After a stroke, neurological and visual disturbances often occur. In developed countries, 25% of cases of visual impairment are caused by stroke. In this case, vision loss can be complete or partial. Is it possible to restore vision after a stroke with the help of medical therapy, exercises and the right environment.
Temporary loss of vision
Temporary vision loss usually occurs suddenly in one eye, is painless and is described by patients as a sudden shadow. This condition may last for several minutes, then vision returns. Sometimes this condition repeats again and again. May occur in temporary vision loss in the second eye.
Typically, temporary vision loss occurs in elderly patients suffering from atherosclerosis and various vascular diseases. The cause may be small thrombi (blood clots) that break off from the arterial wall and enter the vessels of the eye, blocking the blood supply to the retina. When the blood clot is destroyed, it is destroyed and vision returns. Thrombosis or embolism usually occurs in the carotid or coronary (heart) arteries. An embolus may be cholesterol or calcium crystals.
This problem falls under the category of “ transient ischemic attacks ,” which can even result in a heart attack or stroke .
In this case, vascular studies are indicated and anticoagulants may be prescribed.
Acute vision loss also be caused by other problems, such as:
- Blockage of the vertebral arteries involved in the blood supply to the optic lobe of the brain.
- Increased intracranial pressure (the pressure of the fluid surrounding the brain). Increased intracranial pressure can cause immediate loss of vision, especially when the person changes position (for example, from a sitting position to a standing position).
- Spasm of the orbital artery, which supplies the retina with blood. It can also, although extremely rarely) cause temporary loss of vision in the eye.
Visual gymnastics after a stroke
To restore vision, it is recommended to perform a set of special exercises. Gymnastics helps maintain tone, strengthen muscles and brain function. All types of gymnastics are based on relaxing the eyes, reducing intraocular pressure, combating irritation and visual tension. Exercises can include any eye movements, focusing the gaze at different distances, drawing objects and images in the air. Long-term therapy makes the picture clearer and eliminates distortions.
If you experience partial vision loss after a stroke, exercise can help retrain your brain. Doctors include exercises in physical therapy. The simplest exercise is with a pencil. You need to hold the pencil at a distance of 45 cm and follow it with your eyes, moving the pencil up, down and to the sides. You can't move your head. Also, a pencil is placed in front of the patient’s face and moved to the sides.
After a stroke, it is recommended to work with puzzles and drawings. Patients can complete drawings of objects and shapes, play word games, and solve puzzles. Exercises like this help retrain the brain and help it identify objects using vision.
Even the simplest exercises help strengthen the muscles of the eyeballs, train muscle memory and track objects. Often after a stroke, muscle tone disappears. You can simply hold the upper eyelid with your fingers and try to close your eyes. Such exercises can prevent eye fatigue and relieve stress, but long-term structural damage in the brain is not corrected by exercise.
Exercises can only be beneficial if they are performed systematically. It is necessary to repeat the full course daily. Improvement can only be achieved in cases where there is minor vision loss. In case of serious disorders, therapeutic exercises should be combined with medication. Only comprehensive restoration will help restore vision.
Exercises to restore vision after a stroke
- Cover your eyes with your palms, inhale and exhale deeply several times. Gently press with your palms on the upper and lower edges of the eye socket. Start with 3-4 repetitions, increasing the number of approaches.
- Gently press your fingers into the indentations above the eyeballs. Make vibrating movements, sharply release your fingers. Repeat 5 times.
- Gently press on the eyes, sharply releasing your fingers. Repeat 5 times.
- Close your eyes tightly and relax your eyes.
- Squeeze the bridge of the nose near the corners of the eyes. Hold for 5 seconds, then quickly release your fingers. Repeat 5 times.
If the patient cannot perform gymnastics on his own, relatives or hospital staff can help him. Eye exercises are not effective in restoring damaged brain cells, but exercises help relieve eye strain and eliminate redness and burning.
It is recommended to combine exercises with drug therapy and training of other parts of the body that have been damaged (limbs, face, jaws). Only an integrated approach will allow complete rehabilitation after a stroke.
There are no diseases that go away without consequences for the body. Stroke is one of those conditions that extremely negatively affects a person’s quality of life, depriving him of basic functions: vision, speech, movement. A stroke causes an acute circulatory disorder, including in the brain, an organ that is responsible for the functionality of the body. Vision problems occur if the lesion is localized in the area of the vessels that supply blood to the visual center in the brain.
