes:
1. Collection of genealogical and clinical-anamnestic data;
2. Carrying out ECG, ECHO-CG, ABPM;
3. EEG registration;
4. Study of autonomic homeostasis;
5. Clinical and biochemical blood tests (activity indicators, glucose, electrolytes, cholesterol, etc.);
6. According to indications, psychological testing is carried out;
7. Consultations with specialists to exclude symptomatic (secondary) arterial hypotension;
Treatment of arterial hypotension includes non-drug and drug treatments. In case of labile arterial hypotension, preference is given to non-drug effects. Persistent and prolonged arterial hypotension requires the combined use of non-drug and drug therapy.
Non-drug treatment includes: normalization of the daily routine, including rest and work patterns. A full night's sleep is necessary, and daytime rest is encouraged. Daily exposure to fresh air is recommended for up to 2 hours a day. Morning exercises are required, followed by water procedures, available at any home, that promote vascular training. The diet involves eating 4-6 times a day without limiting salt in an optimal water regime. Massage is indicated - general, cervical-collar area, hands, calf muscles.
Physiotherapeutic methods of treatment that have a stimulating effect are widely used for arterial hypotension: electrophoresis according to Vermeule on the collar area with solutions of magnesium sulfate, caffeine, mesatone, bromocaffeine. Electrosleep with a frequency of 10 Hz is used. Acupuncture optimizes neurovegetative balance and improves microcirculation. Water procedures—fan and circular showers, underwater massage showers—have proven themselves well among children and adolescents. Therapeutic baths have a positive effect on vascular tone. It is important to use various methods of psychotherapy in treatment that correct the patient’s relationship with the environment.
If non-drug therapy is ineffective, the following groups of drugs are used: adaptogens, anticholinergic drugs, nootropics and cerebroprotectors, antioxidants, and, if necessary, tranquilizers and antidepressants. As a rule, drug treatment of arterial hypotension begins with adaptogens that gently stimulate the central nervous system, and most importantly, have a positive effect on the sympathetic division of the autonomic nervous system. The most commonly used are plant adaptogens (Table 3). They have an adrenomimetic effect, contribute to the formation of adaptive reactions by regulating the balance between the processes of excitation and inhibition in the cortex and subcortical vegetative formations. Adaptogens are prescribed once a day in the morning with a course of treatment lasting up to three weeks.
Table 3.
Adaptogens
| Adaptogen groups | Herbal remedies |
| General tonic | Trifol, dandelion, fennel, spirullina, kelp, nettle, echinacea, thyme, centaury |
| Adaptogens with a moderate stimulating effect, II series | Green tea, licorice, coffee tree |
| Adaptogens with the greatest stimulating effect, first row | Ginseng, Schisandra chinensis, zamanika, Rhodiola rosea, aralia |
It is necessary to remember the undesirable effects of adaptogens:
- the phenomenon of exhaustion of the nervous system due to disorderly, uncontrolled use;
- increased blood pressure and psycho-emotional agitation;
- the phenomenon of overdose with the development of paradoxical reactions;
Adaptogens of groups 1 and 2 are not advisable to prescribe for heart rhythm disturbances; Schisandra is contraindicated for intracranial hypertension, ginseng is contraindicated for bleeding.
Of the anticholinergic drugs, the most widely used are combination preparations of belladonna - belloid, bellataminal, bellaspon.
The use of nootropic drugs is pathogenetically justified in patients with arterial hypotension, since this group of patients quite often suffers from cerebral insufficiency and immaturity of cortical-subcortical relationships. Glycine, piracetam, phenibut, Cortexin and GABAergic drugs have proven themselves to be effective in pediatric practice.
In order to improve cerebral hemodynamics and microcirculation, a course of treatment with cinnarizine and vinpocetine is used. Actovegin and Oxibral have an optimizing metabolic effect.
The use of antioxidant therapy and correction of energy-deficient diathesis are also necessary for patients with arterial hypotension.
Indications for prescribing tranquilizers are pronounced neurotic manifestations, emotional stress, phobias, and hidden anxiety. Preference is given to activating tranquilizers and daytime anxiolytics (trioxazine, grandaxin, etc.).
Thus, an integrated, etiopathogenetic approach to the treatment of arterial hypotension makes it possible to monitor its course, prevent its progressive course and decrease in the quality of life of patients.
N.N. Arkhipova
Kazan State Medical Academy
Literature:
1. Belokon N.A., Kuberger M.B. Diseases of the heart and blood vessels in children: A guide for doctors in 2 volumes. - M.; Medicine,!1987.T.1-P.303-337
2. Korovina N.A. al. Autonomic dystonia in children // Guide for doctors. M., 2006, 67 p.
3. Kushnir S.M., Antonova L.K. Autonomic dysfunction and autonomic dystonia. - Tver., 2007, 215 p.
4. Kurochkin A.A. et al. Neurocirculatory dystonia in children and adolescents (literature review and clinician’s view on controversial issues of terminology, etiology, pathogenesis, clinical picture and treatment) // Russian Bulletin of Perinatology and Pediatrics. - 1999. - No. 6. - P. 21-25.
