Any woman thinks about procreation. Not everyone is given the opportunity to have children. Some diseases overshadow the period of waiting for a baby or are a contraindication for pregnancy.
For example, with diabetes mellitus, there are some peculiarities in the course of the process, and difficulties arise with conceiving a child. The disease is divided into two types: type 1 and type 2. All forms are characterized by improper processing of glucose by the body. Sugar accumulates in the blood, which leads to complications.
You should be careful when planning a pregnancy if you have type 1 diabetes. This diagnosis is given to a person for life; every expectant mother who is ready to take risks and give birth to a healthy child will have to overcome difficulties during the development of the baby.
Risks and consequences
Pregnancy with insulin-dependent diabetes mellitus is a dangerous period. The body of mother and baby is exposed to negative influences. In the first trimester of pregnancy, the fetus may experience:
- cleft palate;
- pathologies of the development of organs, their rudiments, changes in location;
- vertebral hernias.
In the second and third trimester there is a risk:
- chronic lack of oxygen (fetal hypoxia);
- cessation of fetal development.
Even after birth, the baby is susceptible to diseases, hypoglycemia, jaundice, etc. may occur. The postnatal period for such newborns is very difficult.
Definition, forms of the disease
Diabetes mellitus is an endocrine disease. It occurs due to a lack of insulin, a pancreatic hormone, in the blood. This substance is responsible for ensuring that glucose enters all cells of the human body.
Diabetes has several forms:
- Insulin dependence is an autoimmune disease. It occurs due to a lack of insulin in the body due to disruption of the pancreas. This form cannot be treated.
- Insulin-independent – older people are susceptible; the disease progresses due to the fact that cells lose sensitivity to insulin. For therapy you need to take medications and maintain a diet.
Reasons for development:
- excess body weight;
- heredity;
- metabolic disease;
- use of certain medications (steroid hormones, diuretics;
- atherosclerosis;
- vascular diseases;
- disruption of the pancreas;
- adrenal insufficiency;
- elderly age;
- neuroses, constant stress.
Negative consequences during pregnancy:
- death of the fetus in the womb;
- polyhydramnios;
- intrauterine development disorder;
- problems with uterine tone;
- late gestosis;
- jaundice in a baby;
- blurred vision;
- premature aging of the placenta;
- premature birth.
Pregnancy planning, management, planned hospitalizations
If a woman nevertheless decides to carry and give birth to a child, the very first thing to do is to notify the specialists caring for the patient: a gynecologist, an immunologist, an endocrinologist. It is also necessary to take tests for 3 months before planning a pregnancy. With stable glucose levels, you can begin to conceive.
3 hospitalizations, routine examinations, and additional tests are prescribed. First, the woman is sent to the clinic in the first trimester. Hospitalization is needed to correct blood counts and identify possible deviations from the norm.
The second occurs at 18-20 weeks. This time, gynecologists examine the development of the fetus and correct metabolic processes in the mother’s body.
The third time hospitalization is needed at 35 weeks. A pregnant woman is being prepared for the upcoming birth.
DEFINITION OF DIABETES MELLITUS AND ITS CLASSIFICATION
Diabetes mellitus is a group of metabolic diseases characterized by hyperglycemia, which results from defects in insulin secretion, insulin action, or both (WHO, 1999)
CLASSIFICATION OF DIABETES MELLITUS
(WHO, 1999)
SD type | Characteristics of diseases |
| Diabetes mellitus type 1 • Autoimmune • Idiopathic | Destruction of $-cells of the pancreas, usually leading to absolute insulin deficiency |
| Diabetes mellitus type 2 | With predominant insulin resistance and relative insulin deficiency or a predominant defect in insulin secretion with or without insulin resistance |
| Gestational diabetes mellitus | Occurs during pregnancy |
| Other types of diabetes* | • Genetic defects of function β-cells • Genetic defects in insulin action • Diseases of the exocrine pancreas • Endocrinopathies • Drug or chemical induced diabetes • Diabetes induced by infections • Uncommon forms of immune-mediated diabetes • Other genetic syndromes associated with diabetes mellitus |
Chronic complications of diabetes include vascular complications (micro- and macroangiopathies) and neuropathies.
Diabetic microangiopathies include:
Diabetic retinopathy (DR) is a microangiopathy of the retinal vessels in diabetes mellitus, which in the terminal stage leads to complete loss of vision.