Visual impairment can be a complication of a stroke or an independent disease (ocular stroke). Poor blood circulation in the brain very often affects the visual centers. After a stroke, vision also deteriorates due to infections acquired in intensive care.
Sources used:
- Kvasova M. D. Vision and heredity. - Moscow / St. Petersburg: Dilya, 2002.
- Textbook of eye diseases. Volume I: monograph. / E. Fuchs. - M.: State Publishing House of Medical Literature, 1988.
- D. Hubel. Eye, brain, vision. — ed. A. L. Byzova. - M.: Mir, 1990.
- International Council of Ophthalmology
Occlusion (blockage) of the central retinal artery
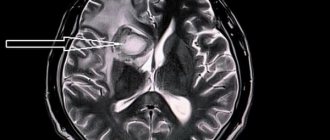
If a blood clot or embolus enters a retinal artery, it may become blocked, stopping blood flow and causing loss of vision. In some cases, the blood clot can quickly dissolve, and vision can be restored.
However, if the blood clot is large enough, vision is not restored. As a rule, the patient does not experience pain. There is usually no pain in this case. If blood supply to the retina is interrupted for more than 1.5 hours (approximately), vision may not be restored, even if the blood clot resolves and blood circulation resumes.
(In Fig. The white arrow shows an arterial thrombus.) This condition indicates a risk of heart attack or stroke.
If the patient immediately contacts an ophthalmologist, the prescribed treatment will help prevent irreversible vision loss .
Signs of memory impairment
A patient who has suffered a stroke usually faces difficulties in self-identification and other difficulties:
- Memories from childhood, adolescence or any other period of life disappear. He may not remember people he has ever encountered, certain significant situations and events.
- Loss of motor skills and loss of coordination. It’s as if the body is returning to childhood: it doesn’t remember how to eat, take care of itself in terms of hygiene, and learns everything all over again.
At the same time, there are situations when the victim remembers everything related to his profession down to the smallest detail. For example, he knows how to drive a car, knows musical notation, remembers how he wrote his dissertation, etc. - but does not have the skills of banal household self-service.
Sometimes amnesia is not immediately noticeable and appears much later in the process of secondary complications after a stroke.
When the disease occurs, the patient’s psyche also suffers: the person does not remember the people who communicate with him. Does not understand the purpose of certain items. Can’t remember professional skills – feels extremely uncomfortable. The victim may become depressed or be in a state of increased anxiety, which negatively affects the rehabilitation process and sometimes leads to psycho-emotional breakdowns.
Central retinal vein occlusion
Venous outflow from the vessels of the retina is carried out by one single vessel - the central retinal vein . If this vein becomes obstructed, various problems may occur, proportional to the degree of obstruction. In the case of such a pathology, the patient notices:
* vision impairment,
* blurred image,
* appearance of floaters
* loss of visual fields.
These changes occur unexpectedly and progress over a period of time (from several hours to several days). As a rule, these changes occur in one eye, rarely in both eyes.
The basis of this pathology is, as a rule, vascular changes, blood clots (as well as with blockage of the arteries).
The most effective treatment for this disease is treatment of concomitant diseases (diabetes, hypertension, atherosclerosis) in the hope that blood flow will be restored.
In about a third of all cases, vision is almost completely restored, in a third it remains at the same level, and in a third there is further deterioration and significant loss of vision.
In the most severe situations, it is necessary to resort to laser treatment to prevent dangerous forms of glaucoma . however, laser treatment will not restore vision.
Stroke. Loss of vision due to strokes
A stroke is a disruption of blood circulation in the brain as a result of blockage of a vessel. If the blockage occurs in the blood vessels supplying the optic lobes of the brain, vision loss may occur. When the affected area is small, a small portion of the visual field is lost (a so-called blind spot ).
There are two visual lobes of the brain - right and left. In the left, a visual image is formed from the right halves of the retinas of both eyes, in the right - from the left halves. Therefore, when one half of the brain is damaged, the corresponding parts of the visual fields are lost in both eyes.
Treatment of strokes . occurring in the vascular system supplying blood to the occipital lobes of the brain, is carried out in the same way as the treatment of any stroke, with the participation of a therapist and a neurologist.
Methods for improving vision after a stroke
After a stroke, artificial tears, Korneregel, Taufon, Normax, Taurine are prescribed. Hydration is extremely important for patients who have been in a coma.
