Hemorrhagic vasculitis: photos, causes and methods of treatment in children and adults
Hemorrhagic vasculitis is also called allergic purpura, capillary toxicosis, or, after the names of the authors who described it, Henoch-Schönlein disease. The disease is part of a large group of vasculitis, inflammation of blood vessels of various types and sizes.
The peculiarity of the reaction of the vascular wall is aseptic conditions (absence of a pathogen) and the dominant role of a pronounced allergic reaction. The disease is accompanied by increased thrombus formation, impaired blood microcirculation in tissues and internal organs, which leads to damage to the kidneys, joints, and digestive organs.
Men under 20 years of age and children from 7 to 13 years of age are more susceptible to capillarotoxicosis. The incidence in these populations ranges from 14 to 24 per 10,000.
Causes
The causes of the disease have not been precisely established. It is considered to be autoimmune. However, a connection with factors activating pathological processes has been identified. These include:
- traumatic damage to the skin and blood vessels;
- transferred viral and bacterial infectious diseases, of particular importance is given to acute and chronic inflammation in the upper respiratory tract (influenza, ARVI, tonsillitis, sinusitis), measles, frequent sore throats, chicken pox, typhus, streptococcal diseases;
- vaccinations during routine vaccination, prophylactic use of immunoglobulins;
- food allergies;
- restructuring of the body during malignant and benign tumors;
- changes in women during pregnancy;
- the influence of increased doses of solar radiation (with prolonged tanning), temperature fluctuations, radiation;
- allergic reactions to medications (usually antibiotics, sedatives and antihypertensive drugs);
- metabolic disorders in endocrine diseases (diabetes mellitus);
- genetic predisposition in the family.
- household and professional poisoning, toxic infection;
- in children - helminthic infestations;
- reaction to insect bites.
Hemorrhagic vasculitis in adults develops more often in old age, with weak and impaired immunity.
Prevention
The main measures to prevent hepatitis B in its relapses include:
- Adequate treatment of acute infectious diseases of the upper respiratory tract and timely sanitation of infectious chronic foci of ENT organs.
- Exclusion/minimization of contacts with allergens (if there is a history of allergic reactions) and control of medications.
- Preventing hypothermia of the body.
- Strengthening the immune system (hardening, rational nutrition).
- Dispensary observation of ill persons for 2 years.
Symptoms of hemorrhagic vasculitis, photo
Manifestations of the disease depend on which organs and systems are affected. Hemorrhagic vasculitis can manifest itself in one or more groups of symptoms (see photo). The main ones are the following:
- skin lesions;
- joint damage;
- lesions of the gastrointestinal tract;
- renal syndrome;
- in isolated cases - damage to the lungs and nervous system.
The most characteristic is the acute onset of the disease, accompanied by an increase in temperature to febrile levels. There may be cases when there is no increase in temperature.
- Skin syndrome (or purpura) occurs in every patient. It manifests itself in the form of a symmetrical small-spotted or maculopapular hemorrhagic rash, localized mainly on the extensor surfaces of the lower (less often upper) extremities, around large joints and on the buttocks. The rash can be represented by single elements, or it can be intense, combined with angioedema. As a rule, the rashes are recurrent and wave-like. When the rash fades, the pigmentation remains. In case of frequent relapses, peeling of the skin occurs at the site of the rash.
- Articular syndrome is often observed simultaneously with skin syndrome; it is most typical for adults. Most often, the process involves the large joints of the legs, most rarely the elbows and wrists. Pain, redness and swelling are noted. Typical for hemorrhagic vasculitis is the volatile nature of articular lesions. In 25% of cases, migrating joint pain precedes skin lesions. Joint syndrome, which rarely lasts more than a week, is sometimes combined with myalgia and swelling of the lower extremities.
- Abdominal syndrome is also observed in 2/3 patients. It is characterized by spastic abdominal pain, nausea, vomiting, and gastric bleeding. However, truly life-threatening phenomena are observed only in 5% of patients.