Diabetic nephropathy (DN) is a specific damage to the renal vessels in diabetes mellitus, accompanied by the formation of nodular or diffuse glomerulosclerosis, the terminal stage of which is characterized by the development of chronic renal failure (CRF).
Diabetic macroangiopathies include:
- coronary heart disease and heart failure (as a complication of coronary artery disease);
- cerebrovascular diseases;
- peripheral angiopathy.
Diabetic neuropathy is damage to the nervous system caused by diabetes.
Emergency conditions for diabetes
Uncontrolled hyperglycemia can lead to ketoacidotic coma (more often in type 1 diabetes) or hyperosmolar coma (more often in type 2 diabetes). These life-threatening conditions require a complex of emergency treatment measures.
- Ketoacidotic coma
- Hypoglycemic coma
- Hyperosmolar coma
- Hyperlactic acidemic coma
DIAGNOSIS OF DIABETES MELLITUS
Diagnostic criteria for diabetes and other disorders of carbohydrate metabolism (WHO, 1999)
| GLUCOSE CONCENTRATION, mmol/L (MG/%) | |||
| Whole blood | Plasma | ||
| Venous | Capillary | Venous | |
| NORM | |||
| On an empty stomach and 2 hours after TSH | 3,3-5,5 (59-99) | 3,3-5,5 (59-99) | 4,0-6,1 (72-110) |
| <6,7 (<120) | <7,8(<140) | <7,8(<140) | |
| DIABETES | |||
| On an empty stomach or 2 hours after TSH or 2 hours after a meal (postprandial glycemia) or random determination of glycemia at any time of the day, regardless of meal time | ≥6,1 (≥110) | ≥6,1 (≥110) | ≥7,0 (≥126) |
| ≥10,0 (≥180) | ≥11,1 (≥200) | ≥11,1 (≥200) | |
| ≥10,0 (≥180) | ≥11,1 (≥200) | ≥11,1 (≥200) | |
| IMPAIRED GLUCOSE TOLERANCE | |||
| On an empty stomach (if determined) and 2 hours after TSH | <6,1 (<110) | <6,1 (<110) | <7,0(<126) |
| 6,7-10,0 (120-180) | 7,8-11,1 (140-200) | 7,8-11,1 (140-200) | |
| On an empty stomach and after 2 hours (if determined) | IMPAIRED FASTING GLYCEMIA | ||
| ≥5,6 (≥100) <6,1 (<110) | ≥5,6 (≥100) <6,1 (<110) | ≥6,1 (≥110) <7,0 (<126) | |
| <6,7 (<120) | <7,8(<140) | <7,8(<140) | |
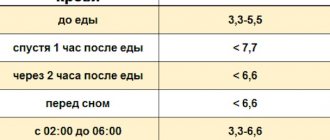
Fasting glucose refers to the blood glucose level in the morning before breakfast after a prior fast of ≥8 hours.
Postprandial glycemia is the blood glucose level 2 hours after a meal.
Glycated hemoglobin (HbAl c) - This indicator allows you to evaluate the average level of glycemia over 1.5-2 months [2,8,17]. Under physiological conditions, its level is 3-6%.
Pump insulin therapy. The device currently in use is a continuous glucose monitoring device, which is a device the size of a pager (pump). It is equipped with a subcutaneous sensor that calculates glucose levels every 5 minutes, recording up to 288 glucose values per day. The device can be used in patients with various types of diabetes in outpatient and inpatient settings[2,8,9].
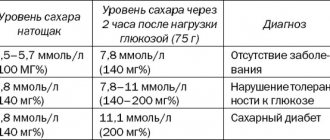
Gestational diabetes mellitus (GDM) is an impairment of glucose tolerance of varying severity that occurs during pregnancy. In a five-year, blinded, randomized study, Hyperglicemia and adverse pregnancy outcomes (HAPO) examined 25,505 pregnant women of different ethnic groups. In 15 largest centers in nine countries, they underwent PTG with 75 g of glucose at 24-32 weeks of pregnancy. The study results demonstrated a strong relationship between maternal hyperglycemia and neonatal outcomes. In 2010, the International Association of Diabetes and Pregnancy Study Groups (IADPSG), based on the HAPO study, proposed new criteria for the diagnosis of GDM. Currently, the diagnosis of “impaired glucose tolerance” is not used during pregnancy. Any disorder of carbohydrate metabolism that first appeared or was identified during pregnancy is defined as
Manifestations of GDM are usually hidden and can be detected in risk groups after a glucose tolerance test (TSG).
