Aspirin, or acetylsalicylic acid, is a medicinal substance belonging to the group of so-called non-steroidal anti-inflammatory drugs.
It includes drugs familiar to many, such as ibuprofen (Nurofen, Faspik, Advil), nimesulide (Nimesil, Nise), meloxicam (Movalis, Artrosan) and some others, but only aspirin has a unique effect on platelets.
Aspirin does not thin the blood.
In fact, it is a myth that aspirin thins the blood. How “thin” a person’s blood is depends on the content of hemoglobin and red blood cells in it (a person with anemia has more “watery” blood), as well as on the amount of fluid consumed. Aspirin reduces the ability of blood to clot, that is, to form blood clots, and does not affect its “thickness.”
Contraindications
The drug has relative and absolute contraindications. You should refuse to take it if you have allergic reactions to the constituent components, as well as in conditions where bleeding may begin.
Relative contraindications include:
- bronchial asthma;
- problems with kidney function;
- diabetes;
- age up to 12 years;
- chronic gastrointestinal diseases;
- period of bearing a child;
- breastfeeding period.
If there are relative contraindications, then taking the drug is possible only after examination by a doctor and his approval.
How does aspirin work?
It blocks the action of the enzyme cyclooxygenase in the body, thus reducing the synthesis of special substances - prostaglandins.
Prostaglandins are involved in the processes of inflammation, in the regulation of vascular tone, muscle contractions, protect the wall of the stomach and intestines from chemical damage and promote the formation of blood clots when the walls of blood vessels are damaged.
Platelets are pieces of cells that constantly float through the bloodstream. In some situations, they can “activate” and stick together, forming a blood clot. As a rule, this occurs when a vessel is damaged - an injury or a cut, and helps the body avoid large blood losses.
Cardiovascular diseases are currently the leading cause of death in the world and in Russia, and first of all we are talking about coronary heart disease and myocardial infarction, as well as ischemic stroke.
Cardiovascular diseases are currently the leading cause of death in the world.
Most heart attacks and strokes occur when blood flow to an area of the heart or brain is blocked by a blood clot.
And it all begins gradually, with the development of atherosclerotic vascular disease. This is the name of the process in which a gradual accumulation of cholesterol, cellular breakdown products and calcium occurs in the inner layer of the vascular wall - an atherosclerotic plaque is formed. Atherosclerosis usually affects large and medium-sized arteries, and the plaques themselves often grow to such a size that they begin to significantly impede blood flow.
But the real problems begin when the plaque becomes brittle and ruptures. The body reacts to a ruptured plaque in the same way as to a ruptured vessel, saving itself from major blood loss - it tries to “patch” the damage by covering the area with a blood clot, and platelets are the first to arrive at the site of damage. A ruptured plaque “misleads the platelets” and becomes the site of the formation of a blood clot, partially or completely blocking the blood flow.
If a blood clot blocks a vessel supplying blood to the heart, myocardial infarction develops; if it supplies blood to the brain, an ischemic stroke occurs.
In recent decades aspirin has firmly entered our lives as a drug that helps maintain heart health, and has practically become a “vitamin for the myocardium.” Anyone can go to the pharmacy and buy aspirin without a prescription.
Daily use of low-dose aspirin (usually 50-100 mg per day) has been considered an effective way to reduce the risk of myocardial infarction, ischemic (that is, associated with decreased cerebral blood flow) stroke, and other problems associated with impaired vascular blood flow.
However, in 2017-2019, several large medical studies were conducted that changed the point of view of doctors on this drug.
The data obtained concerned patients who did not have coronary heart and vascular disease, heart attacks or strokes in the past, but who took the drug to prevent them in the future.
The first found no benefit from aspirin in patients at low risk of developing cardiovascular disease.
The second unexpectedly showed an increase in overall mortality in older people without cardiac disease who took aspirin as prophylaxis.
The third found a high risk of bleeding that outweighed the benefit of aspirin in most patients at moderate risk of developing cardiovascular disease, and identified a group of people who benefit from prophylactic aspirin.
Finally, to find out how many people take preventative aspirin, a survey was conducted in the United States of more than 14,000 men and women over 40 years of age. It turned out that about a quarter of healthy people take aspirin for preventive purposes, and a quarter of these people decided to take aspirin treatment on their own, without consulting a doctor. Moreover, half of respondents aged 70 years and older, and without cardiovascular disease, took aspirin daily.
A quarter of healthy people take aspirin for preventive purposes.
Unfortunately, taking any medicine, regardless of its study and breadth of use, is simultaneously associated with both health benefits and the risk of complications.
Aspirin, while reducing the formation of blood clots in the body, has serious side effects, which are the “other side of the coin” - gastrointestinal bleeding, as well as severe intracerebral, intraocular and intraarticular hemorrhages.
