Blood pressure fluctuates throughout the day and increases slightly when a person wakes up. However, many people may have high blood pressure in the morning. Doctors call it morning hypertension
. Morning hypertension increases the risk of heart attack and stroke, which often occur in the early hours.
Several factors can affect blood pressure:
- stress or anxiety
- physical activity
- diet
Blood pressure readings are displayed as two numbers. The top number represents systolic, which reflects the pressure when the heart contracts. The bottom number shows diastolic, which is a measure of the pressure when the heart relaxes. Normal blood pressure is 120/80 mmHg. Art. Readings between 120/80 mmHg. and 139/89 mmHg. Art. indicate that a person is at risk of developing hypertension, and readings above 140/90 mmHg. Art. indicate hypertension.
Blood pressure rises and falls throughout the day and night. During sleep, blood pressure drops by 10-30%, then rises upon awakening. In some people, this increase can be significant, leading to morning hypertension.
As a 2010 study notes, strokes and heart attacks peak in the first 4 to 6 hours after waking up.
Why is blood pressure higher in the morning than in the evening?
The risk of morning hypertension increases:
- high cholesterol
- cardiovascular diseases
- obstructive sleep apnea
- diabetes
- thyroid diseases
- Cushing's syndrome
- lupus
- scleroderma
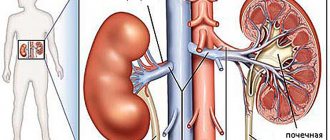
- kidney disease
Certain lifestyle factors also increase the risk of developing hypertension. Examples include:
- smoking
- alcohol consumption
- diet high in salt and saturated fat
- lack of sufficient physical activity.
Morning hypertension can be caused by the following factors:
- The dosage of the antihypertensive drug is too low
- taking short-acting and intermediate-acting drugs
- taking one antihypertensive drug rather than a combination of drugs
The medications can be taken before bed to provide better blood pressure control. You can also split the daily dose, taking half in the morning and half before bed. It is important to talk to your doctor before making any changes to your medications.
The influence of sleep disturbance on the course of arterial hypertension
For many decades, arterial hypertension (AH) has been the most pressing problem in cardiology and modern medicine. This is due to its wide distribution throughout the world, damage to target organs and subsequent persistent loss of performance, leading to huge socio-economic losses due to early disability of the population and high mortality. According to the latest recommendations for the diagnosis and treatment of arterial hypertension, the prevalence of hypertension is 43.4% [1]. At the same time, despite the simplicity and accessibility of hypertension treatment, effective blood pressure (BP) control is achieved by only 14.4% of men and 30.9% of women [2]. One of the reasons for this is that the etiology and pathogenetic mechanisms of essential hypertension still remain not fully understood. The multifactorial nature of the disease is due to complex mechanisms of interaction between environmental factors and the individual’s genotype, which determines the functioning of the renin-angiotensin-aldosterone, kallikrein-kinin and sympathoadrenal systems, and the vasodilating function of the endothelium.
It is known that it is the combination of genetic predisposition with cardiovascular risk factors, such as smoking, psycho-emotional stress, excessive alcohol consumption, abdominal obesity, physical inactivity, and excessive consumption of table salt, that leads to the development of hypertension [3].
Currently, hypertension is one of the diseases that can be effectively controlled. Even a slight decrease in blood pressure reduces target organ damage. A study of controlled trials that focused on the effectiveness of antihypertensive therapy made it possible to track a reduction in the risk of myocardial infarction by 22% and stroke by 41% with a decrease in systolic blood pressure by 10 mmHg. Art. and diastolic blood pressure by 5 mm Hg. Art. [4]. According to the results of studies conducted by S. Lewington et al. (2002), it was found that with effective treatment of hypertension, mortality from cardiovascular diseases is reduced by 15–20%, and disease progression will occur 10–12 times less often among patients taking antihypertensive drugs than among patients who did not take these drugs drugs [5].
The problem of sleep disturbance (insomnia) is also widespread in the population. Sleep is one of the main factors modulating the functional state of the cardiovascular system, both in normal and pathological conditions [6]. It is a heterogeneous process consisting of successive functional states of the brain, including the slow-wave sleep phase, the so-called dreamless sleep, and the rapid sleep phase, sleep with dreams [7].