During the rehabilitation period, you need to reconsider your diet. After a stroke, it is recommended to eat more carrots, yellow peppers, pumpkin, egg yolks and fish. Cataract prevention is provided by grapes, blueberries and onions.
After a stroke, it is useful to massage with hot or cold compresses. This helps relax the eyes and improve blood circulation. It is enough to wet one towel in cold water and the other in warm water, and alternate them for 5-10 minutes.
The usual tossing of a ball or ball helps in restoring vision. You need to throw the object back and forth from the affected side. Focusing your gaze on an object will help to establish synchronicity between movements and vision.
Computer programs will help to rehabilitate vision after a stroke. One of these programs shows a black square; at certain intervals, a cluster of one hundred dots flashes on the side of the affected eye. Exercises on the computer take 15-20 minutes a day. The course of treatment is several months.
Comparative exercises allow you to check the extent of visual focus impairment. They make it possible to determine the required degree of rehabilitation therapy. The patient should close his eyes and direct his gaze to the injured side of the body. After determining the correct (according to the patient) direction, the eyes are opened, and the doctor determines the proximity of the gaze from the desired direction.
Compensatory vision therapy stimulates the areas of the brain that support vision. It includes scanning, visual field recognition and prism exercises. The visual field can be adapted by moving images from invisible zones.
Prisms in ophthalmology are used to correct various visual impairments. The type and placement of the prism will be determined by the symptoms. In case of double vision, the prism is placed on a glass lens, which allows you to align the direction of view. Spatial neglect requires the use of a prism on the left side of the visual field so that it reflects objects on different sides.
Restorative vision therapy aims to stimulate nerve connections in the brain. There are different techniques for all types of visual impairments.
Usually, surgical treatment of the organs of vision does not help anything after a stroke, because the problem lies in the brain. Only in some cases does surgery correct double vision by affecting the eye muscles.
Causes of vision loss
Loss of vision (amaurosis) can be a consequence of retinal detachment or ischemia and other eye diseases (for example, glaucoma or uveitis), damage to the optic nerves, or bilateral damage to the visual cortex. Patients with acutely developed visual impairment should be urgently hospitalized. At the same time, the information that the emergency doctor is able to collect about the development of vision loss is important and helps to quickly establish a diagnosis at the hospital stage. In this article we will look at what sudden loss of vision is and the causes of this disease.
Causes of vision loss and blindness
Sudden loss of vision in one eye usually results from damage to the retina and other structures of the eye or the optic nerve. One of its common causes is a transient circulatory disorder in the retina. Typically, patients complain of a veil that suddenly falls in front of the eye and sometimes covers only part of the field of vision. Sometimes sensory disturbances and transient weakness in opposite limbs are simultaneously observed. The duration of the episode ranges from several minutes to several hours.
In 90% of cases, the cause is retinal artery embolism from an ulcerated atherosclerotic plaque in the internal carotid artery, aortic arch, or from the heart (often with valvular disease or atrial fibrillation). Less commonly, the cause of vision loss is a drop in blood pressure in a patient with severe stenosis of the internal carotid artery. Sudden loss of vision in one eye is a harbinger of a stroke and should be a reason for active examination of the patient. The likelihood of developing a stroke can be reduced by constant intake of aspirin (100–300 mg per day) or indirect anticoagulants (for cardiogenic embolism).
Migraine as a cause of vision loss
In young people, retinal migraine may cause transient blindness in one eye. The loss of vision in this case is a migraine aura that precedes an attack of headache or occurs shortly after its onset. However, even with a typical history, it is advisable to exclude pathology of the carotid arteries and heart using a special study. The differential diagnosis is also made with a visual aura in the form of a migrating scintillating scotoma during an attack of classic migraine, but the visual aura usually involves the right and/or left visual fields in both eyes, and not one eye, in addition, it remains visible in the dark and when closing the eyes .
Vision loss due to ischemic neuropathy
Anterior ischemic optic neuropathy is caused by insufficient blood flow through the posterior ciliary artery, which supplies the optic disc. Clinically, it manifests itself as a sudden loss of vision in one eye, not accompanied by pain in the eyeball. The diagnosis of vision loss can be easily confirmed by fundus examination, which reveals swelling and hemorrhage in the area of the optic nerve head.
