Coarctation of the aorta (CA) is a congenital segmental narrowing of the aorta, most often located after the origin of the left subclavian artery (Fig. 1). This pathology was first described by Meckel in 1750, the term “coarctation” was proposed in 1838 by Mercier [1].
Fig. 1: Aorta normally and with coarctation (diagram)
Coarctation of the aorta belongs to a group of fairly common diseases. Thus, among children and adults with congenital heart and vascular defects, CA occurs in 10% of cases. Among newborns with congenital heart defects, the incidence of CA can reach 20% [1].
The disease is 2-2.5 times more common in males [2]. Familial cases of coarctation of the aorta are rare. According to A.Becker, J.Keith, D.Fyler, in 70% of infants with coarctation of the aorta it is combined with a patent aortic duct (PDA), in 53% - with a ventricular septal defect (VSD), in 14% - with stenosis aorta, in 3-5% - with stenosis or insufficiency of the mitral valve [2,3,4]. Often (in approximately 60-70% of cases), a combination of aortic coarctation with several congenital heart defects (CHD) is noted [5]. Isolated coarctation of the aorta is observed only in 15-18% of patients with a complicated course of the disease in infancy [6].
The cause of coarctation of the aorta has not been definitively established, but several theories have been proposed. The most famous of them, the classical theory of Skoda (Skoda J., 1855), explains the narrowing of the aorta by closure of the PDA, as a result of which the adjacent area of the aorta is involved in the process [7]. Some authors associate the pathogenesis of this pathology with a discrepancy between the diameters of the newborn aorta in the area of the isthmus and the descending part (the isthmus is usually 30% narrower than the ascending and descending parts) [6].
In 1903, L. Bonnet proposed the first classification, highlighting infantile and adult variants of the defect, which were later renamed preductal and postductal forms [8]. Currently, there are several classifications based on different criteria. Thus, depending on the age of patients, CA is distinguished in infants, CA in adolescents and adults [4,9]. According to the localization of the narrowing, preductal, juxtaductal and postductal variants of CA are distinguished. The postductal variant of the coronary artery is characterized by the location of the narrowing distal to the place where the PDA flows into the aorta (from the Latin ductus - duct). The preductal variant is detected when the aorta narrows proximal to the point where the PDA enters it. Juxtaductal coarctation is detected when the narrowing is localized directly at the junction of the aortic duct into the aorta (Fig. 2)
Fig. 2: Preductal, juxtaductal and postductal variants of CA (scheme) 1. ascending aorta; 2. pulmonary artery; 3. aortic duct; 4.descending aorta; 5. brachiocervical trunk; 6. left common carotid artery; 7.left subclavian artery; A. juxtaductal coarctation; B. preductal coarctation; C. postductal coarctation
Depending on the concomitant defect, isolated coarctation of the aorta, coarctation of the aorta in combination with a patent aortic duct, coarctation of the aorta with VSD, and coarctation of the aorta in combination with other congenital heart defects are identified.
In the differential diagnosis of patients with arterial hypertension, it is mandatory to exclude CA, which is often discovered by chance during the examination of such patients [10]. The main diagnostic guidelines are high blood pressure (BP) in the upper extremities at a young age, absence or decreased pulse in the lower extremities, disproportionate development of the upper half of the body with hypotrophy of the lower half, acrocyanosis and chilliness of the extremities (especially legs). It is the absence or weakening of the pulse in the lower extremities, arterial hypertension in the upper half of the body and the systolic pressure gradient between the upper and lower extremities that are the main signs of CA [1]. Auscultation can reveal systolic and diastolic murmurs over the aorta, over the heart area and in the projection of the intercostal arteries. In patients with CA, upon palpation, pulsation of the intercostal arteries is determined, and pulsation in the jugular fossa may be detected. X-rays of the chest organs show usurization of the lower contours of the ribs (due to hypertrophy of the intercostal arteries). When performing a computed tomography scan of the chest and angiography of the thoracic aorta, narrowing of the aorta in the area of its isthmus can be detected.