Risk groups for developing GDM:
| OPTIONS | HIGH RISK | MODERATE RISK | LOW RISK |
| Overweight (>20% of ideal) | Yes | Yes | No |
| Type 2 diabetes in close relatives | Yes | No | No |
| History of GDM | Yes | No | No |
| Impaired glucose tolerance | Yes | No | No |
| Glucosuria during previous or current pregnancy | Yes | Not really | No |
| History of hydramnios and large fetus | Not really | Yes | No |
| Birth of a child weighing more than 4000 g or a history of birth control | Not really | Yes | No |
| Rapid weight gain during this pregnancy | Not really | Yes | No |
| Woman's age over 30 | Not really | Yes | <30 years |
Glucose tolerance test procedure
To diagnose GDM, a glucose tolerance test (TGT) is used, which is performed against the background of a normal diet without restriction of carbohydrates. The study is carried out on an empty stomach, no earlier than 10 hours after the last meal. After determining the fasting blood glucose level, the patient is asked to drink a solution with 75 g of glucose. During TSH, a pregnant woman should refrain from physical activity, eating, and smoking. Next, the glucose level is determined 1 hour and 2 hours after the glucose load.
Diagnosis and screening of GDM
Criteria for identifying GDM based on TSH
| Load | On an empty stomach | After 1 hour | After 2 hours | After 3 hours |
| 50 g glucose | >5.3 mmol/l | >7.8 mmol/l | – | – |
| 100 g glucose | >5.3 mmol/l | > 10.0 mmol/l | >8.6 mmol/l | >7.8 mmol/l |
GDM is diagnosed if the normal level is exceeded by at least 2 of the given indicators for OPT with 100 g of glucose. If only 1 of them is exceeded, the test is repeated after 2 weeks.
Hormonal and metabolic changes during pregnancy in patients with diabetes
Physiological pregnancy in the early stages is accompanied by increased glucose utilization and an increase in the amount of adipose tissue in the mother’s body. The main hormonal and metabolic changes during pregnancy are associated with the formation of a new endocrine organ - the placenta, which secretes protein and steroid hormones (chorionic gonadotropin, placental lactogen, progesterone, estrogens). The hormonal function of the placenta is associated with the mobilization of fat from the depot and a decrease in the utilization of glucose by insulin-sensitive tissues. Developing insulin resistance contributes to an increased use of lipid metabolism products, while glucose is saved to feed the fetus, for which it is the main source of energy. During pregnancy, fasting blood glucose levels decrease. Glucose and ketone bodies easily pass through the placental barrier. Insulin does not cross the placental barrier. Hyperglycemia in the mother promotes increased transfer of glucose across the placenta and causes hyperplasia of β-cells of the pancreatic islets in the fetus, hyperinsulinemia and, as a consequence, fetal macrosomia.
Due to increased glucose utilization in early pregnancy, a decrease in insulin requirements is observed, reaching minimum values at 9-11 weeks of pregnancy (89.3% of the initial level). In order to adequately and timely reduce insulin doses, it is necessary to determine blood glucose levels more often (6-8 times a day). With the onset of the second half of pregnancy and the development of insulin resistance, the need for insulin gradually increases, reaching maximum values at 32-33 weeks (140-160% of the original).
From the 35th week of pregnancy, there is a gradual decrease in the need for insulin with a sharp decrease towards childbirth to 80-75% of the initial level. A decrease in insulin requirements may begin earlier in cases of severe placental insufficiency (PI, which is often found in patients with vascular complications of diabetes and may require early delivery). Insulin requirements remain low during the first two days of the postpartum period. Starting from the 3rd day of the postpartum period, the need for insulin begins to increase and quickly reaches the initial level.
The effect of pregnancy on vascular complications of diabetes depends on the degree of diabetes compensation before and during pregnancy, the severity of diabetes complications before pregnancy, and the addition of preeclampsia. A third of patients experience transient worsening of retinopathy and nephropathy with unsatisfactory compensation of diabetes.