Most often it develops in patients with long-term arterial hypertension and diabetes mellitus, often in patients with vasculitis or polycythemia. In 5% of cases (especially often in patients over 65 years of age), neuropathy is associated with temporal arteritis and requires immediate corticosteroid therapy to prevent loss of vision in the second eye. The diagnosis of temporal arteritis is facilitated by identifying painful thickening and absence of pulsation of the temporal artery and signs of polymyalgia rheumatica.
Posterior ischemic optic neuropathy is less common. It is usually caused by a combination of severe anemia and hypotension and may cause retrobulbar nerve infarction. Sometimes posterior ischemic neuropathy occurs against the background of massive blood loss during surgery, gastrointestinal bleeding, or trauma. There are no changes in the fundus. In hypertensive crisis, a sudden drop in vision may be a consequence of spasm of the retinal arterioles or ischemic edema of the optic nerve head. An excessively rapid decrease in blood pressure can lead to optic disc infarction.
Causes of vision loss: optic neuritis
Optic neuritis, an inflammatory demyelinating disease, often involves the retrobulbar part of the nerve (retrobulbar neuritis), so pathology cannot be detected during the initial examination of the fundus. Most patients, in addition to acute loss of vision, experience pain in the eyeball, which intensifies with its movement. Vision loss often develops at a young age, can recur, and is often the first manifestation of multiple sclerosis. Intravenous administration of large doses of methylprednisolone (1 g per day for 3 days) accelerates recovery.
Loss of vision due to toxic neuropathy
Sudden blindness in both eyes may be a manifestation of toxic optic neuropathy. Toxic neuropathy may be associated with methyl alcohol, ethylene glycol (antifreeze), or carbon monoxide poisoning. A more gradual development of optic neuropathy with increasing atrophy without a disc swelling phase can be caused by a number of drugs - chloramphenicol (chloramphenicol), amiodarone, streptomycin, isoniazid, penicillamine, digoxin, ciprofloxacin, as well as lead, arsenic or thallium poisoning.
Loss of vision due to increased intracranial pressure
Blindness can also be a consequence of intracranial hypertension and the development of congestive optic discs (with benign intracranial hypertension or brain tumors). It is often preceded by short-term episodes of blurred vision in one or both eyes, occurring when changing body position and lasting several seconds or minutes. In case of persistent loss of vision, administration of methylprednisolone (250–500 mg intravenously) and urgent consultation with an ophthalmologist and neurosurgeon are necessary.
Infarction of the occipital lobes of the brain as a cause of vision loss
Acute blindness in both eyes can also be a consequence of bilateral infarction of the occipital lobes (cortical blindness) and occur as a result of blockage of the basilar artery (usually as a result of embolism) or prolonged systemic arterial hypotension. The source of embolism is usually atherosclerotic plaques in the vertebral arteries. Vision loss is often preceded by episodes of vertebrobasilar insufficiency with unilateral or bilateral paresthesias or paresis, ataxia, dysarthria, hemianopsia, dizziness, double vision. Unlike bilateral blindness caused by damage to the optic nerves, with cortical blindness, pupillary reactions remain intact. Some patients with cortical blindness develop anosognosia: such a patient denies the presence of blindness, claiming that the room is dark or he simply forgot his glasses.
Acute loss of vision as a symptom of hysteria
Acute loss of vision may be psychogenic in nature and be one of the manifestations of hysteria. Typically, such patients (usually young women) claim that everything around them is immersed in darkness (patients with organic cortical blindness often find it difficult to describe their visual sensations). The history often reveals other hysterical symptoms (lump in the throat, pseudoparesis, hysterical seizures, mutism, hysterical gait disturbances). Pupillary reactions are normal, there are no stem symptoms. Unlike those around them, whose obligatory presence and extreme concern can serve as an additional diagnostic criterion, patients are often not alarmed, but rather calm, and sometimes even smile mysteriously (“beautiful indifference”).
© Author: therapist Elena Dmitrenko
Stroke
Stroke, stroke treatment, stroke prevention, hemorrhagic stroke, ischemic stroke, International Center for Neurosurgery.
Definition
A stroke occurs when blood flow to part of the brain is stopped or significantly reduced. As a result, the brain does not receive enough oxygen and the nutrients it needs. Within minutes, brain cells begin to die.
Stroke is a medical emergency because prompt medical attention can minimize brain damage and possible complications.