Normal sleep is sleep consisting of four or six wave-like cycles, lasting about 90 minutes. It significantly affects the autonomic nervous system and hemodynamics [8]. It is known that insomnia leads to deterioration of memory, attention, decreased performance, and contributes to frequent headaches and irritability. Chronic stress, anxiety, and somatic diseases are triggers for the formation of sleep disorders. Rare attendance leads to the fact that no more than a quarter of patients receive treatment for insomnia [9]. Therapeutic tactics for this pathology may include eliminating the cause of sleep disorders, being an etiological method of therapy. Changing sleep duration and structure without addressing the cause is a symptomatic approach [10].
The history of the study of sleep physiology is quite extensive. It is known that insomnia is nothing more than a “failure” of circadian rhythms and a disruption in the interaction of various endogenous and exogenous factors with each other [11].
The hypothalamus and pineal gland support the ri. Light pulses affecting the ganglion cells of the retina have a stimulating effect on the suprachiasmatic nuclei of the hypothalamus through the retinohypothalamic tract. The suprachiasmatic nuclei of the hypothalamus influence the pineal gland, which synthesizes melatonin, which is produced in the dark (from 20–22 o'clock the level of melatonin begins to increase, reaching its maximum between 2 and 4 o'clock in the morning), and inhibited during daylight hours (with the onset of morning the level of melatonin gradually decreases) [12]. In turn, the interaction of melatonin with specific receptors on neurons in the cerebral cortex induces sleep. Thus, the mechanisms of action of melatonin on the body and the effects associated with it are a very relevant topic today.
At night, blood pressure numbers are significantly lower compared to the waking period, which is most likely due to the regulatory effect of melatonin. There are many clinical trials demonstrating the antihypertensive effect of melatonin in patients with initially high blood pressure [13]. However, it has not been proven that a hereditary predisposition to insufficient melatonin production is one of the factors leading to increased blood pressure levels.
There is also a large number of studies examining the effect of poor sleep quality on increases in both nighttime and daytime BP levels. It has been proven that the correction of sleep disturbances in hypertension with melatonin contributed to both improved sleep and a decrease in blood pressure [14, 15].
R. Robillard et al. (2011) in their study showed that sleep disturbance entails an increase in both systolic blood pressure and diastolic blood pressure in normotensive people, which led to the conclusion that lack of sleep changes the mechanisms of blood pressure regulation and increases the risk of developing hypertension in healthy people c normal blood pressure values [16].
In a study by M. Jonas et al. (2013) described a direct connection between the lack of adequate reduction in blood pressure during sleep and a decrease in melatonin secretion. Based on the results obtained, the authors concluded that melatonin plays an important role in the regulation of circadian blood pressure rhythms in patients with hypertension [17]. This effect of melatonin is associated with its ability to reduce the secretion of gonadotropins and hormones of the adenohypophysis, increasing the content of gamma-aminobutyric acid and serotonin in the midbrain and hypothalamus, which leads to the normalization of circadian rhythms, the biological change of sleep and wakefulness [12].
The effect of melatonin on the regulation of circadian blood pressure rhythm was shown in a small study by E. Grossman et al. (2016), which included 38 patients who received antihypertensive therapy but had elevated blood pressure during sleep. Two groups were formed: patients in the first, experimental group received sustained-release melatonin before bedtime, and patients in the control group received placebo. At the end of the study, a significant decrease in blood pressure during sleep was established in the experimental group (systolic - from 136 ± 9 to 130 ± 10 mm Hg (p = 0.011), and diastolic - from 72 ± 11 to 69 ± 9 mm Hg . (p = 0.01)). In the control group of patients, the level of nighttime blood pressure remained unchanged [18]. Also P. Lemoine et al. (2012) in a study that included 791 patients in the age group from 18 to 80 years old, noted the ability of melatonin to reduce the period of falling asleep and increase the total duration of sleep. These effects were especially pronounced in patients over 55 years of age, with these effects increasing over six months of use. In addition, the effectiveness and safety of melatonin was noted when used together with antihypertensive, hypoglycemic and anti-inflammatory drugs, especially in elderly and middle-aged people with hypertension [19].
Academician A.I. Martynov et al. (2002) found that elderly patients with various sleep disorders are 5 times more likely to have elevated blood pressure at night. In addition, patients in whom it was impossible to achieve normalization of nocturnal BP, despite taking antihypertensive drugs, had significantly worse sleep indicators compared to patients with normal BP values during sleep [20].