Management of pregnancy in patients with diabetes mellitus
Management of pregnancy during diabetes requires clear definition of goals:
- Achieving normoglycemia
- Preventing the development of complications
- Stabilization of existing complications
- Maintaining pregnancy to term (minimum 38 weeks)
- Preventing obstetric complications:
preeclampsia
polyhydramnios
urinary tract infections
To successfully achieve your goals, a team approach of specialists in the management of pregnant women and patients with diabetes is necessary:
- Endocrinologist
- Obstetrician-gynecologist
- Neonatologist
- Ophthalmologist
Absolute contraindications for prolonging pregnancy in diabetes mellitus are::
- severe nephropathy with creatinine clearance less than 50 ml/min, daily proteinuria 3.0 g or more, blood creatinine more than 120 mmol/l, arterial hypertension;
- severe coronary heart disease;
- progressive proliferative retinopathy.
Pregnancy is undesirable if:
- HbA1c >7.0% in early pregnancy;
- development of diabetic ketoacidosis in early pregnancy;
- presence of diabetes in both spouses;
- combination of diabetes mellitus with Rh sensitization in the mother;
- combination of diabetes and active pulmonary tuberculosis;
Pregnancy that develops against the background of diabetes mellitus carries a risk to the health of the mother and fetus.
Risk factors for a mother with diabetes:
- progression of vascular complications (retinopathy, nephropathy, ischemic heart disease);
- frequent development of hypoglycemia, ketoacidosis;
- frequent complications of pregnancy (preeclampsia, infection, polyhydramnios).
Risk factors for the fetus:
high perinatal mortality;
congenital anomalies (2-4 times higher);
neonatal complications;
risk of developing diabetes:
- 1.3% - if the mother has type 1 diabetes,
- 6.1% - if the father has type 1 diabetes.
Treatment tactics for diabetes during pregnancy
In the treatment of diabetes during pregnancy, the main goal is to achieve normoglycemia , when the level of glucose in the blood does not go beyond physiological fluctuations (3.5-6.7 mmol/l).
The principles of diet therapy are the exclusion of easily digestible carbohydrates, split meals (5-6 times with an interval of 2-3 hours.) Products that must be completely excluded from the diet include sugar, jam, sweets, baked goods, ice cream, factory juices, other sugar-sweetened drinks, grapes, bananas. The diet is prescribed taking into account body weight and must contain a sufficient amount of calories (at least 1700 kcal per day). 50-55% of the diet should be carbohydrates, 20-25% proteins and 20% fats. Food should contain sufficient fiber. Slowly digestible carbohydrates should be represented by potatoes, cereals (buckwheat, millet, pearl barley, oatmeal) and wholemeal bread. When calculating the calorie content of food, it is convenient to use “bread unit” equivalents. To assimilate one bread unit (10-12 g of carbohydrates) 1-2 units of insulin are required [2,5,8,9].
Bread unit (XE, carbohydrate unit) is a conventional unit developed by nutritionists, used to approximate the amount of carbohydrates in foods: one XE is equal to 10 (excluding dietary fiber) or 12 grams (including ballast substances) carbohydrates or 20 (25) g. bread.
Insulin therapy has been used in the treatment of diabetes since 1922 and is prescribed by an endocrinologist. For 60 years, insulins produced from the pancreas of cows and pigs have been used. Since 1985, human insulin has been produced using genetic engineering. According to the duration of action, all insulins are divided into 4 groups: ultra-short, short, medium and long-acting. The main route of insulin administration is subcutaneous. intramuscular and intravenous insulin administration is indicated only for ketoacidosis. There are traditional and intensive (basal-bolus) insulin therapy. The most modern method of intensive insulin therapy is intensive subcutaneous administration of insulin using a specialized dispenser (pump insulin therapy) [2,9].
For type 1 diabetes, insulin therapy is the main treatment method. In the absence of compensation in pregnant women with type 2 diabetes and GDM, insulin therapy is prescribed while following a diet. The use of oral hypoglycemic drugs and biguanides during pregnancy is contraindicated due to their teratogenic effects. Transfer to insulin therapy in pregnant women with type 2 diabetes is required in almost 40% of patients [8,15]. In GDM, the need for insulin therapy occurs in 10-30% of cases [13].