5. Leontyeva I.V. Lectures on pediatric cardiology. - M., 2005. P. 405-503.
6. Guide to pharmacotherapy in pediatrics and pediatric surgery: T.5.-Clinical cardiology. - ed. prof. Belozerova Yu.M.. - M., 2004.-P.170-176.
7. Tvorogova T.M., Korovina N.A. Arterial hypotension in children and adolescents.//Russian medical journal.-2007.-No. 21.- P.1519-1524.
Preventative examinations of newborns by a neurologist
An experienced neurologist will be able to promptly diagnose a disease or developmental disorder of a child, prescribe additional diagnostic procedures: functional and ultrasound studies, conduct complex treatment, and involve the required specialists in the treatment process: physical therapy doctor, physiotherapist, psychologist, speech therapist, osteopath and others.
It is important to identify existing diseases in time, in the first months of life, in order to prevent delays in the child’s development or limitation of his capabilities.
The sooner treatment is prescribed, the more optimistic the prognosis will be. Timely, comprehensive therapy will save the child from age-related complications and many psychological problems, ensure his full development and create conditions for achievements in life.
Consultation with a neurologist is most effective at home
In order to examine the child and assess muscle tone, the child must be calm and should not cry at the time of examination or before the examination (crying can greatly affect tone). Children with altered tone react more sharply to changes in the environment, unfamiliar smells or sounds. Any fear or agitation of the baby can distort the results of the examination.
Therefore, in order for an examination by a neurologist to be as effective as possible, we recommend calling a neurologist to the newborn’s home.
Routine observation of newborns by a neurologist
Routine examinations by a neurologist are especially important for infants. During this period, the doctor can identify early manifestations of congenital diseases, such as hydrocephalus, cerebral palsy, malformations of the brain and spinal cord, and timely detect acquired diseases.
To prevent and timely identify possible disorders of the peripheral nervous system, brain and spinal cord, children in the first years of life need to be regularly examined by a pediatric neurologist.
A neurologist should examine a newborn baby:
- In the first 30 days after birth. If there are risk factors, several consecutive examinations are carried out during this period.
- Every 3 months during the first year of life.
- Every 6 months until the child reaches the age of three.
- Annual examinations up to 6 years of age.
- Preventive examinations during the period of adaptation to social life (7-11 years) and active puberty (11-14 years).
When you need to urgently call a neurologist at home
In newborns and children of the first year of life
- In a calm state, when crying or excited, the baby’s hands or chin begin to tremble.
- The baby's sleep is disturbed: there are difficulties falling asleep, shallow and restless sleep with frequent awakenings.
- When the fontanelle bulges.
- If the fontanel is painful, crying when touched)
- With frequent and profuse regurgitation, even with small amounts of food.
- When any convulsions occur.
- If the child has a forced position of the legs: with the toes tucked, or the feet are extended as if the child is “standing on tiptoes.”
- With monotonous crying, refusal to feed, sluggish sucking.
In children older than one year
- For severe or frequent headaches.
- For neck pain.
- If the child complains of shooting or piercing pain in the back when moving.
- For muscle twitching or tics.
- If your child experiences fainting.
- With constant absent-mindedness.
- With forgetfulness, sudden changes in mood.
- If the child experiences unmotivated crying or aggression.
- If speech, reading, or writing impairment is obvious.
- With a sharp decrease or impairment of vision, taste, hearing, and smell.
- With low learning ability, progressive educational retardation.
- With “bad behavior”, uncontrollability.
- With increased fatigue.
- If you see a lack or a sharp deterioration in contacts with other children.
- For bedwetting of urine or feces (for children over 5 years old, if it occurs more than 2 times a week).
- If a change in gait is obvious, refusal to stand on a leg.
- In case of sleep disturbance, if there is difficulty falling asleep.
In case of head injuries, loss of consciousness, severe convulsions, or the child’s condition is unclear, CALL AN AMBULANCE IMMEDIATELY.
Arterial hypotension. Symptoms
A sharp drop in blood pressure under the influence of the above triggering factors has characteristic manifestations:
- instability;
- weakness;
- nausea and dizziness;
- heartbeat;
- feeling of "cotton legs"
- visual and speech impairments;
- psycho-emotional experiences of anxiety and fear;
- fainting.
Chronic arterial hypotension (both primary and acquired) is expressed in:
- headache and dizziness;
- palpitations, shortness of breath during physical and emotional stress
- chronic fatigue and high fatigue;
- sleep disorders;
- unsteadiness when walking;
- feeling hot or cold, sweating, numbness;
- deterioration of memory and attention;
- poor tolerance to stuffiness, heat, transport, heights;
- frequent fainting.