Essential arterial hypertension is an increase in systolic blood pressure at the time of heart contraction and blood ejection to 140 mmHg. Art. and above this mark and/or diastolic blood pressure at the moment of relaxation of the heart muscle to 90 mmHg. Art. and higher.
The Yusupov Hospital diagnoses and treats essential hypertension. The experience of highly qualified doctors and modern medical equipment make it possible to diagnose the disease at an early stage of its development and prevent complications.
Doctors at the Yusupov Hospital urge people to be attentive to their health.
Essential hypertension - what is it?
Essential hypertension is a form of arterial hypertension (AH), characterized by a stable increase in blood pressure (from 140/90 mm Hg and above) in the absence of pathological changes in the organs and systems that regulate it.
Essential hypertension accounts for approximately 90% of the total number of cases of arterial hypertension.
Every year, about 9 million cases of this form of hypertension are reported worldwide, with a mortality rate of 6.5%.
Essential arterial hypertension
Before complications develop, the disease is often asymptomatic, and its only manifestation is an increase in blood pressure. Complaints are absent or nonspecific. Patients note periodic headaches, often in the forehead or back of the head, dizziness and tinnitus.
It has now been proven that these symptoms cannot serve as indicators of high blood pressure and are likely to have a functional origin. They occur in patients with arterial hypertension no more often than in the general population, and do not correlate with blood pressure levels.
An exception is severe headache with malignant arterial hypertension caused by cerebral edema. Symptoms and signs of cardiac damage are associated with: 1) left ventricular hypertrophy, which is a compensatory response aimed at normalizing increased wall stress due to increased afterload; 2) concomitant ischemic heart disease; 3) heart failure as a complication of both pathological processes. Recent studies cast doubt on the “benign quality” of left ventricular hypertrophy in arterial hypertension. Regardless of the level of blood pressure, it increases the risk of myocardial infarction and sudden death by 3 times, and complex ventricular arrhythmias and heart failure by 5 times. Since the degree of increase in blood pressure and its duration do not always correlate with the severity of hypertrophy, it was suggested that some additional factors, in addition to arterial hypertension, play a role in its development. The pathogenetic role of genetic predisposition, humoral agents - the renin-angiotensin-aldosterone system, catecholamines, prostaglandins, etc. is discussed. These circumstances served as the basis for the introduction of the term “hypertensive (hypertensive) heart” and determine the importance of developing methods for preventing the reverse development of myocardial hypertrophy in arterial hypertension. hypertension.
The clinical significance of “hypertensive heart” is associated with impaired diastolic function of the myocardium due to an increase in its stiffness and the development of relative coronary insufficiency. A decrease in diastolic compliance of the left ventricle leads to an increase in its filling pressure and venous congestion in the lungs with unchanged systolic function. Patients note shortness of breath during physical activity, which increases with the addition of systolic myocardial failure. With long-standing arterial hypertension, symptoms of kidney damage can be detected - nictipolyuria. In uncomplicated essential arterial hypertension, symptoms of damage to the central nervous system are predominantly caused by concomitant atherosclerosis of the cranial and extracranial arteries. These include dizziness, impaired performance, memory, etc. History. The onset of the disease between the ages of 30 and 45 years and a family history of essential arterial hypertension are typical.
During clinical examination, the most important diagnostic sign is increased blood pressure. To measure it as accurately as possible, a number of rules must be followed (see Chapter 4). It must be borne in mind that when the patient is sitting, blood pressure may be higher than when the patient is lying down. To avoid discrepancies associated with atherosclerosis of the subclavian artery, blood pressure should be measured in both arms and, if differences are detected, subsequently monitored in the same arm.
Due to the involuntary psycho-emotional reaction of “anxiety” during the procedure of measuring blood pressure by a health worker in a medical institution, its result, especially with a single determination, is often overestimated compared to the data of automatic measurement in an outpatient setting (pseudohypertension). This can lead to overdiagnosis of borderline or mild arterial hypertension in almost 1/3 of cases. Therefore, the conclusion about elevated blood pressure should be based on the results of 3 separate measurements taken over 3-4 weeks, except in cases requiring emergency treatment. When blood pressure is more than 140/90 mm Hg. it is measured 2-3 times at each appointment and the average value is taken for further assessment. Blood pressure measurements are carried out at home by the patient himself or his relatives.