The good news is that stroke can be treated and prevented. The key to preventing stroke is strict control of the main risk factors for stroke. These include: high blood pressure, smoking and high cholesterol.
Symptoms of a stroke
Look for the following symptoms if you think you or someone you know may be having a stroke. Also remember when these symptoms started, as how long they last may have an impact on treatment options.
Main symptoms:
- Walking disorder.
- Impaired speech and understanding of words.
- Paralysis or numbness on one side of the face or entire body.
You may feel sudden numbness, weakness, or paralysis on one side of your body. Try raising both arms above your head. If one arm begins to fall, you may have a stroke. Likewise, one side of the mouth may fall down when trying to smile. - Visual impairment on one or both sides.
- Headache.
A sudden, severe, “out of the blue” headache that may be accompanied by vomiting, dizziness, or confusion.
When should you see a doctor immediately?
If you notice any of the above signs, even if they change or disappear, call an ambulance immediately. In the event of a stroke, every minute counts. Don't wait, even if your stroke symptoms begin to subside. The later treatment for a stroke is started, the greater the likelihood of brain damage and disability. To ensure maximum effectiveness of stroke treatment, it is necessary to transport the patient to the hospital within 60 minutes of the first symptoms.
What can you do while waiting for an ambulance?
Causes of stroke
When a stroke occurs, blood flow through the brain is disrupted and brain tissue is damaged. There are two main types of stroke. The most common type is ischemic stroke, which results from blockage of blood flow through an artery. Another type, hemorrhagic stroke, occurs as a result of bleeding from a blood vessel in the brain. A transient ischemic attack (TIA)—sometimes called a mini-stroke—occurs when blood flow through the brain is temporarily interrupted.
Ischemic stroke
Almost 90 percent of strokes are ischemic strokes. They occur when the arteries in your brain become narrowed or blocked, resulting in a sharp reduction in blood flow to the brain (ischemia). The lack of blood flow deprives brain cells of oxygen and nutrients, and the cells can begin to die within minutes. The most common types of ischemic stroke are:
- Thrombotic stroke.
This type of stroke occurs when a blood clot (thrombus) forms in one of the arteries supplying blood to the brain. The clot usually forms in areas affected by atherosclerosis, a disease in which the arteries are clogged with fatty deposits (plaques). The process can occur in one of the two carotid arteries that run through the neck and carry blood to the brain, as well as in other arteries in the neck or brain. - Embolic stroke.
An embolic stroke occurs when a blood clot forms in blood vessels outside the brain—usually in your heart—and travels through the bloodstream into narrower arteries in the brain. This type of blood clot is called an embolus. The cause is an irregular heartbeat (atrial fibrillation). This abnormal heart rhythm can cause blood clots to form in the chambers of the heart, from where they travel to other parts of the body.
Hemorrhagic stroke
Hemorrhage is the medical term for bleeding. A hemorrhagic stroke occurs when a blood vessel in the brain leaks or ruptures. Brain hemorrhages can result from a number of causes affecting the blood vessels, including uncontrolled high blood pressure (hypertension) and weak spots in the walls of blood vessels (aneurysms). A less common cause of hemorrhage is the rupture of an arteriovenous malformation (AVM), which is a tangle of thin-walled blood vessels and is a congenital pathology. There are two types of hemorrhagic stroke:
- Intracerebral hemorrhage, with
this type of stroke, blood leaks from a blood vessel in the brain into surrounding tissue, damaging cells. Brain cells are also damaged due to impaired blood supply. High blood pressure is a common cause of this type of hemorrhagic stroke. With long-term hypertension, high blood pressure can cause small arteries inside the brain to crack and collapse, leading to hemorrhage. - Subarachnoid hemorrhage, in
this type of stroke, bleeding develops in the arteries near the surface of the brain, and the hemorrhage occurs in the space between the surface of the brain and the skull. Bleeding is often signaled by a sudden, severe headache. This type of stroke is usually associated with a ruptured aneurysm, which may be congenital or develop with age. After a hemorrhage, the brain's blood vessels may widen or narrow randomly (vasospasm), causing damage to brain cells, further restricting blood flow to parts of the brain.
Transient ischemic attack (TIA)
A transient ischemic attack (TIA)—sometimes called a mini-stroke—is a brief episode of symptoms similar to those of a stroke. A transient ischemic attack is caused by a temporary decrease in blood flow to part of the brain. Most TIAs last less than five minutes.