In addition, A. Brzezinski et al. (2015), having conducted a meta-analysis of 17 different studies, concluded that melatonin in elderly patients is effective as a drug for normalizing sleep quality and helps reduce the time to fall asleep; in addition, its positive effect on nocturnal hypertension was noted [21].
This is of great importance in connection with the facts obtained by T. Ohkubo et al. (2010). They noted that if the degree of reduction in blood pressure during sleep is only 5%, then the risk of cardiovascular mortality increases by approximately 20%. The study, conducted in Dublin over 8 years, involved more than 5 thousand patients with hypertension. The authors noted that an increase in nighttime blood pressure by 10 mm Hg. Art. led to a 21% increase in mortality and a higher incidence of cardiovascular complications. Thus, lowering blood pressure during sleep reduces the risk of occurrence and progression of cardiovascular complications [22].
In addition, many authors have become interested in the existing relationship between sleep duration and the risk of occurrence and progression of hypertension. J. Fernandez-Mendoza et al. (2012) demonstrated the relationship between insomnia and an increased risk of hypertension associated with a shortened sleep duration of less than 6 hours [23].
Gottlieb et al. (2006) in their Sleep Heart Health Study (SHHS) of people aged 45 to 69 years demonstrated an association of sleep duration with the occurrence of hypertension. It was found that short sleep duration contributes to the occurrence of hypertension compared with people whose sleep was 7-8 hours per night. A high incidence of hypertension over 8–10 years was also shown in the Korean National Health and Nutrition Survey (NHNES), in which participants slept less than 5 hours. In addition, a relationship was found between age and gender with sleep duration and hypertension. In the NHNES study, the association between sleep restriction and the incidence of hypertension was found to be greater in women aged 60–86 years [24].
D. Yadav et al. studied a similar problem. (2017). From November 2005 to January 2011, they conducted a study including 1715 participants who did not suffer from hypertension. Participants underwent a comprehensive medical examination at baseline and follow-up. Sleep duration was assessed using a questionnaire, according to the results of which all participants were divided into four groups depending on the duration of sleep: the first group consisted of people whose sleep was less than 6 hours; the second group - sleep from 6 to 7.9 hours; the third group - sleep from 8 to 9.9 hours; and the fourth group - sleep 10 hours or more. At the end of the study, it was found that people who slept less than 6 hours were at high risk of developing hypertension, with hypertension occurring after approximately 2.6 years. In the study subjects whose sleep ranged from 8 to 9.9 hours and more than 10 hours, no increase in blood pressure was recorded [25].
The results of a meta-analysis of cross-sectional studies involving a large group of patients, published by G. Seravalle et al. (2018), indicate that short sleep duration more often causes hypertension and cardiovascular diseases [26].
C. J. Bathgate et al. (2018), summing up the results of their two-year study on insomnia and the risk of developing hypertension, concluded that the relationship between high blood pressure or stage 1 and 2 hypertension is stronger in patients with short sleep duration. The authors proposed including insomnia in the main list of factors for the development of hypertension [27].
A. Vgontzas et al. (2009) followed patients in Pennsylvania. The 1,741 participants were divided into several groups based on sleep duration (6 hours, 5 to 6 hours, and less than 5 hours). Based on the results of the observation, the authors concluded that patients who slept less than 5 hours had a high risk of hypertension, and the average risk of hypertension was in patients whose sleep ranged from 5 to 6 hours [27].
C. W. Kim et al. (2018) observed 106,385 patients who did not have hypertension or cardiovascular diseases at the time of inclusion in the study. Based on the monitoring results, the authors recorded 4750 cases of hypertension. Decreased sleep duration was associated with an increased risk of incident hypertension over the subsequent 2.4 years. Among patients at increased risk of hypertension, there were more women than men. The authors concluded that women with short sleep duration (less than 7 hours) are at greater risk of developing hypertension during the follow-up period [28].
A number of studies have shown that depression is often combined with insomnia, and this combination significantly increases the risk of developing cardiovascular diseases and hypertension. The most striking results are the work of Gangwisch et al. (2010), which examined the possible influence of depression and insomnia on the risk of hypertension. Insomnia and short sleep duration were the main symptoms of depression, contributing to the occurrence of hypertension and increasing the risk of developing cardiovascular diseases. In all middle-aged patients suffering from depression and having short sleep duration and insomnia, the development of hypertension was observed 44% more often. The authors concluded that treating sleep problems in depressed middle-aged adults may reduce the risk of hypertension and cardiovascular complications [29].