- Renal syndrome is observed less frequently (from 40 to 60% of cases) and does not develop immediately. It manifests itself in the form of hematuria (blood excretion in the urine) of varying severity; in rare cases, the development of glomerulonephritis (kidney inflammation) of the hematuric or nephrotic form is possible. More often, glomerulonephritis manifests itself in the first year of the disease, less often it occurs during the next relapse of hemorrhagic vasculitis or after the disappearance of all other manifestations of the disease.
In isolated cases, pulmonary complaints are observed - bleeding, hemorrhages. Damage to the nervous system also rarely occurs - headaches, convulsions, and the possible development of encephalopathy or polyneuropathy.
How to classify hepatitis B: by form, course or mechanism of occurrence?
Types of hemorrhagic vasculitis vary in form and course. This is, in fact, what its classification is based on. So, based on clinical manifestations, the following syndromes are distinguished:
Skin manifestations of eosinophilic granulomatosis (Churg-Strauss syndrome)
- Cutaneous - the most common variant, unrelated to thrombocytopenia, although outwardly quite similar to it;
- Articular , as a rule, occurs together with the skin and is characterized by the involvement of various joints in the process, including large ones. In this case, migrating (“flying”) pain, swelling in the joint area and symmetry of the lesion are observed;
- Abdominal , preceded by intestinal damage with possible intestinal perforation and intestinal bleeding;
- Renal , proceeding according to the scenario of acute glomerulonephritis, and in other cases giving nephrotic syndrome;
- Mixed form of hepatitis B (combination of several types).
Depending on the clinical course, phase of activity and severity of the disease, three types of hemorrhagic vasculitis are distinguished:
- Mild course:
- Moderate degree of activity;
- Highly active process.
However, the classification also includes such a factor as the beginning of a pathological process associated with its further course. In such cases, we can talk about hemorrhagic vasculitis with:
- Lightning-fast version of the current;
- Acute period;
- Subacute course;
- A protracted process;
- Chronic relapsing form.
When studying vasculitis, the conclusion suggests itself that the prerequisite for the syndrome is an inadequate immune response of the body to some factor that disrupts immunity. But hepatitis B that occurs against the background of another pathology is not always of the same type, since they differ in the mechanism of formation of the pathological process. They have their own varieties, which only specialists can classify. We will just try to add a little information about vasculitis, which is of great interest to our readers. As a rule, these hemorrhagic syndromes are secondary, since they occur against the background and as a result of some disease:
- Cerebral vasculitis is formed due to non-infectious inflammation of the vascular walls of the bloodstream of the brain. Usually it is secondary in nature and accompanies systemic lupus erythematosus, rheumatoid arthritis, scleroderma and other autoimmune processes. With rare exceptions, isolated forms are found as part of the types of systemic vasculitis (primary);
- Cryoglobulinemic is considered to be the result of the formation at temperatures below 37°C of insoluble protein compounds - cryoglobulins, which are deposited in small-caliber vessels and can enter the circulation, as evidenced by their presence in a certain concentration when analyzing blood serum. This may likely explain the negative effects of cold and the appearance of hemorrhagic vasculitis in autoimmune diseases in some patients;
Cryoglobulinemic cutaneous vasculitis of varying severity and stages - Leukocytoclastic (leukocytoclastic angiitis) is often a companion to cryoglobulinemia and is called allergic cutaneous vasculitis, or accompanies Henoch-Schönlein purpura (the variant we describe). Primary leukocytoclastic vasculitis can be considered in the case of inflammation of the vascular wall, the cause of which could be an allergy;
- Urticarial vasculitis sometimes accompanies skin syndrome with hepatitis B, resembles an allergy (urticaria) and can rarely be an independent disease if it is of an allergic nature.
Hemorrhagic vasculitis in children
Symptoms of vasculitis in children, depending on the frequency of their occurrence, are distributed as follows:
- rash in the form of papules and red spots – 100% of cases
- arthritis and joint pain – 82%
- abdominal pain – 63%
- kidney damage (glomerulonephritis) – 5-15%.