There must be very good reasons for recommendations for its preventive use!
So, when should a cardiologist recommend that a patient take low-dose aspirin every day?
- Firstly, this is necessary for those patients who have already experienced one or more strokes or myocardial infarction. The risk of developing a recurrence in such people is almost 8 times higher compared to those who have never been sick. This kind of prevention is called secondary (we try to prevent the second and subsequent cardiovascular accidents)
- Prophylactic treatment is also necessary for those who have not had a heart attack, but who previously had a stent installed in the coronary artery, or for those who have undergone coronary artery bypass surgery. The doctor will also prescribe aspirin to someone who has been diagnosed with angina pectoris - pain in the chest during physical (less often emotional) stress associated with atherosclerotic narrowing in the coronary vessels
- Aspirin is infrequently prescribed to patients with atrial fibrillation, heart valve disease or prosthetic valves - usually when more effective drugs cannot be prescribed
- Aspirin is used to treat atherosclerotic changes in the arteries of the legs - with these problems, patients experience severe pain in the calf muscles when walking, this is called “intermittent claudication”
- And finally, the most difficult situation is prescribing aspirin to a patient who does not yet have any cardiovascular diseases in order to prevent their occurrence. The so-called “primary prevention” of the disease
Please remember that for people over 70 years of age who do not have cardiovascular disease, taking preventive aspirin is generally not recommended, it will not provide any benefit, and the risk of severe bleeding is very high.
For people over 70 years of age who do not have cardiovascular disease, preventive aspirin is generally not recommended.
Aspirin prophylaxis currently recommended for people 50–69 years of age with a low risk of bleeding and a greater than 10% risk of heart attack or stroke over the next 10 years of life. Risk factors include male gender, diabetes, frequent high blood pressure, smoking and high cholesterol levels in blood tests.
Adverse reactions and overdose
While taking the medicine, undesirable reactions may occur:
- increased susceptibility to the constituent components, manifested by skin rash;
- pain in the abdomen.
With regular and frequent use, in rare cases, bleeding from the stomach may begin, which is manifested by the following symptoms:
- anemia;
- malaise;
- unbearable pain in the stomach.
If such signs appear, you should immediately stop taking it and inform a specialist.
An overdose of the drug is manifested by the following symptoms: nausea, vomiting, hearing problems, confused thinking.
Rules for taking medications
The symptoms of a hangover hinder a person’s functionality and put him in a state of weakness and malaise. The benefit of the drug will be optimal if it is taken correctly in accordance with the parameters established by the attending physician or with the specified recommendations in the instructions.
- It is unacceptable to swallow the tablet without liquid.
- Pills or effervescent powder must be diluted with a certain amount of water.
- It is strictly forbidden to take the tablet with alcohol, beer, tea or juice.
- You should not take the pill right before going to bed.
- It is good to take the powder in the morning, as this will determine the condition of the body for the whole day without causing harm.
The effect of the drug on the body has a different period. According to the indicated properties of aspirin, it begins to act within 10-20 minutes. If the effect does not occur, do not quickly swallow an additional tablet to improve the result. The recommended waiting time for the drug to act is indicated in the permissible probability and the approximate relationship between the properties of the drug and the body. Therefore, these dates are not reliable. It all depends on the person, the amount of alcohol and many other factors that slow down the body’s recovery process.
Special Recommendations
Aspirin cardio and chronic diseases
Particular caution should be exercised when taking aspirin for persons suffering from diseases of the respiratory system. The fact is that taking aspirin causes a narrowing of the bronchi, which can cause so-called aspirin asthma, or provoke asthma, which is in remission.
Aspirin cardio and childhood
When taken in its pure form in children, due to their young age, the concentration of glucose in the plasma can sharply decrease, in parallel with this, the level of ketone bodies in the blood increases, plasma acidification occurs, and fatty acids accumulate in the liver. These metabolic disturbances lead to swelling of tissues and organs.
Children become more than just lethargic. Aggravating symptoms such as cramps, diarrhea, rapid breathing and palpitations may occur. Up to loss of consciousness and severe muscle hypotension. Such conditions in children can be life-threatening, so the drug is contraindicated for them.
Aspirin cardio and alcohol
The combined use of alcohol and aspirin is not recommended. Alcohol and alcohol-containing products are known for their vasodilating properties. But in combination with aspirin, the effect can be most unexpected. The risks of bleeding increase, including in diseases of the gastrointestinal tract, exacerbation of liver diseases or the occurrence of any acute symptoms associated with this organ.
Aspirin cardio and pregnancy
The active substance freely and easily penetrates the placental barrier, which can lead to negative consequences for the fetus.
When used in the first trimester, it leads to the development of a “cleft palate” (cleft palate); in the third trimester, it causes inhibition of labor, premature closure of the ductus arteriosus in the fetus, disruption of the functioning of the pulmonary vessels and hypertension in the pulmonary circulation.