In the classic course of the disease, about ¾ of patients with aortic coarctation die before the age of 40 years. The average life expectancy of such patients is 34 years [11].
The most effective treatment for coronary artery disease is surgical correction. The optimal age for surgery is from 3 to 20 years [12]. Mortality in the immediate postoperative period is 8.3% [7]. The first successful operation for coarctation of the aorta in a 12-year-old boy was performed by the Swedish surgeon C. Crafoord in 1944 [9]. In the USSR, the first operation was performed by E.N. Meshalkin in 1955 [13].
We present a description of two patients with coarctation of the aorta. Patient M., 25 years old, a worker at a poultry factory, was transferred from the obstetric and observational department of the Republican Clinical Hospital No. 1 to the cardiology department with a periodic increase in blood pressure to 220/120 mm Hg. (adapted to blood pressure 170-180/90 mm Hg), attacks of palpitations lasting up to 2 minutes, accompanied by headache, acrocyanosis and chilliness of the fingers, complaints of weakness and rapid fatigue of the lower extremities with little physical exertion, inspiratory shortness of breath and general weakness after significant physical activity (climbing to the 4th floor). At the age of 21, during a medical examination, an increase in blood pressure to 170/100 mm Hg was first detected. There were no subjective sensations; she did not receive antihypertensive therapy. At the age of 24, she became pregnant; at the 5th month, an examination at the antenatal clinic revealed an increase in blood pressure to 200/130 mm Hg. On the recommendation of the antenatal clinic doctor, a surgical termination of pregnancy (caesarean section) was performed at 26 weeks. According to the patient, as a child she was seen by a doctor with a diagnosis of rheumatism.
Upon examination, it was revealed: by percussion, the boundaries of relative cardiac dullness were expanded to the left by 2 cm. On auscultation, systolic and diastolic murmurs were heard above the apex of the heart and above the aorta, and a click of the opening of the mitral valve. When auscultating the intercostal arteries, systolic murmurs are heard. Blood pressure in both arms is 190/100 mm Hg. In the lower extremities, pulse and blood pressure are not determined.
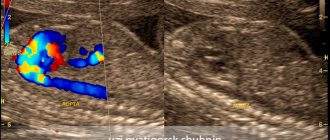
The ECG shows sinus tachycardia with deviation of the electrical axis of the heart to the right, hypertrophy of both atria. An X-ray of the chest organs revealed an expansion of the heart shadow to the left and a narrowing of the lower contours of the ribs. X-ray computed tomography revealed a local narrowing of the aortic lumen to 9-10 mm at the level of the transition of the arch to the descending section (Fig. 3, 4).
Fig. 3: Computed tomogram of the chest organs of patient M. The arrow marks the place of narrowing Fig. 4: Computed tomogram of the chest organs of patient M
Echocardioscopy revealed a combined aortic defect (aortic stenosis, second degree aortic valve insufficiency); combined mitral disease (stenosis of the left atrioventricular orifice, first degree insufficiency); left atrium enlargement; tricuspid regurgitation of the first degree. Rheovasography revealed a decrease in blood pressure in the legs, a marked decrease in total blood flow in the upper extremities, and a sharp decrease in total blood flow in the lower extremities on both sides. According to the conclusion of FGDS, it was noted: compression of the thoracic esophagus from the outside (by the aorta).
When analyzing the examination results, CA was suspected. The patient was diagnosed with : Rheumatism, inactive phase. Combined mitral defect: moderate stenosis of the left AV orifice and stage I mitral insufficiency. Combined aortic disease with predominant stenosis of the aortic mouth, moderate aortic insufficiency. UPS. Coarctation of the descending thoracic aorta. Arterial hypertension stage III. CHF I. FC II.