Algorithm for managing pregnant women with diabetes mellitus
Maintaining an adequate diet:
- calorie content: 1st trimester - 30 kcal/kg BMI,
2 - 3rd trimesters - 35-38 kcal/kg BMI;
- composition: proteins - 15%, fats - 30%,
carbohydrates - 55% (mostly complex).
protein consumption 1.5 - 2.0 g/kg.
- tableted hypoglycemic drugs
Intensive insulin therapy with genetically engineered human insulins.
Regular self-monitoring of glycemia in order to maintain normoglycemia:
- fasting glucose 3.5 - 5.5 mmol/l;
- glycemia after meals 5.0 - 7.8 mmol/l.
Monitoring HbA1c every trimester; the goal is ≤6.5%.
Observation by an ophthalmologist - examination of the fundus once every trimester.
Observation by a gynecologist and diabetologist
(weight, blood pressure, albuminuria are measured at each visit):
- up to 34 weeks of pregnancy - every 2 weeks;
- after 34 weeks - weekly.
Condition of the fetus and newborn
The negative impact of hyperglycemia and ketonemia in early pregnancy is manifested by an increase in the incidence of fetal malformations (diabetic embryopathy). The incidence of fetal malformations in type 1 and type 2 diabetes is 9.5%, and in decompensated diabetes it increases to 20%. The most common defects of the cardiovascular system are anencephaly and anal atresia. In the first 9-12 weeks of pregnancy, the fetus does not yet produce its own insulin. Maternal hyperglycemia during this period of pregnancy causes an increased risk of congenital malformations. An increased level of glucose in the mother’s blood leads to hyperglycemia in the fetus and hypersecretion of insulin by its pancreas, which leads to the development of a symptom complex - “diabetic fetopathy”, the main symptom of which is macrosomia. Excess insulin leads to an increase in the size of the fetus and placenta, inhibits the maturation of the fetal central nervous system, the surfactant system in the lungs, the adrenal cortex, and the hematopoietic system. In this case, hypertrophy of some organs (heart, adrenal glands, liver, kidneys) can be combined with a decrease in the size of others (brain, thymus gland). In addition, fetal hyperinsulinemia inhibits lecithin synthesis. This explains the increased incidence of respiratory distress syndrome observed in children of diabetic mothers. If hyperglycemia is noted shortly before birth, then after birth the child experiences hypoglycemia, the cause of which is persistent high insulinemia with a sudden cessation of the flow of glucose, which previously came through the umbilical vein from the mother. Therefore, immediately after birth, the baby needs an infusion of glucose. Because these hypoglycaemias can be prolonged, in most cases it is necessary to observe the baby of a mother with diabetes for several days in the neonatology department.
On ultrasound, diabetic fetopathy is indicated by a double body contour resulting from excessive deposition of subcutaneous fat.
Achieving and maintaining normoglycemia before and throughout pregnancy significantly reduces the incidence of malformations and perinatal complications of the fetus.
Delivery tactics
The optimal period is 38 - 40 weeks.
The optimal method is programmed vaginal delivery with careful glycemic control during and after birth.
Indications for caesarean section:
- generally accepted in obstetrics;
- the presence of severe or progressive complications of diabetes and pregnancy;
The most common complications during childbirth are premature rupture of amniotic fluid (20-40%), weakness of labor (20-30%). During childbirth with a large fetus, there is a high risk of birth canal injuries, shoulder dystocia and clavicle fracture. On the day of birth, insulin doses must be reduced by 2-2.5 times; in the postpartum period, starting from the 3rd day, insulin doses increase [2,8,9].
Tactics for managing patients after childbirth
Reducing the insulin dose.
Breastfeeding (warn about the possible development of hypoglycemia!).
Control of compensation, complications, weight, blood pressure.
- For GDM: reclassification of the state of maternal carbohydrate metabolism no later than after 6 weeks. after childbirth (with normal glycemic values - repeat examinations once every 3 years; if impaired tolerance to carbohydrates is detected - once a year).
contraception 1.0-1.5 years
Features of the flow
From the moment of conception until childbirth, the expectant mother should be under the supervision of doctors and, if necessary, immediately seek help. Diabetes is a test that during pregnancy intensifies its unpleasant moments:
- In first place among the negative sensations during pregnancy and during type 1 diabetes is toxicosis, there is a risk of developing ketoacidosis. Most often, discomfort begins from the very first weeks.
