Definition of disease
The largest artery in the human body is the aorta. This vessel of the systemic circulation leaves the left ventricle and is subjected to high loads, since it receives the maximum pressure of blood flow. Therefore, an important and necessary property of the aorta is its elasticity and density.
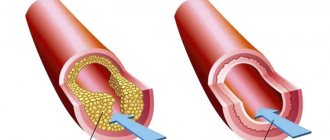
Calcification is the deposition and gradual accumulation of calcium salts, forming calcified plaques, on the walls of the aortic valve. The danger of this process is that as calcium penetrates into the walls of the vessel, they become more fragile, brittle and less elastic.
This, in turn, poses a threat to human life, because when blood pressure increases, the calcified walls of the vessel may not withstand and rupture, which will lead to death. With calcinosis, calcium dissolved in body fluids (including blood) is deposited in tissues and blood vessels. This happens when there is an excess of calcium in the blood.
Content:
Causes of aortic calcification
The reasons for an excessive amount of calcium salts in the blood, which significantly increases the likelihood of aortic calcification, may be the following:
- With age, calcium is increasingly washed out of the bones, entering the blood in excess quantities.
- Various kidney diseases, in which the kidneys are unable to remove the required amount of calcium from the body and it enters the blood.
- In some pathological conditions of the intestine, increased absorption of calcium into the blood also occurs.
- Sometimes there are deviations in the process of calcium absorption by bone tissue (complete absence or insufficient absorption). The remaining calcium enters the blood.
Possible causes of aortic calcification also include bad habits, poor diet, stress, heart disease, heredity, physical inactivity, diabetes, and obesity.
To prevent and early diagnose aortic calcification, you should have regular blood tests. A referral can be obtained from a general practitioner or cardiologist. If the analysis shows an increased level of calcium in the blood, then you should look for the cause of this deviation.
Material and methods
The open comparative study included patients aged 50 to 75 years with a high risk of developing cardiovascular complications according to the SCORE scale (more than 5%), atherosclerosis of the brachiocephalic arteries and decreased BMD.
Patients with normal BMD formed the control group. The patients underwent a comprehensive examination of the cardiovascular system at the Scientific Dispensary Department of the National Medical Research Center for Cardiology: general clinical examination, biochemical blood test, study of the levels of 25-hydroxyvitamin D (25 (OH)D) and parathyroid hormone (PTH), OPG, and also applanation tonometry, volumetric sphygmography, dual-energy X-ray absorptiometry (DEXA), multislice computed tomography (MSCT) of the coronary arteries (CA) and thoracic aorta. The study did not include patients with coronary artery disease who had suffered a cerebrovascular accident, transient ischemic attack, as well as those with secondary causes of AP, diabetes mellitus, taking medications that affect bone metabolism, and statins within the last 6 months. A biochemical blood test was performed on an Architect C8000 selective analyzer (Abbot, USA), including determination of total cholesterol (TC), low-density lipoprotein cholesterol (LDL), high-density lipoprotein cholesterol (HDL), triglyceride levels (TG), calcium, phosphorus, creatinine with calculation of glomerular filtration rate (GFR) using the MDRD formula. The content of 25 (OH)D and PTH in the blood plasma was determined by the immunochemical method with electrochemiluminescence detection (ECLIA) on the ELECSYS 2010 analyzer. The concentration of OPG in the blood serum was determined by the enzyme-linked immunosorbent assay (ELISA) in all 68 patients with impaired BMD and in 5 patients with normal BMD. BMD. Applanation tonometry to determine the parameters of central pressure (systolic - SBP, diastolic - DBP and pulse - PBP in the aorta, augmentation index - AI) and pulse wave velocity in the carotid-femoral segment (PWVcf), reflecting the stiffness of the aorta, was performed using the Sphygmocor device (“ AtcorMedical, Australia) using a high-quality Millar applanation sensor using a standard method (direct distance measuring method · 0.8). Pulse wave velocity at the brachiomalleolar segment (PWV) was measured using volumetric sphygmography, which was performed using a VaseraVS-1000 device (FukudaDenshi, Japan). DEXA of the femoral neck (FNC) and lumbar spine to determine BMD was performed using a HologycDiscovery device (USA) according to standard methods. According to the Russian recommendations for the diagnosis and treatment of AP, the diagnosis of “osteopenia” was established when the T-criterion for BMD in the lumbar spine or BBC was from –1 to –2.5 SD, AP – when the T-criterion was –2.5 SD and below. T-scores up to –1 SD from peak bone mass corresponded to normal BMD. To determine the calcium index (CI) of the coronary artery and thoracic aorta, MSCT was performed on a 64-spiral computed tomograph (Toshiba Aquilion, Japan) using a standard patient position on the basis of the tomography department of the National Medical Research Center of Cardiology (headed by Academician of the Russian Academy of Sciences, Prof. S. K. Ternova). CI of the coronary artery and thoracic aorta was assessed from the aortic root (above the origin of the coronary artery) to the apex of the heart according to the standard method. Calculation K.I. were performed according to Agatson using special computer software. For each patient, CI in the coronary artery and thoracic aorta was determined for the area of the calcified area if its density was more than 130 HU. When CI=0, the absence of aortic calcification and CCA was stated. Statistical calculations were carried out using the Statistica 8.0 software package. The main parameters of the studied indicators are presented in the form of a median and values of the lower (25%) and upper (75%) quantiles. A distribution in which the Kolmogorov–Smirnov difference criterion from the theoretically normal Gaussian distribution was more than 0.05 in significance was accepted as normal. Comparison of two groups was carried out using the Mann-Whitney test. Associations between variables were identified using Spearman's correlation coefficient. Differences at p
<0.05 was considered statistically significant.