Most often, recovery occurs spontaneously. Therefore, the disease is relatively favorable in childhood, especially if nutritional rules are followed and the possible causative factor is eliminated. After inflammation subsides, the risk of relapse is greatest in the first 3 months, but may occur later.
After recovery, you should adhere to the principles of dietary nutrition throughout the year and avoid contact with allergens that enter through the respiratory tract.
Skin syndrome is the leading one in the clinical picture of vasculitis. It is characterized by the following features:
- the appearance of a rash called purpura;
- its symmetry;
- purpura rises above the skin and is easily palpated;
- at the same time there may be red spots, pimples, blisters, which are characterized by itching;
- primary rashes on the feet, later they spread to the thighs and buttocks;
- after a couple of days, the rash turns from bright red to brown, and then turns pale and disappears;
- Sometimes pigmented lesions may remain and persist for a long time.
The development of glomerulonephritis usually occurs a month after the appearance of the first symptoms of the disease. Kidney damage can occur with minimal symptoms or be prone to an aggressive course. Depending on this, the clinical and laboratory signs of glomerulonephritis are very diverse. They include:
- protein in urine;
- edema, sometimes very pronounced as part of nephrotic syndrome, in which protein loss in the urine can reach 3.5 g per day;
- pain in the lumbar region;
- redness of urine (macrohematuria) or only microscopically detectable presence of red blood cells in it (microhematuria);
- transient increase in pressure.
Abdominal syndrome is a consequence of intestinal ischemia. In children it is characterized by:
- nausea;
- vomit;
- the appearance of bloody streaks in the stool;
- diffuse pain throughout the abdomen, like colic;
- pain intensifies after eating;
- loose stool.
The abdominal form of hemorrhagic vasculitis resembles an “acute abdomen”, traditionally requiring surgical intervention. However, for this disease it is contraindicated, because the reason is vascular damage. Adequate drug therapy is required.
Articular syndrome in hemorrhagic vasculitis has typical symptoms that distinguish it from articular syndrome in other diseases (osteoarthrosis, rheumatoid arthritis, gout). These include:
- absence of joint destruction;
- symmetry of the lesion;
- no migration of pain;
- frequent damage to the ankle and knee joints.
Treatment of a child with hemorrhagic vasculitis must begin in a hospital setting. Three weeks of bed rest followed by extension is usually suggested.
Diet
Hypoallergenic diet
- Efficacy: therapeutic effect after 21-40 days
- Timing: constantly
- Cost of products: 1300-1400 rubles. in Week
Diet Table No. 1
- Efficacy: therapeutic effect after 3 weeks
- Terms: 2 months or more
- Cost of products: 1500 - 1600 rubles. in Week
Diet 7 table
- Efficacy: therapeutic effect after a week
- Terms: 1 month or more
- Cost of products: 1200-1300 rubles per week
A hypoallergenic diet is prescribed, which involves excluding obligate allergens from the diet: milk, fish, citrus fruits, chocolate, cocoa, orange and red vegetables/fruits, as well as extractive substances. For abdominal syndrome, a modified Table No. 1 according to Pevzner is indicated until it is completely relieved. For nephritis - dietary Table No. 7 with a gradual transition to a hypochloride diet.
How is hemorrhagic vasculitis diagnosed?
Henoch-Schönlein disease is quite easy to diagnose in a patient who has all three main symptoms.
There are slight differences in the course of the disease in children and adults.
In children:
- More than 30% of children develop fever.
- Characteristic is the acute onset and course of the disease.
- Abdominal syndrome is accompanied by loose stool streaked with blood.
- Often the kidneys are involved in the process from the very beginning, with hematuria and proteinuria detected in urine tests.
In adults:
- The onset of the disease is delayed, the symptoms are milder.
- Abdominal syndrome occurs in only 50% of patients and is rarely accompanied by nausea and vomiting.
