Diabetes mellitus is common in patients with hypertension and significantly increases the risk of cardiovascular disease, including myocardial infarction, stroke, and peripheral vascular disease. Pharmacological therapy in patients with hypertension and diabetes is controversial due to concerns about the metabolic effects of some antihypertensive agents, as well as concerns about the safety of calcium antagonists. Therefore, diet, lifestyle changes and knowledge about proper prevention of disease progression are the key to maintaining health and reducing the risk of developing cardiovascular complications.
Factors affecting blood pressure
The cause is unknown in most cases. This is called essential hypertension. The pressure in the blood vessels depends on how hard the heart pumps blood and how much resistance the blood vessels (arteries) offer. The slight narrowing of the arteries is thought to increase resistance to blood flow, which increases blood pressure.
What Causes High Blood Pressure?
Most people don't have a single reason. However, there are a number of things that increase the likelihood of its occurrence. These are the so-called risk factors:
- The influence of nicotine.
- Excessive consumption of salt or processed foods (convenience foods, canned foods, smoked foods).
- Alcohol abuse.
- Having excess weight.
- Insufficient physical activity.
- Private stress, which provokes the release of adrenaline and cortisol.
In addition, diabetic nephropathy, a complication that develops in some people with diabetes, can cause hypertension in patients with diabetes. In this condition, the kidneys are damaged, which can cause high blood pressure due to damage to the arteries, arterioles, tubules and glomeruli of the kidney tissue. It is more common in people with type 1 diabetes. In rare cases, high blood pressure is caused by other medical conditions. This is then called secondary hypertension. For example, kidney problems or hormonal imbalances can cause high blood pressure.
Diabetes comes in different forms
Murzaeva Irina Yurievna
Endocrinologist, Preventive medicine
May 23, 2019
Something is starting to tire of the modern way of presenting information, especially of a medical nature. Now there are a great many blogs, everyone writes something - who can and who can’t, actively accompanying the text with photographs of themselves in “different poses” :). Medical information is often “corresponded (copied)” from each other, as a result - nothing new or interesting, and most importantly, little reliable and truthful.
Therefore, in this article they will not write a theory, so much is said and written about diabetes, in the end it is not only not cured, but often they cannot even compensate for blood sugar decently. I would like to present and describe all the variety of forms of diabetes that occur, try to reflect that not everything is so simple and that diabetes is divided not only into types 1 and 2... And the best way to present this is clinical cases from practice.
Male, 65 years old. Diabetes mellitus type 2 for more than 15 years, was on PSSP therapy for a long time (oral hypoglycemic drugs), first on therapy with 2 types of drugs, then 3 types of drugs, over time - PSSP stopped “restraining” increasing glycemia, was transferred to insulin therapy, but the combination and selection of different insulins poorly compensated for the high blood glucose levels. Result - intestinal carcinoma was detected, after the operation I lost weight, returned to therapy with 2 types of PSSP, insulin therapy was discontinued. Keep blood sugar within 6-7 mmol/l. Conclusion: in cases of long-term uncompensated diabetes, especially with an active change in therapy (its complication), especially in young people 45+, it is necessary to exclude oncopathology of any nature.
Woman, 45 years old. Type 2 diabetes mellitus (?) developed against the background of normal weight. Antibodies to GAD (an autoimmune marker of pancreatic inflammation were negative). I received 2 types of PSSP. I rarely came to see her, once a year. In the 5th year of diabetes, she began to actively lose weight, her blood sugars increased - she was switched to insulin therapy, the weight was not restored, blood sugars continued to rise, an ultrasound scan of the pancreas showed a tumor of the pancreas, which was later confirmed by an MRI of the pancreas, the tumor was discovered at a late stage. Upon active questioning of relatives, two direct relatives in the family had pancreatic cancer with an early outcome before 55 years of age. Conclusion: as in the first case.
Woman, 37 years old. Blood sugar increases gradually over the course of a year, maximum figures are 11 mmol/l.