Research structure.
Based on the results of densitometry in accordance with the T-criterion, patients with a high risk of developing CVD complications were divided into 3 groups: 1st group consisted of 18 patients with normal BMD, 2nd - 48 with osteopenia and 3rd - 20 with O.P. . After further examination, a comparative group analysis was carried out.
Aortic stenosis
Aortic stenosis is a fusion of the aortic valve leaflets. Since this pathology leads to a narrowing of the valve opening, the release of blood flow into the aorta is difficult, resulting in a significant increase in the load on the left ventricle, which leads to myocardial hypertrophy.
There are three forms of aortic stenosis: subvalvular, valvular and supravalvular. Among patients with heart defects, aortic stenosis occurs in 84% of cases, and in men it is three times more common. Of all the forms of aortic stenosis, valvular stenosis is the most common. Aortic stenosis can also be congenital or acquired (90-97%). The supravalvular form is a congenital pathology.
Causes of aortic stenosis
The causes of acquired valvular or subvalvular stenosis can be aortic atherosclerosis, rheumatic valve disease, aortic calcification, and infective endocarditis. Sometimes the cause is diabetes mellitus, chronic kidney disease, Paget's disease, systemic lupus erythematosus or carcenoid syndrome.
Symptoms of aortic stenosis may not appear for a long time, especially at an early age. However, over time, the patient begins to complain of squeezing, aching pain in the chest (in the heart), shortness of breath, fainting, increased heart rate, nausea, and fatigue. Since cardiac output is reduced, this can lead to loss of consciousness. In later stages, aortic stenosis can cause a sudden attack of suffocation (cardiac asthma).
Also, in patients with aortic stenosis, the likelihood of sudden death increases, especially during physical activity. Hypertrophied myocardium causes acute coronary insufficiency and arrhythmias that threaten the patient’s life.
Symptoms and degrees of calcification
An increase in the concentration of free calcium in the blood serves as a provoking factor not only for calcification of the heart valves, but also for the development of pathologies such as heart failure, heart attack, and stroke. In this case, the symptoms of calcification are combined with signs of concomitant diseases.
Degree of development of calcification of heart valves
| Degree of disease | Signs of mitral valve pathology | Signs of aortic valve pathology |
| Compensated | An increase in the level of calcium in the blood, calcification of the valves. The tissues are compacted, there is a slight deterioration in hemodynamics | Difficulties arise with the opening of the valves, but the compensation mechanisms of the left ventricle keep the situation under control. During physical activity, minor heart pain is possible, which increases as the disease progresses. |
| Subcompensated | Shortness of breath during physical activity, tachycardia, arrhythmia, wet cough (sometimes with blood clots), hoarseness | Shortness of breath during physical activity, heart pain. Over time, signs of respiratory failure and aortic narrowing occur at rest |
| Decompensated | It develops rarely - with long-term ignoring of symptoms or an avalanche-like progression of the pathology. Pronounced weakness, shortness of breath with little physical activity. Cough with scarlet sputum, pale skin. Requires emergency medical attention | Signs of increased volume of both ventricles. Severe heart failure. The condition is extremely dangerous |
Aortic valve calcification
Patients do not feel any noticeable discomfort for a long time. Signs of pathology appear with stenosis of the aortic valve opening up to half of its passage. The progression of heart failure is accompanied by:
- dizziness;
- angina attacks;
- fainting with a sudden change in body position;
- shortness of breath at night;
- attacks of cardiac asthma and pulmonary edema (in severe cases).