It should be noted that this case is an example when the arterial hypertension syndrome in a young patient was not deciphered in time. The lack of alertness of doctors regarding coarctation of the aorta did not allow us to suspect this pathology. In a young patient (21 years old), we should primarily talk about secondary arterial hypertension. At the same time, despite the obvious simplicity of diagnosis and the typical clinical picture of the patient, the doctors’ conservative understanding of arterial hypertension syndrome did not allow a diagnosis of CA even at its first manifestation.
The patient was recommended for surgical treatment - resection of aortic coarctation with prosthetics in the cardiac surgery department of the Interregional Clinical Diagnostic Center. With surgical correction, the prognosis for this patient is favorable.
The second patient P., 40 years old, is observed in the city rheumatology center with a diagnosis of ankylosing spondylitis. The main complaints are pain in the cervical spine, in the right shoulder joint, limitation of movements in all parts of the spine; notes a periodic increase in blood pressure to 180/100 mm Hg. (no headaches). A clinical blood test revealed an acceleration of ESR (40 mm/hour), slight leukocytosis (10.0*109), and an increase in a1- and a2-globulins (12.0% and 10.3%, respectively). X-rays of the lumbosacral spine reveal sacroiliitis and straightening of the lumbar lordosis.
An increase in blood pressure was first detected at the age of 16 (140/90 mm Hg), but was not subjectively manifested in any way. At the age of 18, he was diagnosed with VSD while serving in the army, and therefore was demobilized early. Upon careful questioning, it was possible to identify two episodes of dizziness with loss of consciousness, and several cases of nosebleeds. He has noted chilliness in his extremities since childhood. The examination revealed: blood pressure in the right arm 130/75 mm Hg, in the left arm 130/80 mm Hg, blood pressure in the right leg 125/100 mm Hg, in the left leg 130/100 mm Hg .st. Pulsation in the legs is detectable, but reduced. Upon examination, a pronounced venous network is revealed on the anterior chest wall. During auscultation, systolic murmurs are heard along the left edge of the sternum and in the intercostal spaces on both sides.
Fig. 5: X-ray of the chest organs of patient P. Arrows mark the usuration of the ribs and both arches of the double aortic arch
CA was suspected on the basis of a chest x-ray (Fig. 5), which revealed: multiple usurations along the lower edges of the ribs on both sides, the aorta is dilated, thickened, the arch has a double bend, with increased pulsation of the contour of the shadow, the shadow of the artery extending from it is expanded . The contrasted esophagus goes around both aortic arches. Echocardioscopy revealed congenital heart disease—muscular VSD. Compaction of the walls of the aorta, the cusps of the aortic valve. Combined aortic disease (aortic stenosis, second degree aortic valve insufficiency). Hypertrophy of the IVS myocardium. Mitral tricuspid regurgitation of the second degree.
Based on the results of the analysis of the examination, the patient was diagnosed with congenital heart disease - muscular VSD. Combined aortic disease (aortic stenosis, aortic valve insufficiency degree II). Hypertrophy of the IVS myocardium. Mitral and tricuspid regurgitation. Coarctation of the aortic arch. Ankylosing spondylitis, activity II, rapidly progressive course, central form.
In this case, the combination of acquired rheumatic (aortitis) and congenital (coarctation of the aorta) defects is interesting. Damage to the cardiovascular system occurs in 20-22% of patients with ankylosing spondylitis. The most characteristic in this case is isolated insufficiency of the aortic valve (determined in 1.3% of patients) due to inflammatory changes both in the aorta itself with its subsequent expansion, and in the leaflets of the aortic valve. Aortic valve insufficiency usually develops during a long course of ankylosing spondylitis with high clinical and laboratory activity. It is possible to develop an aortic aneurysm. There are known cases of the development of aortitis and aortic disease before the appearance of the first clinical and radiological symptoms of ankylosing spondylitis. Myocarditis, pericarditis and myocardial dystrophy may also develop.
The asymptomatic course of aortic coarctation in this patient is manifested in the absence of a clear pattern of inhibition of blood flow distal to the site of aortic narrowing. This variant of the disease can be observed in rare cases of coarctation of the aorta with a double aortic arch as in this patient (Fig. 6).