- Kidney damage leads to the development of chronic diffuse glomerulonephritis, with the formation of chronic renal failure.
Diagnostics
Diagnosis of the disease is carried out comprehensively. First of all, the doctor conducts an oral interview, during which he clarifies the patient’s complaints and collects an anamnesis. In the future, the following studies may be prescribed:
- Ultrasound of the abdominal organs and kidneys.
- Determination of bleeding duration.
- Carrying out a cuff test, as well as a tourniquet and pinch test.
- Fecal examination.
- Conducting immunological studies, as well as blood biochemistry.
- Virological studies to detect hepatitis.
- Carrying out endoscopic examination of the gastrointestinal tract.
- A blood test can reveal an increased number of leukocytes and ESR. Immunological disorders are also observed in the form of an increase in immunoglobulin A and a decrease in the level of immunoglobulin G.
- During the physical examination, the doctor checks the functioning of the joints and carefully examines the skin to identify changes in their color and possible rashes. If swelling is detected in the facial area, this may indicate a disruption in the normal functioning of the urinary system. You should also check your pulse.
The disease should be distinguished from the following ailments and conditions:
- Infectious endocarditis.
- Systemic vasculitis (Goodpasture's syndrome, periarteritis nodosa, Behçet's disease).
- Diffuse connective tissue diseases (systemic lupus erythematosus).
- Meningococcemia.
- Macroglobulinemic Waldenström's purpura.
- Yersiniosis.
- Crohn's disease.
Additionally, a trepanobiopsy procedure and bone marrow examination may be prescribed.
Clinical manifestations of forms and variants of the course of hepatitis B
The previously listed syndromes relating to skin rashes, gastrointestinal disorders, joint pain and renal pathology are considered supporting signs in the diagnostic search for hemorrhagic vasculitis, and therefore they should be given a more detailed description.
The most common and widely known skin syndrome is characterized by the following manifestations:
- The extensor surfaces of the upper and lower extremities (lower third of the leg and dorsum of the foot) are dotted with a symmetrical rash (papular-hemorrhagic), spreading to the joints and gluteal region (less often to the trunk). Sometimes blisters (urticarial elements) are added to the rash, which is very similar to urticaria;
- Absence (or appearance in very rare cases) of rashes on the stomach, scalp, face, neck;
- A pink, red or deep red hemorrhagic rash that does not disappear with pressure (different from an allergic one), which in severe cases can merge, ulcerate, necrotize and subsequently leave noticeable pigmentation (doctors call it hemosiderosis);
- Angioedema, affecting the hands, feet, almost the entire face and scalp, genitals, covering most of the body with painful infiltrates and “flying” edema, which can quickly disappear if you begin to intensively treat hepatitis B.
Cutaneous manifestations of hemorrhagic vasculitis
With a mild course, the patient’s condition changes slightly, an increase in temperature is rare (and then no higher than low-grade), rashes affect small areas of the body, and there are no gastrointestinal disorders (abdominal syndrome).
A moderate degree of activity is characterized by:
- The condition of the sick person is assessed as moderate to severe;
- Presence of fever (38°C and above);
- The appearance of general weakness, pain in the head;
- The presence of pain in the joints and their swelling;
- Excessive skin rashes, sometimes with the development of angioedema;
- Manifestation of abdominal syndrome: nausea, vomiting, diarrhea (sometimes with blood), painful abdominal pain;
- Peripheral blood reaction: leukocytosis exceeding 10x109/l, neutrophilia with a shift to the left, eosinophilia, accelerated ESR - 20-40 mm/hour, accelerated Lee-White coagulation, violation of the ratio between protein fractions.
A high degree of activity gives a severe clinical picture of the process and is expressed:
- Headaches, weakness and malaise;
- Significant disorders of the gastrointestinal tract (abdominal syndrome) with nausea, repeated bloody vomiting, frequent bloody stools;
- Vivid symptoms of articular syndrome;
- Skin necrotic purpura, which has a confluent nature;
- The appearance in other cases of cardiovascular disorders;
- Manifestations of kidney damage such as hematuric nephritis, as evidenced by an exceeding normal (over 5 Er in the field of view) number of red blood cells in the urine;
- Significant changes in laboratory parameters.
