Learn more about diseases starting with the letter “P”: Panic attacks; Duchenne-Erb's palsy; Todd's palsy; Parasomnias; Paroxysmal hemicrania; Paroxysmal myoplegia, Paroxysmal positional vertigo; Peripheral autonomic failure; Hepatic encephalopathy; Pineoblastoma; Pineocytoma; Writer's cramp; Platybasia; Plexites; Brachial plexitis; Humeroscapular periarthrosis; Pneumococcal meningitis Pneumocephalus; Subacute sclerosing panencephalitis; Spinal cord injury.
Hepatic encephalopathy is, without exaggeration, the most dangerous complication accompanying liver disease. The essence of the disease is damage to the nervous system by toxic substances. The first signs of encephalopathy are:
- personality changes;
- deterioration of intellectual abilities;
- mood and mental disorders;
- disturbances in the functioning of the endocrine glands.
The main diagnostic methods for detecting pathology are: hardware diagnostic methods (MRI, CT, ultrasound) and laboratory diagnostics (various blood tests, biochemical studies of affected tissues).
Total information
Liver pathology is extremely rarely complicated by hepatic encephalopathy. However, if the disease is nevertheless detected, its outcome is almost always tragic: for 2/3 of those affected, encephalopathy ends in death. Chronic liver diseases are more often complicated by hepatic encephalopathy than acute ones. They are potentially reversible, but significantly affect the patient’s ability to work and lifestyle.
Modern medical science does not yet have a clear idea of the causes of the development of the disease, but recent research allows us to hope for a solution to this problem in the near future. Discovering the mechanisms of the disease will contribute to the development of an effective treatment plan that will not only reduce the number of deaths, but will significantly improve the quality of life of those affected.
Our specialists
Tarasova Svetlana Vitalievna
Expert No. 1 in the treatment of headaches and migraines. Head of the Center for the Treatment of Pain and Multiple Sclerosis.
Somnologist.
Epileptologist. Botulinum therapist. The doctor is a neurologist of the highest category. Physiotherapist. Doctor of Medical Sciences.
Experience: 23 years.Derevianko Leonid Sergeevich
Head of the Center for Diagnostics and Treatment of Sleep Disorders.
The doctor is a neurologist of the highest category. Vertebrologist. Somnologist. Epileptologist. Botulinum therapist. Physiotherapist. Experience: 23 years.
Bezgina Elena Vladimirovna
The doctor is a neurologist of the highest category. Botulinum therapist. Physiotherapist. Experience: 24 years.
Dyachenko Ksenia Vasilievna
Head of the center for the treatment of dizziness and balance disorders.
The doctor is a neurologist of the highest category.
Angioneurologist. Neurorehabilitation specialist. Physiotherapist. Candidate of Medical Sciences.
Experience: 19 years.Drozdova Lyubov Vladimirovna
The doctor is a neurologist. Vertebroneurologist. Ozone therapist. Physiotherapist. Experience: 17 years.
Zhuravleva Nadezhda Vladimirovna
Head of the center for diagnosis and treatment of myasthenia gravis.
The doctor is a neurologist of the highest category. Physiotherapist. Experience: 16 years.
Palagin Maxim Anatolievich
The doctor is a neurologist. Somnologist. Epileptologist. Botulinum therapist. Physiotherapist. Experience: 6 years.
Causes of pathology
The appearance of encephalopathy can be provoked by:
- acute liver disease;
- entry of neurotoxins into the circulatory system;
- cirrhosis of the liver.
Factors contributing to the development of the disease: hepatitis of all types (alcoholic, fatty, toxic, viral), oncology, drug or toxic intoxication, other diseases accompanied by hepatocytolysis.
An excessive increase in the microflora of the obligate intestine or the consumption of excess amounts of protein-rich food can trigger the entry of intestinal neurotoxins into the circulatory system. Liver cirrhosis, complicated by hepatic encephalopathy, is accompanied by the formation of scars (replacement of healthy liver tissue with connective tissue), inhibition of all basic liver functions.