Fig. 6: Double aortic arch (diagram). The arrow marks the place of bifurcation of the aortic arch
When CA is combined with a small VSD, an asymptomatic course of the disease until adulthood is also possible [3]. Considering such changes, causing the absence of a clear clinical picture, it was quite difficult to suspect CA in this patient.
The patient we observed refused surgical treatment due to the absence of any complaints from the cardiovascular system. Based on the literature data, the prognosis for a patient with asymptomatic CA is favorable. Cases of a favorable course of this pathology are extremely rare, when CA is an accidental finding during an instrumental examination in the absence of clinical symptoms throughout life. In the available literature in recent years, a description of only 8 similar cases has been found, where the life expectancy of patients was more than 55 years [1,14,15,16,17,18,19,20]. Among them, one patient is female, the other seven are male. In a woman, CA was combined with coronary heart disease, in other patients - with VSD, aneurysm of the intercostal artery, double mitral valve and other congenital heart defects. In all cases, patients did not notice an increase in blood pressure, or blood pressure increased slightly.
AND . G . Salikhov 1 , S. A . Lapshina 1 , G. E. _ Fattakhova 1 , R. Z. _ Abdrakipov 2 , R. G . Mukhina 3
Kazan State Medical University 1
Republican Clinical Hospital2
City Rheumatology Center3
Salikhov Ildar Gazimdzhanovich - Doctor of Medical Sciences, Professor, Head of the Department of Hospital Therapy of KSMU
Literature:
1. Matchin Yu. G., Kozlov S. G., Lyakishev A.A. and others. Favorable course of coarctation of the aorta. - Cardiology, 1991. T.31, No. 12; pp. 105-106
2. Fyler DC Report of the New England Regional Infant Cardiac Program. Pediatrics, 1980. 65 (suppl); p. 376-461.
3. Becker AE, Becker MJ, Edwards JE Anomalies associated with Coarctation of aorta-particular reference to infancy. Circulation, 1970. 41; p.1067-1075.
4. Keith JD Coarctation of the aorta. in: Keith JD, Rowe RD, Vlad P., editors. Heart disease in infancy and childhood. 3rd edition. New York: Macmillan, 1978. p.736-760.
5. Sinha SN Kardatzke ML, Colo RB, et al. Coarctation of the aorta in infancy. Circulation, 1969. 40; p. 385-398.
6. Tawes RL, Aberdeen E, Waterston DJ et al. Coarctation of the aorta in infants and children: a review of 333 operative cases including 170 infants. Circulation, 1969. 39(suppl); p. 173-184.
7. Skoda J. Protokell der sections-sitzung fur physiologie and pathologie. Wochenblatt der zeitschrift der Kaiserlich-Konighchen Gesselshaft der aerzte zu Wien, 1855. 19 Oct.; p.710-722; (Quoted by Ho and Anderson, 1979).
8. Bonnet LM Sur la lesion dite stenose congenitale de l'aorta dans la region. Del isthme Revue de medicine, 1903. 23; p. 108, 225, 385
9. De Leval M. Coarctation of the aorta and interruption of the aortic arch. Surgery for congenital heart defects. London, 1983. p.213-225.
10. Schuster SR, Gross R., E. Surgery for coarctation of the aorta: a review of 500 cases. J. thorac. Cardiovascular Surgery., 1962. 43; p. 54-70.
11. Campbell M. Natural history of Coarctation of the aorta. Brit.Heart J., 1970. Sep., 32(5); p. 633-40.
12. Rao PS Baloon angioplasty of native coarctation: a review. Clin. Cardiol., 1989. 12(11); p. 618-628
13. Burakovsky V. Sh., Bockeria L. A. Cardiovascular surgery. M. Medicine; 1989. pp. 298-310.
14. Convens C, Vermeersch P, Paelinck B et al. Aortic coarctation: a rare and unexpected caused of secondary arterial hypertension in the elderly. Cathet Cardiovasc Diagn., 1996. 39; p. 71-74.