As with an ischemic stroke, in a TIA, a clot disrupts blood flow to part of the brain. But unlike a stroke, which is characterized by a longer-term lack of blood supply and often permanent tissue damage, a TIA does not cause significant damage because the blockage of the vessel is temporary.
Seek emergency medical help even if your symptoms begin to subside. If you have had a TIA, it means that the blood vessels leading to the brain are partially blocked or narrowed and you are at high risk of having a severe stroke. It is difficult to differentiate between a stroke and a TIA based solely on the presence of symptoms of the disease. Some symptoms go away even in the presence of a stroke with brain damage.
Risk factors
Many factors can increase your risk of stroke. Some of these factors also increase your risk of developing heart disease. Risk factors for stroke include:
- Have a personal or family history of stroke, heart attack, or TIA.
- Age 55 years and older.
- High blood pressure. The risk of stroke begins to increase as blood pressure rises above 115/75 mmHg.
- High cholesterol - total cholesterol levels above 5.2 mmol/L.
- Smoking cigarettes or passive smoking.
- Diabetes.
- Overweight (body mass index of 25 to 29) or obese (body mass index of 30 or higher).
- Lack of physical activity.
- Cardiovascular disease, including heart failure, heart disease, heart infection, or abnormal heart rhythm.
- Using birth control pills or hormone therapy that includes estrogen.
- Alcohol consumption.
- Drug use.
Because the risk of stroke increases with age and women tend to live longer than men, women are more likely to suffer and die from stroke.
Complications
A stroke can cause temporary or permanent disability, depending on how long the brain suffers from lack of blood flow and what part of the brain is affected. Complications may include:
- Paralysis or loss of muscle movement.
Sometimes a lack of blood flow to the brain can cause paralysis on one side of the body or loss of control of certain muscles, such as on one side of a person's face. Physical therapy may lead to improved muscle movement or decreased paralysis. - Speech or swallowing problems.
A stroke can cause loss of muscle control in the throat and mouth, making it difficult to speak, swallow, and eat in general. For a person, having aphasia can be a severe condition in which they experience difficulty expressing thoughts through language. Sessions with a speech therapist and psychotherapist can improve this condition. - Memory loss or difficulty understanding.
Typically, people who have had a stroke have some memory impairment. Others may have difficulty making decisions, reasoning, and understanding concepts. Improvement may be due to rehabilitation therapy. - Pain.
Some people who have had a stroke may complain of pain, numbness, or other strange sensations in parts of the body affected by the stroke. For example, if a stroke caused loss of sensation in your left arm, you may feel a tingling sensation in that arm. You may also become sensitive to temperature changes. This is called central stroke pain or central pain syndrome. The complication usually develops several weeks after the stroke and may subside over time. Sometimes requires treatment. - Changes in behavior and self-care.
People who have had a stroke may become more withdrawn and less socially active. They may lose the ability to care for themselves and often need outside care and daily care.
As with any traumatic brain injury, the success of treating these complications will vary from person to person.
Examination and diagnosis
To determine the most appropriate treatment, the emergency team must find out what type of stroke the patient has and what parts of the brain are affected. Other possible causes of symptoms, such as a brain tumor or drug reaction, must be ruled out. The doctor may use the following tests:
- Physical examination.
The doctor will ask you or a family member about your symptoms, when they started, medications you take, any head injuries, and your personal and family medical history. He will check your blood pressure, listen to your heart and sounds (murmurs) over your carotid arteries, which may indicate atherosclerosis. The doctor may also use an ophthalmoscope to check for signs of tiny cholesterol crystals or blood clots in the blood vessels at the back of the eye. - Blood tests.
Blood tests provide important information about how quickly your blood clots, what your blood sugar levels are, whether you have an infection, and what your blood chemistry levels are, which is important for deciding how to treat your stroke. - Computed tomography (CT).
An image of the brain that plays a key role in determining the presence of a stroke and its type. A CT angiography scan is a specialized test in which dye is injected into a vein and X-rays create a 3-D image of the blood vessels in the neck and brain. Doctors use this test for aneurysms and arteriovenous malformations to assess the degree of narrowing of the arteries. CT without angiography can provide an image of the brain and show hemorrhage, but provides less information about the blood vessels. - Magnetic resonance imaging (MRI).