The following factors can provoke the death of hepatocytes and toxic damage to brain cells:
- internal bleeding;
- taking hepatotoxic drugs (without medical supervision and adequate supportive therapy);
- constipation, protein dyspepsia;
- surgical interventions or serious injuries;
- peritonitis provoked by ascites;
- bacterial, viral diseases.
Liver failure is accompanied by a list of pathological changes:
- disturbance of homeostasis, CBS;
- changes in oncotic and hydrostatic pressure.
These changes significantly disrupt the normal functioning of astrocyte cells, which account for approximately a third of the weight of brain tissue. Astrocytes are responsible for the normal regulation of the permeability of the cellular barrier, which ensures complete exchange between brain tissues and blood, removing toxins and ensuring the supply of nutrients to brain cells.
In addition to ammonia, toxic damage to astrocytes can cause exposure to false neurotransmitters, magnesium, as well as breakdown products of protein and fatty acids.
Symptoms of the disease
In the clinical picture of the disease, two types of disorders are distinguished: neurological and mental.
These include:
- disorders of consciousness;
- changes in the sleep cycle (severe drowsiness occurs during the daytime, and insomnia occurs at night);
- behavioral deviations (sharp changes in mood, causeless apathy, indifference and detachment);
- intellectual disorders (forgetfulness, confusion of thoughts, impaired fine motor skills, writing and memory);
- lack of emotional coloring of speech.
In addition, due to disturbances in the liver, the smell of acetone from the mouth may appear. Its appearance is due to the fact that the body, trying in every way to get rid of decay products, removes them using the respiratory system.
In some cases, the presence of liver failure can be judged by the appearance of asterixis - asymmetrical sweeping arrhythmic muscle twitching that occurs in the neck and limbs after their tonic tension. In some cases, encephalopathy affects the part of the brain responsible for regulating body temperature, which can cause a sudden change in temperature.
Based on the speed of onset of symptoms, the disease is divided into acute and chronic forms. The acute form develops lightning fast and quickly, and can lead to a coma. The chronic form develops gradually over time.
In its development, the disease sequentially goes through several stages:
- The first stage is subcompensation. This stage is characterized by the development of the disease, mental changes occur (apathy, sleep disturbances and sudden changes in mood), accompanied by lesions of the skin and mucous membranes.
- The second stage is decompensation. At this stage, mental disorders worsen, the patient becomes irritable and aggressive. Fainting and inappropriate behavior may occur.
- The third stage is terminal. It is accompanied by depression of consciousness up to a state of complete detachment, but the reaction to the stimulus (especially painful ones) may persist.
- The fourth stage is coma, characterized by a complete lack of response to stimuli, convulsions appear. At this stage, one patient out of 100 survives.
Hepatic encephalopathy: symptoms, diagnosis, treatment
World Congress of Gastroenterologists
The following nomenclature, proposed by the World Congress of Gastroenterology, is used more often by gastroenterologists than by critical care physicians:
- Type A. Encephalopathy associated with acute liver failure
- Type B. Encephalopathy associated with portosystemic shunting, but there is no disease that directly affects the liver cells
- Type B. Encephalopathy associated with cirrhosis and portal hypertension or systemic shunt Episodic PE (provoked, spontaneous or recurrent)
- Chronic PE (mild, severe, or treatment-induced)
- Minimum PE.
Diagnostics
This disease is a diagnosis of exclusion and its manifestations are difficult to distinguish. A high suspicion of HE as a possible diagnosis should be reserved for any patient presenting with acute or chronic liver dysfunction. In patients with chronic liver disease, precipitating factors that can cause the development of HE include, but are not limited to, hypovolemia, gastrointestinal bleeding, hypokalemia, metabolic alkalosis, hypoxia, the use of sedatives, hypoglycemia, infection or thrombosis of the hepatic or portal vein.
Patients with acute liver failure have a sharp deterioration in liver function, and they may also develop coagulopathy. A thorough history should be obtained, particularly regarding possible exposures to viral infections, drugs (paracetamol overdose is the most common cause), and toxins. Patients with previously diagnosed liver disease should also be asked whether they have had previous episodes of PE. It is also important to exclude other causes of changes in mental status. These include infection, deviations in the concentration of electrolytes (sodium, calcium, potassium), as well as glucose, hypoxemia, uremia, contact with toxins (alcohol or sedatives), primary disorders of the central nervous system, in particular, bleeding or infection.