- Aortic valve insufficiency: symptoms, diagnosis, treatment
The combination of heart pain and asthmatic attacks is very unfavorable. If left untreated, aortic valve calcification can cause bleeding in the lower digestive tract. If the valve opening is severely narrowed, sudden cardiac arrest may occur in elderly patients.
Mitral valve calcification
When blood stagnates in the pulmonary circulation, caused by calcification of the mitral valve, respiratory failure occurs, accompanied by characteristic symptoms. In case of serious damage, wheezing and shortness of breath at rest (to alleviate this, you need to sit down with your legs down) are observed, as well as pulmonary edema, characterized by:
- suffocation;
- wet wheezing when breathing;
- chest pain;
- fear of death.
Sometimes pinkish foam appears when exhaling. In such a case, the patient should be seated comfortably, with all the windows in the room opened, and tourniquets applied to his legs. You can hold a cotton swab soaked in alcohol to your nose and offer diuretics. Further therapy should be carried out exclusively in a hospital. Mitral valve calcification is similar in symptoms to signs of cardiosclerosis, rheumatism, and hypertension, so calcification often remains untreated, provoking the development of mitral valve insufficiency and stenosis.
Diagnosis of aortic stenosis
If symptoms of aortic stenosis appear, you should contact a cardiologist or begin an examination with a general practitioner. Using a stethoscope, the doctor will listen for a murmur over the aorta as the left ventricle contracts. An electrocardiogram can reveal ventricular hypertrophy. Ventricular enlargement can also be detected using x-ray. An echocardiogram uses ultrasound to evaluate the condition of the valves and heart muscle.
Also, an information research method is cardiac catheterization (insertion of a catheter into an artery). Provides information about intracardiac pressure, the location of the narrowing, the concentration of oxygen in the blood, the condition of the valve and the presence of a defect.
The most informative diagnostic method for making a decision on surgical intervention is an angiocardiographic study. It takes place in two stages: ventriculography and oorthography.
Author of the article:
Mochalov Pavel Alexandrovich |
Doctor of Medical Sciences therapist Education: Moscow Medical Institute named after. I. M. Sechenov, specialty - “General Medicine” in 1991, in 1993 “Occupational diseases”, in 1996 “Therapy”. Our authors
Diagnostics
Subjective diagnosis
Collecting a history of patient complaints
Diagnosis of CMC begins with collecting a history of the patient’s complaints; it is important, during a dialogue with the doctor, to outline all the existing complaints, since even a symptom that is insignificant in your opinion can lead the doctor to a specific diagnosis, which will allow you to reduce the search range in the future and save such precious time.
It is also important to describe to the doctor the history of this disease, i.e. when you felt any signs of the disease, how they progressed and in what sequence certain symptoms increased. Thus, CMC is characterized by an asymptomatic course of the disease at the beginning, followed (after several years, and sometimes even decades) by progression and a sharp deterioration in the condition, the appearance of shortness of breath, arrhythmias and cough with scarlet sputum.
You also need to describe to the doctor whether you have had similar cases of diseases in your family and what, in your opinion, could provoke the appearance of the above symptoms.
Objective diagnosis
Ultrasound examination of the heart
After you have told all the details of the disease, the doctor has a certain range of diseases, which needs to be narrowed down to one disease with the help of further laboratory and instrumental examination.
- First of all, the so-called clinical minimum tests are taken - a general blood test, a general urinalysis and a biochemical blood test. Most often, they will not be informative specifically for mitral stenosis, but will allow us to exclude other diseases accompanied by similar symptoms.
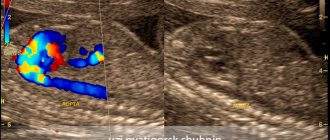
- Without a doubt, the gold standard for detecting calcification of the valve leaflets is an ultrasound examination of the heart, in which we can assess the completeness of the valve leaflets opening and detect various kinds of deposits and inclusions in the leaflets (for example, vegetations).
- An x-ray examination of the chest will also be relatively informative, and this is due to the fact that calcium salts are x-ray negative, so they can be seen during the examination. But this method cannot be applied specifically to CMB, since during X-ray examination we will not see the specific localization of calcification foci (such localization will be characteristic of both lung and mediastinal lesions), but as an additional research method, it has the right to life.
- A relatively new diagnostic method, computed tomography, is also quite effectively used, so if it is possible, then of course you can resort to CT.