Acetylsalicylic acid is also excreted in breast milk, which increases the risk of bleeding in the baby due to impaired platelet function. Therefore, the advisability of using the drug during pregnancy and lactation should be justified by the specialist making the decision on the prescription.
Causes
Some people who suffer from migraines can clearly identify the triggers or factors that cause their headaches, but many patients cannot. Potential migraine triggers include:
- Allergies and allergic reactions
- Bright lights, loud noise, certain odors or perfumes
- Physical or emotional stress
- Changes in sleep patterns or irregular sleep
- Smoking or exposure to smoke
- Skipping meals or fasting
- Alcohol
- Menstrual cycle fluctuations, birth control pills, hormone fluctuations during the onset of menopause
- Foods containing tyramine (red wine, aged cheese, smoked fish, chicken liver, figs, and some beans), MSG, or foods with nitrates (such as bacon, sausages, and salami)
- Other foods such as chocolate, nuts, peanut butter, avocados, bananas, citrus fruits, onions, dairy products and fermented or pickled foods.
Triggers do not always cause migraines, and avoiding triggers does not always prevent migraine attacks.
Properties of acetylsalicylic acid
Crystalline white powder with a faint sour taste, which is pressed into tablets, or simply diluted with warm water. has many useful properties:
- Antipyretic. By suppressing the synthesis of prostaglandins in the thermoregulation center, blood vessels dilate and sweating increases. The decrease in body temperature occurs quite quickly, within 30-40 minutes. The effect lasts for several hours.
- Painkiller. Aspirin affects pain sensitivity centers and has a peripheral anti-inflammatory effect.
- Antithrombotic. Taking acetylsalicylic acid reduces the content of thromboxane A and slows down the adhesion of blood platelets. Increases the fibrinolytic properties of blood plasma, which promotes the resorption of blood clots and reduces the concentration of blood coagulation factors. vitamin K dependent.
- Anti-inflammatory. By reducing swelling and capillary permeability, hyaluronidase activity and suppressing ATP synthesis, the energy supply to the inflammatory process is limited. In acute inflammatory processes, taking aspirin allows doctors to slow down the expansion of the affected area and take emergency measures.
From hot to cool
A comfortable temperature is considered to be 18–24 degrees outdoors or indoors. But these numbers are approximate. The temperature to which a person is accustomed is comfortable. A resident of Siberia feels best at 23-24°C and does not tolerate 40-degree heat well. If a person lives in the south, then in a cool climate it will not be healthy for him either. At the same time, the main influence on the body is not the air temperature itself, but a complex of weather conditions: in addition to temperature, it is humidity, atmospheric pressure, magnetic field, wind. So, in a dry climate you can feel great at +32-34°C. And in the humid weather and +27 for many it is a test.
Today there are air conditioners everywhere, and they are used incorrectly. There is an unshakable rule: the air conditioner temperature should be a maximum of 5–7° less than outside. Let’s say, if it’s +34 outside, then the air conditioner should be set not at +18, but at +27. This will be enough to feel cool without getting a cold or sciatica.
Treatment of migraine: modern approaches
The disease first makes itself felt usually between the ages of 10 and 20 years. From 30 to 45 years, the frequency of attacks reaches a maximum, and after 55-60 they usually disappear. But sometimes symptoms persist even after 50 years [5-7]. There are two main types of the disease: migraine with aura and without aura. It is important to note that the course of the attack and the nature of the aura are individual for each patient. Typically, the migraine scenario repeats itself, and patients can accurately determine and differentiate the onset of an attack [8].
There are three main approaches to migraine treatment used today:
- normalization of sleep patterns, reducing the influence of stressful situations (auto-training, sessions with a psychotherapist, etc.), individually selected diet, increasing rest periods (many patients with migraine have not had a full vacation for several years);
- preventive treatment;
- relief of attacks: reduction of intensity, duration of pain, accompanying symptoms and restoration of the patient’s general condition.
For a long time, “cocktails” of analgesics or NSAIDs were used to relieve a migraine attack. The emergence of new drugs - triptans - has made it possible to open a new page of effective migraine therapy [9]. Today, triptans or 5HT1 serotonin receptor agonists (sumatriptan, zolmitriptan, eletriptan) are the “gold standard”, that is, the most effective remedy that can significantly relieve migraine pain [10].
Relpax® is an original drug from the group of triptans. The active substance is eletriptan [11]. According to the results of a clinical study in which 1334 outpatients with migraine participated, relief and pain relief was observed within 30 minutes of taking Relpax®, and the drug was also well tolerated [12].