Anamnesis
If possible, a complete history should be obtained to determine if there is a precipitating factor or other cause for the change in mental status. It may be necessary to obtain additional medical history from a relative or friend.
Patients may describe symptoms associated with a mild neurological disorder, such as sleep disturbances (insomnia or hypersomnia), euphoria or depression, and motor disturbances, such as asterixis (“fluttering” tremors) and ataxia. More progressive neurological disorders manifest as drowsiness followed by loss of consciousness or coma.
Survey
A complete physical examination should be performed to look for signs of precipitating factors and other causes of changes in mental status. Physical examination findings in cirrhosis include jaundice, ascites, palmar erythema, edema, and telangiectasia. In the early stages of viral hepatitis, liver enlargement may occur. Jaundice may or may not be present. Reflexes may be impaired and nystagmus may develop. In a group of similar cases, 17% of patients had focal disorders, among which hemiplegia was most often recorded.
Priority tests
It is necessary to determine the level of electrolytes, FPP, renal panel, CBC, bacteriological examination, coagulation panel, urinalysis, screening for toxins.
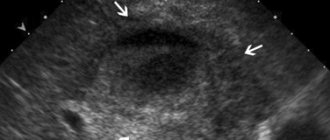
Chest X-ray and CT scan of the head will help narrow the differential diagnostic search, namely, if other abnormalities are present, then other diagnoses can be discarded. Although CT or MRI of the head may reveal cerebral edema, these changes are not sensitive or specific for HE. Ultrasound examination of the upper abdomen should be considered in all patients with acute decompensation without an adequate cause, as acute portal or hepatic vein thrombosis may be the cause.
Psychometric testing can be performed to assess latent or early-onset HE, but this method is not recommended for all patients. The PE Psychometric Scale is a combination of 5 pen-and-paper tests that can be completed at a hospital bedside within 20 minutes. These tests are recommended by the World Congress of Gastroenterology (1998) and the International Society on Hepatic Encephalopathy and Nitrogen Metabolism, which include the Digit Link Test and the Digit Symbol Test.
Other examinations
Results from measuring ammonia concentrations are controversial—very low or very high concentrations may be significant in the appropriate clinical context. Monitoring the direction of changes in ammonia levels may be useful to monitor therapy but is not necessary to establish a diagnosis.
EEG may be useful in diagnosing mild PE and also in excluding occult seizure activity in comatose patients. HE may be associated with a decrease in the frequency and amplitude of brain waves. In patients with ascites, diagnostic paracentesis should also be performed to rule out spontaneous bacterial peritonitis, which may cause PE.
Differential diagnosis
| Disease | Differential signs/symptoms | Differential examinations |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Diagnostic criteria
West Haven Criteria
These criteria are based on the severity of the disease
- Degree 0. Normal
- Degree I. Mild disturbance: changes in sleep, somewhat weakened intellectual function, increased irritability, metabolic tremor, impaired muscle coordination
- Degree II. Moderate impairment: lethargy, significant impairment of intellectual function, disorientation in time, inappropriate or extravagant behavior, slurred speech, hypoactive reflexes, ataxia
- Degree III. Severe: drowsiness, confusion, paranoia or anger, hyperactive reflexes, nystagmus, Babinski reflex, clonus
- Degree IV. Coma: loss of consciousness, dilated pupils.
Treatment
The primary goals of treatment are to provide supportive care, identify and correct precipitating factors, reduce gastrointestinal nitrogen load, and assess the need for long-term therapy.
Symptomatic therapy
This includes regular monitoring of the patient’s neurological and mental state. Comatose patients should be transferred to the intensive care unit, and endotracheal intubation should be considered if airway compromise is present. Patients with significant cerebral edema may require monitoring of intracranial pressure. If PE is accompanied by acute liver failure, then careful monitoring of serum glucose levels and prothrombin time is necessary.