- Hypoglycemia may occur due to abnormal blood sugar levels.
- Women have an increased risk of developing diseases: neuropathies, nephropathy.
- Bleeding and pregnancy failure in the three trimesters are possible.
- Due to toxicosis after an insulin injection, you may need to repeat the injection. The necessary elements leave the body with vomit.
- It is imperative to monitor the dosage of the administered drug.
Preventing Gestational Diabetes
Unfortunately, there are no 100% effective measures that would protect against this disease.
But the more useful habits a woman develops before pregnancy, the easier pregnancy and childbirth will be:
- From the first days of pregnancy, eat healthy foods: choose foods high in fiber and low in fat. Focus on vegetables and whole grains. Strive for variety and watch portion sizes.
- Stay active. Try to devote 30 minutes to sports every day. Take daily walks, ride a bike, or go swimming.
- Plan your pregnancy at a healthy weight and don't gain more than recommended. Excessively rapid weight gain can increase the risk of gestational diabetes.
Although there is no universal protection against GDM, you can reduce your risk of developing it through a healthy lifestyle.
The most important thing is to detect the problem in time and prevent it from developing. Author:
Baktyshev Alexey Ilyich, General Practitioner (family doctor), Ultrasound Doctor, Chief Physician
Additional tests
Glucose is a source of energy and growth for the fetus. When it enters the body of the future newborn in excess, problems begin. In each trimester, a pregnant woman should undergo tests such as:
- examination by a nephrologist, ultrasound of the genitourinary system;
- general and detailed blood test, fasting glucose level should be up to 6.1 mmol/l. After eating 2 hours - no more than 7.4 mmol/l. If the rate is above 7%, conception is not recommended at all.
- urine test, 2-3 times a month;
- biochemistry;
- coagulogram;
- leukocyte count;
- fluorography;
- ECG;
- take a stool test.
Childbirth with diabetes
At the end of the term, a month before the expected date of birth, the woman undergoes a final examination in the hospital to determine the type of delivery. If you are allowed to give birth on your own naturally, they usually follow the same pattern:
- The doctor punctures the amniotic sac.
- Oxytocin, insulin and, if necessary, pain medication are administered.
- The fetus is monitored using CHT, the doctor monitors the level of insulin in the mother's blood.
Each case is considered individually.
Fetal development
The main and crucial period is the beginning of fetal development. In the first trimester, most vital organs are formed. The child is not yet formed, so it actively feeds at the expense of the mother. An increase in blood glucose levels is fraught with the development of hyperglycemia in the unborn baby. Also, the organs of the nervous and cardiovascular systems are no less susceptible to pathologies.
From the 12th week of pregnancy, the condition of mother and child becomes better. The fetus develops its own pancreas, which produces insulin independently. It is important to carry out the necessary tests to monitor blood glucose levels and prevent unwanted complications.
The worst thing that can happen is termination of pregnancy, miscarriage, bleeding. The development of abnormalities in the development of the fetus (cleft lip, absence of organs) also dangerous To maintain the health of the baby and mother, it is necessary to take pregnancy and its planning seriously. Take tests according to the doctors’ schedule, do not neglect the recommendations. With diabetes, it is difficult to bear a healthy baby, but with desire and effort, it is possible. The main thing in this period is blood glucose control. Complications from the disease can be avoided.
Causes of Gestational Diabetes
The exact mechanism of the disease is still not completely clear.
Doctors are inclined to believe that the hormones responsible for the proper development of the fetus block the production of insulin, which leads to disruption of carbohydrate metabolism. During pregnancy, more glucose is required for both the woman and the baby. The body compensates for this need by suppressing insulin production. There are other possible causes of gestational diabetes, such as autoimmune diseases that destroy the pancreas. In principle, any pancreatic pathology can increase the risk of diabetes during pregnancy.
Insulin requirement, how the course of therapy changes
Each trimester has its own need for the drug. In the first and third stages, the need for insulin decreases, in the second it increases. For each expectant mother, the dose and type of insulin are individually calculated for the entire period of pregnancy for insulin-dependent diabetes.
With appropriate control of blood sugar levels and correction of the amount of insulin administered, the baby will not have diabetes (but there is no escape from a predisposition to the disease). So a newborn should not be left unattended.