There is no family history of diabetes. Normal weight, not actively losing weight. During the examination, a high titer of antibodies to GAD was revealed, confirmed 2 times, and a decrease in pancreatic reserve (as measured by a decrease in insulin and blood c-peptide 1 hour after meals). The diagnosis of LADA - diabetes was confirmed. It was decided to proceed to PSSP, since there is no ketoacidosis. For 4 months without insulin therapy, blood glucose remains at 5-6 mmol/l.
Conclusion: all young people need to take antibodies to pancreatic cells (antibodies to GAD, insulin, etc.) to make a diagnosis.
Woman, 37 years old. Gestational diabetes mellitus was diagnosed during pregnancy, according to her, which could not be compensated for by high doses of Lantus (more than 22 units/day) and Novorapid (more than 12 units/day); after childbirth, blood sugar continues to rise above 8 mmol/l on an empty stomach against the background of insulin withdrawal!
During the examination, no antibodies to pancreatic cells were detected, but the reserve of the pancreas was sharply reduced (increase in insulin and c-peptide 1 hour after eating no more than 30%). Diagnosis: Diabetes mellitus type 1, antibody-negative, detected during pregnancy! Further insulin therapy was prescribed given the low pancreatic reserve. Conclusion: during pregnancy it is necessary to more carefully control blood sugar - in this case, type 1 diabetes debuted, mistaken for gestational diabetes mellitus.
Male, 60 years old. From the medical history, he was admitted to hospital 3 years ago with blood sugar 25 mmol/l, mild ketosis (urine acetone +), a diagnosis of diabetes mellitus type 2 was made, combination therapy was prescribed - long-term + short-term insulin. Who canceled on his own 3 months after hospitalization, continuing to follow table No. 9, has NOT received PSSP and insulin therapy for 3 years!!! Blood sugar is maintained at 5-6 mmol/l, and does not lose weight. The diagnosis is unclear. Conclusion: in the tests carried out earlier and submitted for admission, there are no tests for antibodies to the pancreas, c-peptide, insulin, not to mention a genetic test for the type of diabetes. Missing examinations were ordered.
Male, 28 years old. Fasting blood sugar up to 8.0 mmol/l, after meals within normal limits, an increase was registered several years ago. When following a diet, glycemia is 4-5 mmol/l. During examination, antibodies to the pancreas are negative, the pancreas reserve is preserved (insulin and c-peptide 1 hour after meals are normal). That is, there is no data for diabetes mellitus type 1, 2 and no LADA. A decision was made to take tests to rule out MODY diabetes. Conclusion: MODY diabetes is a rare, but still occurring form of diabetes, is a consequence of a point genetic mutation of various types, is divided into more than 13 subtypes, and is a copy of type 2 diabetes (but in young people).
Boy, 22 years old. Blood sugar increased gradually, weight was low (initially). There was no ketoacidosis. There are no relatives with diabetes. When examining the function of the pancreas, there is a gradual decrease in its function, without increasing the titer of antibodies to GAD and insulin. Treatment began on DDP4 drugs - this is a type of PSSP. Gradually he was switched to long-term insulin, then short-term insulin 3-4 times a day with food injections. Pancreatic function decreased sharply over 4 years. Probable diagnosis: slowly progressive type 1 diabetes mellitus, without antibodies (seronegative). Conclusion: the diagnosis of diabetes mellitus can sometimes be made only retrospectively, assessing the course of diabetes “over time.”
Woman, 33 years old. She was examined for pregnancy planning due to obesity; no metabolic abnormalities were detected. But pregnancy was delayed for 1.5 years. After 1.5 years, she was re-referred by a gynecologist: a sharp increase in liver transaminases (ALT, AST, GGTP) by more than 3-4 times and an increase in blood sugar above 7.0 mmol/l, during the period of absence she gained weight. A detailed examination revealed - type 2 diabetes mellitus, insulin resistance, fatty hepatitis. Considering pregnancy planning, insulin therapy was prescribed to compensate for type 2 diabetes. Conclusion: if type 2 diabetes is diagnosed at a young age, pregnancy can only be managed with insulin therapy; PSSPs are not allowed for pregnancy in Russia.