Identification and correction of provoking factors
If precipitating factors are identified during the history and physical examination, they should be eliminated. These include gastrointestinal bleeding, infection, electrolyte abnormalities, renal failure, anti-anxiety or narcotic use, excessive protein intake, acute hepatic or portal vein thrombosis, and recent placement of a transjugular portosystemic liver shunt (TPHS). Ultrasound may help identify hepatic or portal vein thrombosis, or hepatocellular carcinoma. Sometimes it is necessary to occlude the shunt if it is impossible to treat the patient otherwise.
Reducing nitrogen load
It is hypothesized that restricting dietary protein may reduce intestinal ammonia production but may worsen pre-existing protein-energy malnutrition in patients with cirrhosis. One randomized controlled clinical trial found no difference between moderate and severe protein restriction. In fact, in a second randomized controlled clinical trial, a normal protein diet was not associated with an increased risk of PE when compared with a low protein diet. Despite this, the 2001 clinical practice guidelines advise limiting dietary protein intake for the treatment of acute PE. Protein elimination can be introduced from day one, gradually increasing the amount up to 1.2 g protein/kg/day. For patients with cirrhosis, no benefit has been established for administering nutrients parenterally.
Nitrogen loads from the digestive system can be reduced by using disaccharides and antibiotics that are not absorbed in the intestine. Decontamination of microorganisms also helps reduce the amount of ammonia, and therefore the level of ammonia in the blood.
Although the use of disaccharides, which are not absorbed in the intestine, is the mainstay of treatment, the exact mechanism of action of these drugs, in particular lactulose (a laxative), is not fully understood. Lactulose is broken down by intestinal bacteria into lactic acid and other organic acids. Oxidation in the intestinal lumen promotes the conversion of ammonium ions into ammonia, and consequently, the further release of ammonia from the tissues into the intestinal lumen. Oxidation also inhibits coliform bacteria that produce ammonia. Side effects, in particular diarrhea, abdominal discomfort, and bloating, limit the use of drugs. Data from randomized controlled clinical trials indicating their effectiveness are limited. Meta-analyses have concluded that lactulose improves PE and is also likely to reduce mortality, although this latter benefit was not observed when high-quality clinical trials were considered or when a lower relative risk reduction was used.
Interestingly, polyethylene glycol has been studied for the treatment of acute PE, which provides a laxative effect without intestinal oxidation. Despite the fact that the study did not include patients who received lactulose and rifaximin, that is, they were treated according to the usual regimen, the high effectiveness of treatment of acute HE with polyethylene glycol compared with lactulose monotherapy was shown.
The use of antibiotics is not straightforward. A 1997 study found neomycin to be as effective as lactulose, while another study found no difference between neomycin and placebo.
Ototoxicity and nephrotoxicity limit the long-term use of neomycin. Metronidazole is better tolerated by the body than neomycin, although with long-term use the possibility of developing peripheral neuropathy should be taken into account. Oral vancomycin and rifaximin were also used.
However, it should be noted that the European Medicines Agency found that the evidence does not adequately support the use of oral vancomycin for gastrointestinal decontamination in immunocompromised patients and does not recommend its use for these purposes.
A meta-analysis of comparative randomized controlled clinical trials indicates that rifaximin has no greater benefit than disaccharides that are not absorbed in the intestine in the treatment of episodic or persistent PE. However, as a result of the second meta-analysis, it was revealed that rifaximin leads to an improvement in the electroencephalogram response and the degree of portosystemic encephalopathy compared to disaccharides that are not absorbed.
Both meta-analyses indicated that rifaximin was better tolerated. In one retrospective clinical study of 145 patients treated for PE, only 31% of patients reported taking more than 75% of prescribed lactulose doses, whereas 92% of patients reported taking more than 75% of prescribed rifaximin doses.
A second meta-analysis of randomized controlled clinical trials comparing rifaximin with other oral agents indicates that rifaximin may be associated with a statistically non-significant trend toward normalization of blood ammonia and mental status compared with disaccharides or antibiotics, as well as a significant improvement in EEG and psychometric measures. characteristics.
The drug's safety profile, particularly in relation to diarrhea, also favors rifaximin over disaccharides or other antibiotics. As a side note, two randomized controlled clinical trials found that rifaximin was associated with improved health-related quality of life. However, both studies compared the effects of rifaximin with placebo, which limits the interpretation of these results in relation to other oral drugs.