Thus, the above research results clearly demonstrate the relationship between sleep disturbance and an increased risk of developing hypertension. However, it is impossible to unambiguously answer the question of what leads to hypertension: short sleep duration or insufficient melatonin production. These questions require further study, and obtaining answers to them may serve as one of the promising directions in the fight against cardiovascular diseases.
Literature
- Chazova I. E., Zhernakova Yu. V. Recommendations for the diagnosis and treatment of arterial hypertension 2021, the word is up to European experts // Systemic hypertension. 2021. Vol. 15, No. 3. pp. 6–10.
- Boytsov S. A., Balanova Yu. A., Shalnova S. A. et al. Arterial hypertension among persons 25–64 years old: prevalence, awareness, treatment and control. Based on materials from the ESSE study // Cardiovascular therapy and prevention. 2014. T. 13, no. 4. pp. 4–14.
- Kharchenko E. P. Arterial hypertension: an expanding pathogenetic continuum and therapeutic limitations // Therapeutic archive. 2015. No. 1. P. 100–104.
- Law MR, Morris JK, Wald NJ Use of blood pressure lowering drugs in the prevention of cardiovascular disease: meta-analysis of 147 randomized trials in the context of expectations from prospective epidemiological studies // BMJ. 2009. P. 1338–1665.
- Lewington S., Clarke R., Qizilbash N., Peto R., Collins R. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies // Lancet. 2002. Vol. 360. P. 1903–1913.
- Savelyeva Yu. K., Osetrina D. A., Volsky V. V. The meaning of sleep and its physiology // Student Forum. 2021. T. 11–1, No. 32. P. 21–24.
- Chertsova A.I., Prokopenko L.A. Sleep and its duration // International student scientific bulletin. 2015. No. 5–4. pp. 599–600.
- Syrkin A.L., Palman A.D., Poluektov M.G. Sleep and arterial hypertension // Effective pharmacotherapy. 2013. No. 12. pp. 64–70.
- Ringdahl EN, Pereira SL, Delzell JE Diagnosis and treatment of primary insomnia // International Neurological Journal. 2008. No. 3. pp. 23–29.
- Prokhorova S.V., Maksimova T.N. Experience of using prolonged melatonin for the treatment of sleep disorders in depression // Neurology, neuropsychiatry, psychosomatics. 2015. T. 7, no. 3. pp. 46–50.
- Bragina T.V., Markov L.I. The role of circadian rhythms in the human body. In: Aspects of life safety and medicine. Materials of the international scientific and practical conference. 2021. pp. 15–19.
- Snezhitsky V. A., Pobivantseva N. F. Circadian rhythms in cardiological practice // Journal of the Grodno State Medical University. 2013. T. 41, No. 1. P. 9–13.
- Budnevsky A.V., Ovsyannikov E.S., Filina N.V. The role of melatonin in the pathogenesis of cardiovascular diseases // Cardiovascular therapy and prevention. 2021. No. 5. pp. 97–101.
- Lyubshina O.V., Maksimova M.Yu. Sleep disturbances in patients with arterial hypertension // Therapist. 2010. No. 5. P. 30–41.
- Budnevsky A.V., Ovsyannikov E.S., Rezova N.V. et al. Melatonin and arterial hypertension: a possible role in complex therapy // Therapeutic archive. 2021. Vol. 89, No. 12, pp. 122–126.
- Robillard RP, Lanfranchi PA, Prince F., Filipini D., Carrier J. Sleep deprivation increases blood pressure in healthy normotensive elderly and attenuates the blood pressure response to orthostatic challenge // Sleep. 2011. Vol. 34, No. 3. P. 335–339.
- Jonas M., Garfinkel D., Zisapel N. et al. Impaired nocturnal melatonin secretion in non-dipper hypertensive patients // Blood Press. 2013. Vol. 12, No. 1. P. 19–24.
- Grossman E., Laudon M., Zisapel N. Effect of melatonin on nocturnal blood pressure: meta-analysis of randomized controlled trials // Vasc. Health Risk Manag. 2011. Vol. 7. P. 577–584.