Man, 72 years old. He has been suffering from type 1 diabetes since he was 23 years old!!!!!! At his age, he only has: stage 1 diabetic retinopathy, nephropathy in the proteinuria stage, no evidence of chronic renal failure, diabetic serso-motor neuropathy (the most severe of all complications). Acute cardiovascular accidents (heart attack, insulin) could not be tolerated!! Conclusion: type 1 diabetes does not imply an “early outcome” (life expectancy can be normal, as in people without diabetes), complications can be prevented by satisfactory compensation of diabetes.
Male, 48 years old. History of acute pancreatic necrosis (acute inflammation - “melting” of the pancreas), which suggests the death of more than 70%-80% of pancreatic cells. Survived. He was discharged from the hospital on combined insulin therapy, and later, 8-12 months after the acute condition, he was completely removed from insulin therapy, and for the past 3 years he has been receiving only tablet forms of PSSP. Conclusion: there is always an exception to any statistics, pancreatic necrosis, which implies high mortality and lifelong insulin therapy is NOT a death sentence!
… And that is not all..
How is blood pressure measured?
Blood pressure is measured using a device called a tonometer. A cuff (thick tape) is placed on the arm.
As air is inflated, the cuff tightens and then slowly relaxes again. During this relaxation, you can listen to the pulsation of the arteries and record the first and last tone to record blood pressure readings. Blood pressure is measured in millimeters of mercury. After the study, the result will be recorded in two numbers: the first is systolic pressure (during ventricular contraction), the second is diastolic pressure when the heart muscle is at rest. According to the principle of operation, tonometers are automatic and manual. When using a manual tonometer, air is pumped using a special bulb, and the first and last tone is heard using a stethoscope.
The automatic blood pressure monitor inflates the cuff and catches the pulse itself. Also, such devices measure heart rate and have a built-in memory for recording readings. It is much more convenient than manual ones, especially for older people.
conclusions
The relationship between sugar and blood pressure in modern medical science is quite obvious. High blood glucose levels in diabetes, as well as increased consumption of sweets by healthy people, lead to the development of hypertension, and therefore the product is contraindicated in such patients. It is better to use its safer analogues - honey or dried fruits.
On the other hand, in case of hypotension, sugar has a positive effect and, in reasonable quantities, is able to restore reduced blood pressure.
Treatment and prevention of high blood pressure
To avoid a diagnosis of hypertension, patients with diabetes need to adjust their lifestyle in the following ways:
- Maintain a healthy weight. Overweight people should try to lose weight, while people of normal weight should avoid gaining weight. If you are overweight, losing just 5 kg can help prevent hypertension. Talk to your doctor about the most appropriate weight for you.
- Eat a balanced diet. Eat plenty of fruits and vegetables, especially those rich in potassium, and limit your intake of excess calories, fat and sugar. Consider following the Dietary Approaches to Control Hypertension, or DASH diet, which has been shown to help control blood pressure in patients with diabetes.
- Reduce the amount of salt. A low-sodium diet can help maintain normal blood pressure. The higher your sodium intake, the higher your blood pressure. You can reduce your overall salt intake by avoiding packaged and processed foods that are high in sodium and not adding extra salt to your meals.
- Exercise regularly. Get moving to prevent hypertension. Physical activity is critical. The more you exercise, the better, but even light exercise can help control your blood pressure. Moderate exercise for 30 minutes three times a week is a good start.
- Limit your alcohol intake. Excessive alcohol consumption can lead to high blood pressure.
- Check your blood pressure regularly. If your doctor detects early signs of hypertension (prehypertension), additional precautions may be needed to correct the condition.
Take a look at your lifestyle and decide where you can make changes to prevent hypertension. Achieve small goals, like snacking on fruits and vegetables instead of junk food, and continue to practice these healthy habits until they become part of your daily life.