Treatment with rifaximin was found to achieve remission of PE compared with placebo, and also reduce the risk of hospitalization for PE. Although early data on the concomitant use of rifaximin and lactulose did not indicate a benefit, a recent randomized controlled clinical trial examining the effects of lactulose and rifaximin compared with lactulose and placebo found significant benefits on the course of PE and length of hospital stay. , as well as mortality. Although these data are encouraging, caution should be exercised when introducing combination therapy as standard of care given the overwhelming number of patients with poor prognosis (Child-Turcotte-Pugh grade C) and the markedly increased mortality rate at 10 days in control group.
L-ornithine-L-aspartate
Stimulation of periportal glutamine synthesis in hepatocytes with the formation of ornithine and aspartate promotes the removal of ammonia. As a result, L-ornithine-L-aspartate (LOLA) is gaining attention and is being considered as an adjunctive therapy for PE. Two different meta-analyses of randomized controlled clinical trials comparing LOLA with placebo in the treatment of PE found that LOLA had a significant effect on improving the course of PE.
A third meta-analysis found that LOLA significantly improved blood ammonia levels and time to complete the Digit Link Test A. Despite this, when the fourth meta-analysis conducted to examine this issue found evidence to support blood ammonia reduction with LOLA, the authors note that clinical endpoints (eg, neuropsychological testing) were not assessed, which limits interpretation clinical significance.
Another meta-analysis comparing LOLA therapy with rifaximin, a non-absorbed disaccharide, neomycin, and branched-chain amino acids, showed a trend toward greater clinical efficacy of LOLA treatment, although the rate remained statistically nonsignificant. In addition, there is a lack of comparative data between LOLA and lactulose therapy in the treatment of PE. Only one clinical study showed that there was no difference between the two drugs.
Branched chain amino acids
Levels of essential branched chain amino acids (BCAAs) leucine, isoleucine, and valine are usually low in patients with cirrhosis. Because BCAAs play a role in brain signaling, their use in the treatment of PE is being explored. A meta-analysis of 16 studies of the use of BCAA in the treatment of PE found an improvement in PE compared with placebo or diet, but there were significant side effects of nausea or diarrhea.
However, when comparing BCAA with neomycin or lactulose, no effect on PE was observed.
Long-term treatment
Patients with chronic liver disease need help to prevent episodes of relapse of the disease. This includes avoiding the use of psychoactive drugs if possible, preventing spontaneous bacterial peritonitis if indicated, avoiding constipation, and preventing gastrointestinal bleeding. The development of HE has a poor prognosis, and selected patients should be referred to liver transplant centers after the first episode of encephalopathy. The most common prognostic model for assessing disease severity and selection for liver transplantation is the end-stage liver disease (ESLD) model. A score ≥15 is an appropriate indicator to consider transplantation.
Prophylactic treatment with lactulose has been shown to be effective in preventing recurrence of PE in patients with cirrhosis. Lactulose should be given continuously to patients (who tolerate it well) with cirrhosis/portal hypertension and pre- or recurrent episodes of PE. One randomized controlled clinical trial indicated that probiotic treatment may also be effective in preventing recurrence of PE, but further research is required.
Diagnosis of the disease
The main goal of diagnosis is to identify characteristic symptoms, determine the severity of the lesion and the stage of development of the disease. A detailed medical history can play a huge role (it is important to find out whether the patient has previously suffered from hepatitis, abused alcohol or taken uncontrolled medications).
A consultation with a gastroenterologist should be carried out in the early stages of the disease. It is very important that the gastroenterologist pays attention to symptoms of a neurological and psychological nature. Identification of symptoms of brain tissue damage in a patient in a comatose state indicates the possibility of an imminent death.
To confirm the diagnosis, the following laboratory diagnostic methods are used:
- blood test (diagnoses anemia, inhibition of platelet production, leukocytosis);
- coagulogram (detects coagulopathy, after development, which is DIC syndrome);
- liver tests (an increase in all markers characterizing the condition of the liver is noted, without exception).
If necessary, diagnostic methods are used to identify lesions in other organs and systems of the body.