In this type of examination, a strong magnetic field and radio waves create a 3-D image of the brain. MRI can reveal damage to brain tissue during an ischemic stroke. Magnetic resonance angiography (MRA) uses magnetic fields, radio waves and a dye injected into a vein to evaluate the arteries of the neck and brain. - Ultrasound examination of the carotid arteries.
This procedure may show narrowing of the arteries or the presence of blood clots in the carotid artery. - Arteriography.
- Echocardiography.
Ultrasound technology creates an image of the heart and allows the doctor to identify blood clots in the cavities of the heart.
Stroke treatment
Emergency treatment for stroke depends on its type - ischemic or hemorrhagic stroke.
Ischemic stroke
To treat an ischemic stroke, doctors must quickly restore blood flow to the brain.
Treatment with drugs.
Treatment with blood thinners should begin within 4.5 hours - the sooner the better. This improves the chances of survival and reduces stroke complications. For this use:
- Aspirin.
Aspirin is the most proven effective drug for the immediate treatment of ischemic stroke, reducing the likelihood of a recurrent stroke. The dose of the drug may vary.
Other blood thinners such as warfarin, heparin and clopidogrel may also be used, but not for emergency treatment.
- Administration of tissue plasminogen activator (tPA).
Some patients with ischemic stroke will benefit from early administration (within 4.5 hours of onset) of tissue plasminogen activator (tPA), which dissolves the clot and restores blood flow in the blocked artery. The administration of this drug is contraindicated for hemorrhagic stroke.
During treatment
ischemic strokes often require procedures that must be performed as quickly as possible. These are the following procedures:
- Using tissue plasminogen activator (tPA) delivered directly to the brain.
Doctors may use catheters to inject this drug into the brain. - Mechanical clot removal.
Doctors also use a catheter to maneuver into the brain to mechanically remove the clot.
Other procedures.
To reduce the risk of another stroke or TIA, your doctor may recommend procedures to open arteries narrowed by plaque. These may include:
- Endarterectomy of the carotid arteries
. In this procedure, the surgeon removes plaque blocking the carotid arteries in the neck. The blocked artery is opened and the plaque is removed. The procedure may reduce the risk of ischemic stroke. However, carotid endarterectomy itself can also cause a stroke or heart attack by promoting blood clot formation. To reduce the risk of stroke, special filters are used at strategic points in the blood flow. - Angioplasty and stenting.
Angioplasty is another method of widening the arteries leading to the brain, usually the carotid arteries. This procedure uses a catheter balloon that inflates to compress the plaque and dilate the arteries. More often, stenting is used with the placement of special metal tubes (stents) in the narrowed areas of the arteries, which remain in the artery, preventing its narrowing. Placing a stent in an artery in the brain (intracranial stenting) is similar to stenting in the carotid arteries.
Hemorrhagic stroke
Acute treatment of hemorrhagic stroke focuses on controlling bleeding and reducing pressure in the brain.
Emergency measures.
If you are taking warfarin or antiplatelet drugs to prevent clots, such as clopidogrel (Plavix), you may receive blood transfusions or medications to counteract the effects of warfarin or clopidogrel. You may need medications to lower your blood pressure. The use of aspirin and tissue plasminogen activator is prohibited because it may worsen bleeding.
Treatment for hemorrhage usually involves bed rest. If the bleeding area is large, surgery may be needed to remove the blood and relieve pressure on the brain.
Surgical reconstruction of blood vessels.
Surgery may be used to repair certain blood vessel abnormalities associated with hemorrhagic stroke. A doctor may recommend one of these procedures after a stroke or if there is a high risk of spontaneous rupture of an aneurysm or arteriovenous malformation (AVM):
- Aneurysm clipping.
Tiny clamps are placed at the base of the aneurysm, sealing it off from blood flow in the artery. This may keep the aneurysm from rupturing or prevent the aneurysm from bleeding again. The clip remains in place permanently. - Embolization of aneurysm.
This procedure is an alternative to aneurysm clipping. Surgeons use a catheter to maneuver inside the aneurysm. - Surgical removal of AVM.
Surgical removal of small AVMs in accessible parts of the brain can eliminate the risk of rupture and reduce the overall risk of hemorrhagic stroke. This does not apply to AVMs that are too large or deep inside the brain.