Gynecologists at the clinic where the birth will take place need to prepare in advance for possible complications and emergency situations. By considering all options for the development of pregnancy and childbirth, pathologies can be avoided.
Risk factors for gestational diabetes
- Age under 18 and over 30 years old.
- Unbalanced diet with a lot of fast carbohydrates.
- Bad habits (smoking, alcohol abuse).
- Overweight and obesity. Excess weight obviously implies a violation of metabolic processes.
- Lack of physical activity.
- Previous gestational diabetes or prediabetes. The tendency to diseases of this series does not disappear over time.
- Polycystic ovary syndrome.
- A close relative has diabetes. The risk of gestational diabetes increases twofold or more if close relatives have any form of diabetes.
- Previous birth of a child over 4 kg or a large fetus during the current pregnancy.
- Race. Caucasians have the lowest risk of developing gestational diabetes, and black women are most likely to suffer from this problem.
Unfortunately, GDM can develop in a completely healthy woman without risk factors, so you need to visit a doctor and not skip recommended screenings.
Recommended Diet
Even a healthy woman is required to follow a proper diet. For pregnant women who suffer from diabetes, the food entering the body is especially important. The content of sucrose in it is excluded, as before. Also, the expectant mother should control her carbohydrate intake and count calories. The disease weakens a woman’s body, and the process of glucose absorption may be further disrupted.
Eliminate from your diet:
- fruit juices;
- fast food;
- dates;
- pasta;
- fried potatoes;
- bananas;
- artificial drinks (exclude all carbonated drinks);
- milk, etc.
Treatment of diabetes during gestation
Treatment for diabetes while pregnant includes taking insulin and a certain diet. The medicine and dosage will be prescribed by the attending physician.
Nutrition rules:
- reduce the amount of carbohydrates consumed, and proteins need to be increased;
- you need to eat at least 2000-2200 kilocalories per day, if you are overweight - 1600-1990 kilocalories;
- sweets are prohibited;
- fractional meals, approximately 8 times a day;
- It is necessary to consume vitamins A, B, C, D.
Additionally, you need to drink special herbal teas: from blueberry leaves, flax seeds, green beans. If there are no contraindications, then it is necessary to engage in physical exercise. They perfectly tone the body, improve well-being and prepare the ligaments for childbirth.
Diabetes and male infertility
According to statistics, infertility in men with diabetes develops in approximately 30% of cases.
In diabetes, the walls of blood vessels thicken (including small capillaries), changes occur in the blood coagulation system, and blood flow slows down. Due to poor circulation in the pelvis, impotence may develop, since an erection requires a rush of blood (about one hundred and fifty milliliters). In addition, long-term diabetes can lead to autonomic diabetic neuropathy, that is, damage to the nerves of the peripheral nervous system, which are also responsible for erection.
Diabetic neuropathy is also the cause of retrograde ejaculation - the reflux of sperm in the opposite direction - into the bladder. This occurs due to a violation of the muscle tone of the bladder sphincter. If he is in a relaxed state, then the ejaculate is sent along the path of least resistance - in the opposite direction.
In addition, the cause of male infertility in diabetes is a decrease in testosterone. Actually, the cause-and-effect relationship is as follows: decreased testosterone production is one of the causes of obesity, and excess weight is one of the risk factors for developing diabetes in men. At the same time, under the influence of aromatase, an enzyme that is present in adipose tissue, testosterone is converted into the female hormone estradiol. Insufficient testosterone levels negatively affect a man’s reproductive function, worsening the process of spermatogenesis (the formation and maturation of sperm).
Research shows that men with diabetes are more likely to have sperm DNA damage.
Treatment of infertility in men with diabetes
Treatment of male infertility in diabetes mellitus may involve various methods, including the use of IVF + ICSI. In particular, in azoospermia caused by retrograde ejaculation, germ cells can be obtained from the patient's urine. The embryologist then selects the sperm with the best characteristics and places it inside the egg.
Patients diagnosed with diabetes need to undergo a full examination, on the basis of which the doctor will be able to prescribe the optimal infertility treatment regimen in this case.
If you have any questions, you can ask them to the Nova Clinic doctors. You can make an appointment with specialists by calling the phone number listed on the website or using the booking button.