- Lemoine P., Wade AG, Katz A., Nir T. et al. Efficacy and safety of extended-release melatonin for insomnia in middle-aged and elderly patients with hypertension: a combined analysis of controlled clinical trials // Integr. Blood Press Control. 2012. Vol. 5. P. 9–17.
- Martynov A. I., Vein A. M., Ostroumova O. D. et al. The use of zopiclone for the correction of high blood pressure in the sleep-wake cycle in elderly patients with essential arterial hypertension and insomnia // Cardiology. 2002. No. 8. pp. 11–14.
- Brzezinski A., Vangel MG, Wurtman RJ et al. Effects of exogenous melatonin on sleep: a meta-analysis // Sleep Med. Rev. 2005. Vol. 9, No. 1. P. 41–50.
- Ohkubo T., Hozawa A., Nagai K. et al. Prediction of stroke by ambulatory blood pressure monitoring versus screening blood pressure measurements in a general population: the Ohasama study // J. Hypertens. 2000. Vol. 18. P. 847–854.
- Bathgate CJ, Fernandez-Mendoza J. Insomnia, Short Sleep Duration, and High Blood Pressure: Recent Evidence and Future Directions for the Prevention and Management of Hypertension // Curr Hypertens Rep. 2021. Vol. 20, No. 6. P. 52.
- Gottlieb DJ, Redline S, Nieto FJ et al. Association of usual sleep duration with hypertension: the Sleep Heart Health Study // Sleep. 2006. Vol. 29, No. 8. P. 1009–1014.
- Yadav D., Hyun D., Ahn S., Koh S., Kim J. Prospective study of the association between total sleep duration and incident hypertension // J Clin Hypertens (Greenwich). 2021. Vol. 19, No. 5. P. 550–557.
- Seravalle G., Mancia G., Grassi G. Sympathetic Nervous System, Sleep, and Hypertension // Curr Hypertens Rep. 2021. Vol. 20, No. 9. P. 74.
- Vgontzas A., Liao D., Bixler E., Chrousos GP, Vela-Bueno A. Insomnia with objective short sleep duration is associated with a high risk for hypertension // Sleep. 2009. Vol. 32, No. 4. P. 491–497.
- Kim C.W., Chang Y., Kang J., Ryu S. Changes in sleep duration and subsequent risk of hypertension in healthy adults // Sleep. 2018. Vol. 41, No. 11, 159.
- Gangwisch JE, Malaspina D., Posner K., Babiss LA, Heymsfield SB, Turner JB, Zammit GK, Pickering TG Insomnia and Sleep Duration as Mediators of the Relationship Between Depression and Hypertension Incidence // Am J Hypertens. 2010. Vol. 23, No. 1. P. 62–69.
A. V. Budnevsky1, Doctor of Medical Sciences E. S. Drobysheva, Candidate of Medical Sciences R. E. Tokmachev, Candidate of Medical Sciences N. V. Rezova
FSBEI HE VSMU named after. N. N. Burdenko Ministry of Health of Russia, Voronezh
1 Contact information
DOI: 10.26295/OS.2019.22.90.005
The influence of sleep disturbance on the course of arterial hypertension / A. V. Budnevsky, E. S. Drobysheva, R. E. Tokmachev, N. V. Rezova For citation: Attending physician No. 7/2019; Page numbers in issue: 28-30 Tags: blood pressure, insomnia, depression, cardiovascular complications
When and how should blood pressure be measured?
Regular use of a blood pressure monitor will help people monitor blood pressure fluctuations. This will help identify episodes of morning hypertension.
Before measuring blood pressure:
- Empty your bladder.
- Rest quietly and comfortably for 5 minutes before taking your blood pressure.
- Avoid smoking, drinking alcohol, or exercising for 30 minutes after taking your blood pressure.
Take your blood pressure at the same time every day.
- Sit with your back straight, legs uncrossed, and feet flat on the floor.
- Place your hand on a flat surface so that your shoulder is at heart level.
- Place the cuff on your arm so that the bottom of the cuff is directly above the elbow crease.
- Keep a record of your readings, this can help your doctor determine the optimal course of treatment.