Recovery and rehabilitation
After initial measures, stroke treatment focuses on helping the patient regain strength, function, and return to independent living. The effect depends on the area of the brain damaged and the extent of the damage. Damage to the right side of the brain can affect movement and sensation in the left side of the body. Damage to the left side of the brain can affect movements on the right side and can cause speech disorders. In addition, stroke patients may have problems breathing, swallowing, balance, and hearing. Possible loss of vision, impaired bowel and bladder function.
People who have suffered a stroke need treatment using rehabilitation programs. Your doctor will help you choose a program based on your age, general health, and degree of disability. Lifestyle, interests and priorities, and the presence of other family members are also taken into account.
A rehabilitation program may begin before hospital discharge. It can continue in specialized rehabilitation departments, sanatoriums, and at home. The extent of recovery from a stroke varies from person to person.
Stroke Prevention
The key to preventing stroke is identifying risk factors, following your doctor's recommendations, and maintaining a healthy lifestyle. If you've had a stroke or TIA, these steps will also help prevent another. A healthy lifestyle includes:
- Controlling high blood pressure (hypertension).
If you have had a stroke, lowering your blood pressure will help prevent another transient ischemic attack or stroke. Managing stress, maintaining a healthy weight, and limiting salt and alcohol intake will help keep your blood pressure under control. Adding more potassium to your diet may also help. In addition to recommendations for lifestyle changes, your doctor may prescribe medications to treat high blood pressure, such as diuretics, calcium antagonists, angiotensin-converting enzyme (ACE) inhibitors, and angiotensin receptor blockers. - Reduce cholesterol and saturated fat in your diet.
Diet adjustments and statin use are necessary to lower cholesterol levels. - To give up smoking.
Smoking increases the risk of stroke for smokers and nonsmokers exposed to secondhand smoke. Quitting smoking reduces risk several years after quitting. - Diabetes control.
Diabetes can be managed through diet, exercise, weight control and treatment. - Healthy weight support.
Excess weight contributes to other risk factors for stroke, such as high blood pressure, heart disease and diabetes. Losing weight can lower blood pressure and reduce blood cholesterol levels. - Maintain a diet rich in fruits and vegetables.
A diet containing five or more servings of fruits or vegetables may reduce the risk of stroke. - Physical activity.
Aerobic exercise reduces the risk of stroke in different ways. Exercise can lower blood pressure, increase high-density lipoprotein (“good” cholesterol) levels, and improve overall blood vessel and heart health. It also helps you lose weight, control diabetes and reduce stress levels. 30 minutes of activity - walking, running, swimming or cycling - gives good results.
Restoring vision after a stroke - basic principles
In order to be able to restore vision in the future, if you have a stroke, you need to urgently consult a doctor and get qualified help. An ophthalmologist treats visual impairment after a stroke. All stages of recovery must be approved by a doctor. It is very important to analyze the results and adjust the rehabilitation scheme in a timely manner.
Principles of vision restoration after stroke
- moisturizing the eyes with drops and gels;
- restoration of affected visual functions with the help of medications;
- regular and correct exercise;
- diet with vitamins, especially vitamin A;
- taking nutritional supplements.
After a stroke that causes vision loss, you need to seriously engage in general rehabilitation and restoration of visual function. Without making an effort, the patient risks remaining blind for life, because medications are not able to restore vision completely. Rehabilitation may include exercises, medications, and even surgery.
Ways to improve vision after a stroke
- Gymnastics. Special exercises help stop the progression of presbyopia at the initial stage of its development. Before starting therapy, the visual organs should be prepared; it is recommended to hold your face over warm water and splash it into your eyes. There are a large number of techniques, so the choice is up to the ophthalmologist.
- Medicines. Medications for visual impairment after a stroke are prescribed when gymnastics is not effective enough. There are a large number of remedies, so the choice should also be entrusted to a doctor. It will take into account the characteristics of the disorders, concomitant pathologies and contraindications.
- Surgery. The operation is prescribed as a last resort. Patients usually require lens replacement after a stroke. In its place, a special lens is implanted, which performs all the functions of a natural lens and is combined with the structures of the eye. Surgery to remove the lens is one hundred percent prevention of cataracts.
It must be remembered that the problem of vision after a stroke is very individual. A recovery program is developed for each individual patient, taking into account the degree of damage and consequences. However, absolutely everyone is recommended to moisturize the mucous membrane with the help of drops and gels.