To determine the extent of damage to the liver and other internal organs, hardware diagnostic methods such as ultrasound, MRI and CT are used. If encephalopathy is suspected, a biopsy of liver tissue is required (allows us to find out the cause of the disease). Electroencephalography is used to assess the condition of brain tissue.
Therapy
Therapy for this disease is a complex process that requires as quickly as possible clarification of the causes of its occurrence. The course of treatment includes: diet therapy, bowel cleansing, lowering nitrogen levels and symptomatic therapy.
It is necessary to reduce the amount of protein coming from food. It is necessary to adhere to this diet for a long time, since an increase in the amount of protein in the diet of a cured patient can provoke a relapse of the disease.
To speed up the excretion of ammonia in feces, it is necessary to achieve at least two bowel movements per day. For this purpose, cleansing enemas are used.
Antibacterial therapy involves taking antimicrobial drugs, the action of which is especially effective in the intestinal lumen (vancomycin, metronidazole, neomycin).
To achieve a sedative effect, benzodiazepine drugs are used, with preference given to haloperidol.
Forecast and prevention of the disease
The prognosis for the development of the disease, although it depends on a whole range of factors, is almost always negative. The survival rate of patients is higher if the disease develops against the background of chronic liver pathologies. In cirrhosis, the prognosis is seriously worsened in the presence of jaundice and ascites.
In acute liver failure, the prognosis for the development of the disease worsens in children under 10 years of age and adults after 40 years of age due to viral infection. The mortality rate in the first two stages reaches 30%, and in the last stages it exceeds 80%.
Prevention comes down to normalizing lifestyle, avoiding excessive use of medications and timely treatment of diseases that provoke the development of encephalopathy.
Due to the fact that the lethality of the disease directly depends on the stage of its development, timely detection of the disease is of great importance. To do this, it is important, at the slightest suspicion of the presence of the disease, to seek advice from a specialist, as well as to do a CT and MRI. You can undergo diagnostics at one of the clinics located in the service database. The site has collected information about hundreds of diagnostic clinics. A consultant is ready to help you choose a clinic over the phone and make an appointment for a convenient date.
Clinical picture
Currently, there are three clinical variants of PE [2, 3]:
1. Subclinical encephalopathy
Subclinical PE is characterized by the absence of clinical symptoms, but additional studies reveal a number of neuropsychic disorders (deterioration of cognitive abilities, loss of fine motor skills, which can only be determined using psychometric tests). According to the literature, in patients with cirrhosis, subclinical PE is detected in 50–70% of cases. In patients with cirrhosis with portosystemic shunting, PE can be episodic with spontaneous resolution or intermittent, lasting many months or even years.
2. Chronic encephalopathy
This form of PE is divided into three stages (Table 2). In stage I, subtle personality changes, absent-mindedness, decreased attention, inability to concentrate, mild ataxia, and sleep disturbances are clinically observed.
Stage II is manifested by fatigue, drowsiness, apathy, monotonous speech, inappropriate behavior with noticeable changes in the “structure” of the personality, disturbances in time orientation, the presence of intention tremor, reflexes of oral automatism, and ataxia.
Stage III PE is characterized by severe disorientation in time and space, incoherent speech, aggression, hypo- or hyperreflexia, pathological reflexes (Gordon, Zhukovsky), pronounced intention tremor, and muscle rigidity. With inadequate treatment of PE, hepatic coma may occur, which is characterized by a lack of consciousness and disappearance of reactions to painful stimuli. Rigidity of the muscles of the limbs and the back of the head, a mask-like face, and pathological reflexes (Babinsky, Gordon, Zhukovsky) are noted. Sometimes grasping and proboscis reflexes are detected [5].
In addition to psychoneurological symptoms, coma is characterized by clinical manifestations of hepatic cellular failure - jaundice, liver odor, ascites, hemorrhagic symptoms. The causes of death are cerebral edema, pulmonary edema, hepatorenal syndrome, infectious-toxic or hypovolemic shock.
3. Acute PE
It can develop in patients with severe jaundice against the background of ascites with severe necrotic processes in the liver, as well as in patients with fulminant liver failure. Acute HE may be accompanied by the development of hepatic coma.