Blood pressure and sweets: which foods and in what quantities are allowed?
Even despite the fact that in case of hypertension, sweets increase blood pressure, certain foods are still allowed because they bring many benefits with almost no harm. These include the following sweets:
honey;- dried fruits;
- fresh berries;
- black chocolate.
These products contain a high concentration of microelements that are beneficial for the functioning of the heart and also help normalize blood pressure.
As for chocolate, you should give preference to dark bitter varieties. It is allowed to consume cocoa. In addition to the positive effect on the heart and blood vessels, they also successfully fight stress and improve mood, which is associated with their effect on the secretion of “joy hormones” - endorphins. You are allowed to eat no more than one slab of this dessert per week.
Honey has a huge amount of useful vitamins and microelements, especially potassium. Instead of glucose, it contains fructose, so it can be consumed even by diabetics. It is recommended to eat 2 spoons per day.
Dried fruits and berries, in addition to providing the need for sugar, minerals and vitamins, also have a pronounced diuretic effect, which is important for hypertension, reducing the patient’s need for antihypertensive pills. It is very good to use them together with cinnamon, which also lowers blood pressure.
As for hypotension, almost any sweetness will increase blood pressure. But don’t be overzealous - too much sugar will negatively affect the health of hypotensive people, including. It is better to consume natural products such as honey or dried fruits.
How does sweet tea affect blood pressure?
Our usual tea has a fairly strong effect on blood pressure. It contains a significant amount of caffeine, which has a pronounced hypertensive and general tonic effect, and can cause rapid heartbeat and other arrhythmias. In addition, it contains tannin, which has a similar effect. Green tea contains even more of these components than black tea, which must be taken into account when consuming.
Most people are accustomed to drinking tea with sugar, which, of course, only increases the hypertensive effect of the drink, making it effective in hypotensive patients, especially during crises.
Treatment with medications
If you have diabetes, the use of antihypertensive therapy is recommended in cases where blood pressure remains at 140/80 mmHg. even when adjusting your lifestyle through diet, exercise, etc. Target blood pressure is below 130/80 mm Hg. Art. is mandatory if the patient has complications such as damage to the retina, kidney (nephropathy) or brain tissue (stroke).
There are several different medications that can lower blood pressure readings. The choice depends on things like:
- Do you have other health problems?
- Are you taking other medications?
- Possible side effects of the medicine.
- Patient's age and ethnicity.
The first group of drugs that is most often used is a drug called an angiotensin-converting enzyme (ACE) inhibitor. ACE inhibitors protect against kidney damage and also help control blood pressure.
One drug lowers blood pressure to target less than half the time. Therefore, this means that two or more different medications are usually required to achieve the target level (140/80 mmHg or below). In about a third of cases, three or more medications are needed to lower blood pressure to target levels. Therefore, patients with a combination of diabetes mellitus and arterial hypertension need regular consultations with doctors to monitor their health status and adjust treatment.
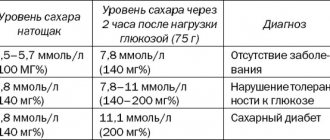
Diagnosis of diabetes mellitus
The following methods and tests have been established for diagnosing diabetes mellitus:
- measuring blood glucose levels (determination of glycemia);
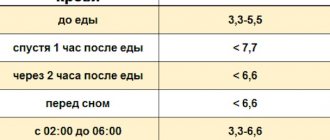
- measurement of daily fluctuations in glycemic levels (glycemic profile);
- measuring insulin levels in the blood;
- glucose tolerance test;
- blood test for the concentration of glycosylated hemoglobin;
- blood chemistry;
- urine test to determine white blood cell, glucose and protein levels;
- Ultrasound of the abdominal organs;
- Rehberg's test.
In addition, if necessary, carry out:
- study of blood electrolyte composition;
- urine test to determine the presence of acetone;
- fundus examination;
- electrocardiography (ECG).