In addition, hemorrhagic vasculitis may be accompanied by other clinical manifestations, which are not obligatory, but are sometimes present and give additional signs of hepatitis, for example, damage to the blood vessels of the heart and lungs, leading to pulmonary hemorrhages. Or symptoms characteristic of cerebral vasculitis with damage to the blood vessels of the brain:
- Headache;
- Delusional states;
- The appearance of convulsive and/or meningeal syndrome.
Obviously, it is not possible to isolate hemorrhagic vasculitis from other autoimmune diseases, to accurately classify it and to derive a unified picture of clinical manifestations, since it has a strong connection with these processes and, like a syndrome, accompanies them.
Treatment of hemorrhagic vasculitis
First, you need a diet (allergenic foods are excluded). Secondly, strict bed rest. Thirdly, drug therapy (antiplatelet agents, anticoagulants, corticosteroids, immunosuppressants - azathioprine, as well as antithrombotic therapy).
The following drugs are used:
- activators of fibrinolysis - nicotinic acid.
- heparin in a dosage of 200-700 units per kilogram of body weight per day subcutaneously or intravenously 4 times a day, gradually withdrawn with a decrease in the single dose.
- disaggregants - chimes 2-4 milligrams/kilogram per day, trental intravenous drip.
- In severe cases, plasmapheresis or glucocorticosteroid therapy is prescribed.
- In exceptional cases, cytostatics such as Azathioprine or Cyclophosphamide are used.
In general, the course of the disease is favorable, and immunosuppressive or cytostatic therapy is rarely used (for example, in the development of autoimmune nephritis).
- The duration of treatment for hemorrhagic vasculitis depends on the clinical form and severity: 2-3 months - for mild cases; 4-6 months - for moderate cases; up to 12 months - with severe recurrent course and Schönlein-Henoch nephritis; in case of chronic course, treatment is carried out with repeated courses for 3-6 months.
Children must be registered at a dispensary. Conducted over 2 years. For the first 6 months, the patient visits the doctor monthly, then once every 3 months, then once every 6 months. Prevention is carried out by sanitation of foci of chronic infection. Regularly examine stool for helminth eggs. Such children are contraindicated in sports, various physical procedures and exposure to the sun.
Answers on questions
What is meant by a hypoallergenic diet?
- First of all, highly allergenic foods should be excluded from consumption, such as eggs, chocolate, citrus fruits, coffee and cocoa, sea fish and seafood, and nuts. It is also necessary to avoid fatty and fried foods. The diet should be dominated by low-fat dairy products, stewed and boiled dishes. Green apples, cereal porridges, turkey and rabbit meat, and vegetable oils are allowed.
What is the prognosis for hemorrhagic vasculitis?
- As a rule, the prognosis, especially for mild forms of the disease, is favorable. Severe hemorrhagic vasculitis is fraught with recurrence of the disease and the occurrence of complications (nephritis complicated by renal failure). With the fulminant form, there is a high probability of death within a few days after the onset of the disease.
Are patients who have suffered hemorrhagic vasculitis taken to the dispensary?
- Clinical follow-up in adults after illness is not indicated. Children must be monitored for two years. Monthly for the first six months, quarterly for the next six months, and every 6 months for the last year. Children should not play sports; physiotherapy and insolation (sun exposure) are contraindicated for them.
Is it possible to develop complications and consequences after hemorrhagic vasculitis and what are they?
- Yes, the disease can lead to intestinal obstruction and peritonitis, chronic renal failure, dysfunction of internal organs (heart, liver), anemia and pulmonary hemorrhages; in children, hemorrhagic diathesis may develop.