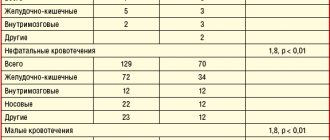
Relpax® demonstrated superiority over sumatriptan. When comparing the effectiveness 2 hours after taking Relpax® and sumatriptan, it was revealed [13-18]: ✔ The reduction in headache intensity after taking the first dose of the drug was statistically significantly greater in the group of patients receiving therapy with eletriptan (Relpax®) than in the treatment group sumatriptan (Fig. 1):
✔ The number of patients whose headaches were completely relieved after taking the first dose of the drug was significantly greater in the group receiving eletriptan therapy than in the sumatriptan treatment group (Fig. 2):
✔ Relpax® (eletriptan) at a dose of 40 mg has better tolerability compared to sumatriptan at a dose of 100 mg (Fig. 3):
The main advantages of Relpax®:
- superiority in effectiveness over other triptans [13-18];
- good tolerability [13-17].
When prescribing Relpax®, one must adhere to three basic principles [11]:
- the drug should be taken as early as possible from the onset of a migraine attack;
- the repeat dose should be taken no earlier than 2 hours after taking the previous one;
- In 24 hours the maximum dose should not exceed 160 mg.
In general, Relpax® is well tolerated. Typically, side effects are transient, mild or moderate, and go away on their own without additional treatment. The main side effects recorded during treatment with Relpax® are typical for the entire class of 5-HT1 receptor agonists [11].
Literature
- Golovacheva V.A., Parfenov V.A. Triptans in the treatment of migraine // MS. 2015. No. 10.
- Koreshkina Marina Igorevna Modern aspects of diagnosis and treatment of migraine // Neurology, neuropsychiatry, psychosomatics. 2013. No. 2.
- Morozova Olga Grigorievna Migraine: new international criteria for diagnosis and principles of therapy based on evidence-based medicine and our own clinical experience // International. neurol. magazine; MNZH. 2021. No. 3
- Filatova E.G. Osipova V.V., Tabeeva G.R. and others. Diagnosis and treatment of migraine: recommendations of Russian experts. Neurology, neuropsychiatry, psychosomatics. 2020;12(4):4–14.
- Maksyukova E.V., Osipova V.V. Migraine in patients of the older age group: clinical and psychological analysis. Russian Journal of Pain. 2011;2:33.
- Sanoeva M.Zh., Saidvaliev F.S., Gulova M.A. Modern view on the problem of migraine (review article) // Bulletin SMUS74. 2021. No. 3 (14).
- Snopkova E.V., Sergeev A.V., Osipova V.V. Comparative clinical and psychological analysis of migraine in young and older patients. Neurological Journal. 2012;17(6):32-37.
- V.V. Osipova. Migraine: clinical picture, diagnosis and treatment approaches. "PHARMATEKA" No. 20 - 2008
- Koreshkina M. I. “Migraine in primary practice. Diagnostics and treatment", Information portal "Pain"
- Ekusheva Evgenia Viktorovna, Filatova Elena Glebovna Migraine in the clinical practice of a neurologist: a thorny path to rational treatment of patients // Consilium Medicum. 2021. No. 2.; 128-135
- Instructions for medical use of the drug Relpax®
- Sheftell F, Ryan R, Pitman V; Eletriptan Steering Committee. Efficacy, safety, and tolerability of oral eletriptan for the treatment of acute migraine: a multicenter, double-blind, placebocontrolled study conducted in the United States. Headache. 2003;43:202-213.
- Mathew NT, Schoenen J, Winner P, Muirhead N, Sikes CR. Comparative efficacy of eletriptan 40 mg versus sumatriptan 100 mg. Headache. 2003;43:214-222.
- Diener HC, Ryan R, Sun W, Hettiarachchi J. The 40-mg dose of eletriptan: comparative efficacy and tolerability versus sumatriptan 100 mg. Eur J Neurol. 2004;11:125-134.
- Sandrini G, Färkkilä M, Burgess G, Forster E, Haughie S; Eletriptan Steering Committee. Eletriptan vs sumatriptan: a double-blind, placebo-controlled, multiple migraine attack study. Neurology. 2002;59:1210-1217.
- Mandema JW, Cox E, Alderman J. Therapeutic benefit of eletriptan compared to sumatriptan for the acute relief of migraine pain—results of a model-based meta-analysis that accounts for encapsulation. Cephalalgia. 2005;25:715-725.
- Almas M, Tepper SJ, Landy S, Schweizer E, Ramos R. Consistency of eletriptan in treating migraine: results of a randomized, within-patient multiple-dose study. Cephalagia. 2014;34:126-135.
- Landy SH, Tepper SJ, Schweizer E, Almas M, Ramos E. Outcome for headache and pain-free nonresponders to treatment of the first attack: a pooled post-hoc analysis of four randomized trials of eletriptan 40 mg. Cephalalgia. 2014;34:376-381.