15. Erdal AC, Silistreli E., Karabay O., et al. Asymptomatic aortic coarctation associated with loss of luminal continuity and intercostals artery aneurysm. Torino, 2004 Feb; 45(1); p.93-4.
16. Miro O, Jimenes S, Gonzales J et al. Highly effective compensatory mechanisms in a 76-year-old man with a coarctation of the aorta. Cardiology, 1999. 92; p. 284-286.
17. Patel Y., Jilani MI, Cho K. Coarctation of the aorta presenting in a 79-year-old male. Thorac Cardiovasc Surg., 1998. 46; p. 158-160.
18. Proenca G., Freitas A., Baptista S. et al. Double orifice mitral valve in an asymptomatic adult with an unusual combination of congenital malformations: a case report. Rev. Port. Cardiol., 2004. Feb., 23(2); p.233-236
19. Servet Cevik, Cemil Izgi, Cihan Cevik Asymptomatic Severe Aortic Coarctation in an 80-year-old Man. Tex Heart Inst J., 2004. 31(4); p. 429-431.
20. Vaquero F., Zorita A., Samos R., et al. Ascending aorta-supraceliac aorta bypass. Correction of a case of atypical Coarctation in the adult. Angiologia, 1993. 45(3); p. 87-90.
Types of Congenital Heart Defects
Congenital heart defects are most common in premature babies with low birth weight. The immediate causes of violations in the design of this organ are not fully understood. The coexistence of at least several genetic and environmental factors has a major influence on the occurrence of heart defects. The risk of their occurrence in a child increases when:
- A woman suffered from rubella in the first trimester of pregnancy.
- The pregnant woman smoked cigarettes, drank alcohol, or used drugs.
- Woman with diabetes.
- The child developed chromosomal abnormalities (including Down syndrome and Turner syndrome).
Heart defects can affect various structures of the organ, including the valves, ventricles, and blood vessels. Taking this into account it stands out:
- Defects in the parts of the heart.
- Abnormal abnormalities in large arteries.
- Improper blood flow to the heart.
- Partial or total stenosis of valves and blood vessels.
Diagnosis of acquired and congenital heart defects
The basis for diagnosing both congenital and acquired heart defects is echocardiography (ECHO), which is a visual examination that allows for non-invasive examination of the structures of the heart - valves, chambers, atria and blood vessels. The most common type is transthoracic echocardiography. Contraindications for this test are obesity (BMI over 35), chronic obstructive pulmonary disease (COPD). Another test used in diagnosing acquired and congenital heart defects is a chest x-ray (X-ray), which can accurately determine the location, size and shape of the heart. It is important to note that the most popular cardiac examination, electrocardiography (ECG), cannot be the main examination for suspected heart disease.
Mitral valve narrowing
Mitral valve narrowing is a relatively rarely diagnosed heart defect. This leads to impaired blood flow, increased pressure in the left atrium and, as a result, overload of the right ventricle. This defect occurs in three variants: subvalvular, valvular and supravalvular. Characteristic symptoms of this heart defect are: shortness of breath, fatigue (decreased tolerance to physical activity), lack of body weight. Due to the high risk of serious complications, the recommended treatment for this heart defect is implantation of an artificial or biological valve. It is important to note that people with artificial or biological valves must take anticoagulants throughout their lives because they often have thromboembolic complications.
Section: Articles Tags: cardiology
Narrowing of the pulmonary artery trunk
Pulmonary artery stenosis is a relatively common heart defect in newborns - it is diagnosed in approximately 6-9% of children. This mild heart defect usually causes no symptoms. For this reason, it is usually diagnosed in adolescence or adulthood as a result of shortness of breath and a significant decrease in the body's physical performance. It is important to note that pulmonary artery narrowing does not usually require surgery, only a pulmonary valvuloplasty procedure, which involves widening the valve. A contraindication to this procedure is the occurrence of a dysplastic valve (not fully formed). In this case, it is necessary to perform heart surgery, which involves widening the valve using a special patch.