Pathogenesis
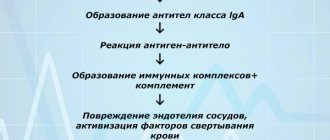
The mechanism of development of hemorrhagic vasculitis (HV) is based on a generalized immunocomplex necrotizing lesion of the blood vessels of the microvasculature of the skin and internal organs with the formation/deposition of granular IgA deposits (antigen-antibody complexes) in the vascular wall and activation of the complement system. As a consequence, a protein membrane attack complex is formed, which underlies the osmotic lysis of endothelial cells.
Also, when the complement system is activated, chemotactic factors are actively released. affecting polymorphonuclear leukocytes, which in turn secrete lysosomal enzymes that aggravate damage to the vascular wall. As a result of damage to the structure of the vascular endothelium, collagen fibers are exposed, which promotes the adhesion of platelets to the surface of the endothelium and the initiation of the blood clotting mechanism. Subsequently, fibrin deposits form in the vessels, blood rheology worsens, aggregation of erythrocytes and platelets , and intravascular disseminated blood coagulation develops.
Against the background of increased vascular permeability and the development of thrombosis with subsequent depletion of the anticoagulant (antithrombin-III) link and thrombocytopenia of consumption, ruptures of blood vessels of the microvasculature of the skin and internal organs occur, which lead to the development of clinical symptoms of hemorrhagic syndrome. The pathogenesis of hemorrhagic vasculitis is schematically presented in the figure below.
Pathogenesis of hemorrhagic vasculitis
How to prevent exacerbations?
After discharge from the hospital, the patient should not forget about his illness at home. Of course, by that time he will already know everything about the nature of the disease, prevention of exacerbations, behavior in everyday life, nutrition and daily routine. Having immersed himself in a homely atmosphere, the patient will not take any medications without a doctor’s prescription, will not attack foods that can provoke a relapse (allergens), but will eat well and will take quiet, easy walks in the fresh air every evening.
In addition, the following are contraindicated for a person:
- Excessive anxiety, mental stress;
- Vaccinations (possible only for health reasons);
- Hard physical labor (children are exempt from physical education lessons);
- Hypothermia;
- Administration of immunoglobulins (antistaphylococcal, antitetanus, etc.).
Due to the fact that hemorrhagic vasculitis is predominantly a childhood disease, special recommendations are provided for children (or parents?):
- Every six months the child visits the attending physician (in the absence of exacerbations);
- Clinical observation for at least 5 years if the kidneys remain healthy, but if they are damaged, control may be lifelong;
- Children are completely exempt from physical education for a year, then move to the preparatory group;
- A mandatory visit to the dentist and otolaryngologist is required 3 times a year;
- Regular urine tests (general and Nechiporenko) and fecal tests for helminths;
- Vaccinations are excluded for 2 years, and after this time, routine vaccination is carried out, but with the permission of the attending physician and under “antihistamine cover”;
- Compliance with an anti-allergenic diet – 2 years;
Advice to parents or other relatives about treatment at home, relapse prevention, nutrition and behavior at school and at home.
List of sources
- Lyskina G. A. Systemic vasculitis. In the book: Pediatric rheumatology. Guide for doctors / Ed. A. A. Baranova, L. K. Bazhenova. M.: Medicine, 2002. pp. 221–270.
- Kulaga V.V., Romanenko I.M., Afonin S.L. Allergic diseases of the blood vessels of the skin. Lugansk: “Etalon-2”, 2006. 168 p.
- A practical guide to childhood diseases, edited by prof. Kokolina V.F. and prof. A.G. Rumyantsev, volume IV. Hematology/oncology of childhood (edited by Rumyantsev A.G. and E.V. Samochatova). Medical practice – M. Moscow 2004 Zinovieva G.A., Frolkova E.V. Hemorrhagic vasculitis. Clinic and treatment // ros. pediatrician, journal — 1998. -N12. P.24-26.
- Krivosheev O.G., Gulyaev CB, Semenovykh A.G. Modern principles of treatment of Henoch-Schönlein purpura // Doctor. 2007. No. 4. -P.54-55.