What influences the increase in pressure
However, high blood pressure after sleep does not necessarily indicate pathology. It can be observed in an absolutely healthy person. There are several non-hazardous factors that affect the indicator in the morning. For example:
- The man ate something salty at night. After such food I really want to drink. Considering the fact that salt retains moisture in the body, the pressure of fluid on the walls of blood vessels increases. Consequently, the pressure rises in the morning.
- Severe fatigue, lack of proper rest, poor sleep. In the presence of all these factors, the brain is in an overexcited state. It forces all organs to work more intensely than usual. Blood circulates faster. This provokes pressure surges in the morning.
- Abuse of medications, or use of them without prescription from a specialist. This is very dangerous, because if taken incorrectly, side effects can occur. Including high blood pressure in the morning after sleep.
- The most harmless reason is a malfunction of the tonometer. If you feel excellent, but the device persistently shows high blood pressure in the morning, you need to check its service life, the serviceability of the batteries, and the correct use.
It is necessary to carefully analyze these reasons; maybe one of them is the provocateur of the disease.
The norm of pressure depends on age, anthropometric characteristics, as well as gender. Therefore, it makes sense to consider the reasons why blood pressure rises in the morning separately for men and women.
Diagnostics
The diagnosis of hypertension is based on blood pressure readings. Your doctor may recommend 24-hour blood pressure monitoring. This test involves wearing a device that shows regular blood pressure readings throughout the day and night. The doctor will also review the patient's medical history and perform a physical examination. If necessary, he will prescribe additional diagnostic methods to confirm or exclude the diagnosis. Examples of additional diagnostic methods include:
- echocardiography - ultrasound of the heart
- an electrocardiogram (ECG) to monitor the electrical activity of the heart
- blood tests
- Analysis of urine
Hormonal disorders
The endocrine system has the greatest influence on blood pressure levels. In this regard, if there is such a problem as desynchronization of daily blood pressure fluctuations, first of all you should think about pathologies in this area. Tonometry indicators can be affected by hormones of the pituitary gland, adrenal cortex, thyroid and pancreas. All of them have a direct or indirect effect on one or more links in the regulation of a given parameter of the body’s homeostasis.
Causes of high blood pressure in the morning are also: pregnancy
The most common reasons include:
- taking hormonal medications;
- hormonally active tumors of the endocrine and mixed secretion glands;
- injury to glandular tissue;
- strictures and tumor lesions of the excretory ducts of the glands;
- hereditary pathologies of cell receptors;
- nutritional obesity;
- presence of diabetes mellitus;
- the period of restructuring of the body during puberty or early pregnancy.
Treatment
Treatment of morning hypertension involves addressing the underlying cause. If the morning rise in blood pressure is caused by medications, the doctor may need to change the dose or time of day the person takes the medications. In some cases, your doctor may recommend taking additional medications. Some people experience a morning rise in blood pressure as a result of certain lifestyle factors. A person may consult a doctor for specific advice on diet, exercise, or smoking cessation.
Causes of morning increases in blood pressure in women
Women may face this problem due to high psycho-emotional stress and frequent stress. A morning increase in blood pressure sometimes occurs against the background of diseases of the genitourinary system, which are accompanied by the problem of removing excess fluid from the body. Its excessive concentration in tissues may be the reason why blood pressure rises in the morning.
- What to do if your child has knee pain in the morning
Taking some birth control pills can increase estrogen levels. As a result of its excess, blood pressure may rise. Moreover, this phenomenon is observed mainly in the morning.
Hypertension cannot be excluded as a provoking factor. This disease is usually caused by a violation of the tone of blood vessels. As the lumen decreases, blood flow becomes difficult in them.
Prevention
A healthy lifestyle helps control morning hypertension at other times of the day. A healthy lifestyle includes:
- balanced diet low in sodium, refined sugar and saturated fat
- limiting alcohol consumption
- to give up smoking
- doing exercises for 90-150 minutes every week
- maintaining a body mass index (BMI) from 18.5 to 24.9
- Stress management techniques such as yoga or meditation
- taking blood pressure medications
- treating underlying conditions that may contribute to hypertension
First aid
If the pressure has risen significantly, then help the patient urgently. He is placed on high pillows so that his head, along with his shoulder blades and shoulders, is raised 30 degrees. The flow of fresh air into the room is important, so open a window or turn on a fan. The patient should not have tight clothing. It is necessary to unfasten the collar, loosen the belt or belt. If there are dentures in the mouth, they are removed.
Calling an ambulance is mandatory so that doctors can bring the patient back to normal and prescribe treatment. Before the specialists arrive, you need to take a hot foot bath. A replacement for the procedure is a heating pad, which is filled with hot water and applied to the feet.
To lower blood pressure, you are given antihypertensive medications to take. Glycine, which is placed 1 gram under the tongue, will ease the course of the crisis. For headaches, you can take Baralgin and 0.5 tablets of Aspirin in soluble form. If the patient’s blood pressure has risen sharply for the first time and there is no medication at hand, then it can be reduced by holding your breath for a long time.
Why might this happen?
In fact, absolutely all people experience a slight increase in blood pressure in the morning and this is normal.
This is due to the fact that already in the evening, before going to bed, the metabolic processes in the body slow down, thereby reducing the pulse and blood pressure in the vessels. The lowest blood pressure levels are observed at night and early in the morning.
And immediately after waking up, the metabolism accelerates back, the production of hormones increases, which causes a jump in blood pressure. At the same time, in healthy people the indicator rises only slightly, by just a few points, and then levels off to normal values.
Increase in blood pressure to 130/80 mm. rt. Art. and less, is also considered insignificant and can occur due to external factors, bad habits and lack of sleep, after eliminating which it returns to normal. It can also occur in older people.
But if the pressure after waking up jumps to more than 140/90 mm. rt. Art. and does not subside throughout the day, then this is already a sign of arterial hypertension, but we’ll talk about it a little later.
Wrong lifestyle
The most popular and easily solved reason for this phenomenon. Not taking your health seriously has a negative impact on the functioning of the cardiovascular system, which causes a rise in blood pressure after waking up.
Unfavorable factors include:
- Smoking and drinking alcohol before going to bed. Nicotine promotes vasoconstriction, which subsequently develops atherosclerosis. This leads to the appearance of hypertension and a persistent increase in blood pressure not only after waking up, but throughout the day. Alcohol initially dilates the blood vessels, and after some time they sharply narrow, causing a surge in pressure. Therefore, drinking alcohol in the evening or at night leads to an increase in blood pressure in the morning.
- A sedentary lifestyle leads to poor circulation, deterioration in the quality of blood vessels, and reduces their permeability. If a person’s low physical activity is observed over a long period, this causes a stable increase in blood pressure, including after waking up.
- Overeating and eating very salty foods at night. Any meal enhances the functioning of the gastrointestinal tract and heart, speeds up metabolism, which for physiological reasons causes an increase in pulse and blood pressure. And overeating leads to increased stress on the body, which can negatively affect blood vessels. Eating salty foods contributes to the narrowing of blood vessels and the accumulation of fluid in the body.
If blood pressure rises in the morning due to these reasons, simple prevention will be sufficient for treatment, which consists of leading a healthy lifestyle and following a proper diet.
Sleep disturbances and stress
For proper rest, the adult body requires at least eight hours of sleep per day.
Reducing this time, as well as staying awake at night, leads to hormonal imbalances and disruptions in the functioning of the cardiovascular system. When the body does not get the rest it needs, this affects the condition of the entire body and leads to increased blood pressure after sleep.
As for stress, it increases the level of the hormones adrenaline and cortisol, which leads to constant tension. At the same time, the heart rate increases, blood pressure rises, and metabolism accelerates. Being under constant stress, with neuroses and depressive states, the body is overstrained, which causes an increase in blood pressure upon awakening.
Means for stabilizing pressure
In case of manifestations of hypertension, it is necessary to contact a general practitioner or cardiologist, who, based on the studies performed, age characteristics, and concomitant diseases, will select medications. If your blood pressure has risen sharply and a serious health threat has arisen, you can take Nifidipine or Corinfar tablets. Read more about Corinfar here.
Traditional medicine recipes are also aimed at stabilizing arterial parameters. Existing methods:
- Take freshly cut nettle, chop it, add honey in equal proportions. Take 1 tbsp daily. spoon with cold water.
- Take 1 tbsp honey mixture. add to water. Replace them with tea and coffee.
- Take 30 grams of aloe liquid, juice from one lemon, a couple of chopped garlic cloves, mix everything with honey, take a teaspoon before meals.
- Rose hips are filled with water and boiled, then lemon juice and honey are added. Drink instead of tea.
This is interesting! The effect of honey on blood pressure - 10 traditional recipes