Particularly effective in eliminating the “alarm reaction” are new automatic devices for indirect measurement and recording of blood pressure over time, which can be carried out in an outpatient setting. The levels of such “outpatient” blood pressure when monitored are lower than “hospital” blood pressure in 80% of cases and serve as a more reliable criterion for diagnosing mild arterial hypertension.
Clinical signs of target organ damage . A physical examination of the cardiovascular system can detect signs of left ventricular hypertrophy, left ventricular failure and atherosclerosis of various vascular systems. With left ventricular hypertrophy, the apical impulse often becomes resistant, and a decrease in the compliance of its chamber is manifested by the appearance of S4 above the apex, indicating its diastolic dysfunction. Clinical signs of kidney damage with a detailed picture of chronic renal failure are more characteristic of malignant arterial hypertension. Signs of damage to the central nervous system are usually associated with complications of arterial hypertension and concomitant cerebral atherosclerosis.
Hypertensive retinopathy . According to the classification of retinal vascular damage and vascular complications of arterial hypertension by Keith and Wagener (N.Keith, H.Wagener, 1939), there are 4 degrees of retinopathy. Grade I is characterized by minimal narrowing of the arterioles and unevenness of their lumen. The ratio of the diameter of arterioles and venules decreases to 1:2 (normally 3:4). In grade II, there is a pronounced narrowing of the arterioles (arteriole-venous ratio 1:3) with areas of spasm. Characteristic is the stretching of the venules and their compression at the intersection with the arterioles, with which they are located in the same connective tissue sheath, due to thickening of the arteriole wall (a symptom of the Salus-Hun intersection). In grade III, against the background of spasm and sclerosis of the arterioles (arteriole-venous ratio 1:4), characteristic multiple hemorrhages in the form of flames and loose exudates resembling “whipped cotton wool” are detected. These exudates represent areas of retinal ischemia or infarction in which swollen nerve fibers are identified. The exudates fade after a few weeks. Dense, small, well-defined exudates due to lipid deposition may also be found, sometimes persisting for years. They are of less clinical significance and do not indicate acute arteriolar injury. A distinctive feature of grade IV retinopathy is the appearance of papilledema, which is associated with any of these changes and reflects the extreme severity of malignant arterial hypertension. In this case, hemorrhages and exudates may be absent. In the early stages of retinopathy, vision is not affected. Extensive exudates and hemorrhages can cause visual field defects and, if the macula is affected, blindness.
Retinopathy of I-II degree is characteristic of “benign” essential arterial hypertension, and III-IV - of malignant one. With the acute development of malignant arterial hypertension, hemorrhages, exudates and papilledema are determined in the absence of changes in arterioles. With retinopathy of the I and II degrees, changes in blood vessels due to arterial hypertension practically do not differ from the signs of their atherosclerosis and are often caused by a combination of these two processes.
The generally accepted WHO classification (1962, 1978, 1993) is presented in table. 36. According to this classification, depending on the course, “benign” and malignant forms of the disease are distinguished. “Benign” essential arterial hypertension is divided into three stages (I, II, III), which approximately correspond to its three forms, determined by the level of blood pressure, primarily diastolic. Depending on the predominantly affected target organ, one or another clinical variant is distinguished.
The classification of essential arterial hypertension is based on the identification of three stages of the disease. Their characteristics are presented in table. 37.
Stage I is observed in 70-75% of patients with essential arterial hypertension. Most patients have no or vague complaints, primarily related to their psycho-emotional state. An increase in blood pressure, the level of which very roughly corresponds to a mild (mild) form of arterial hypertension, is not accompanied by objective signs of target organ damage. The nature of hemodynamic changes in most cases corresponds to the hyperkinetic type. Spontaneous normalization of blood pressure is possible, especially according to ambulatory monitoring, but for a shorter period than with borderline arterial hypertension. In a significant proportion of patients, the disease has a slightly progressive course with persistent stabilization at stage I for 15-20 years or more. Despite this, the long-term prognosis is unfavorable. As the results of the Framingham study showed, the risk of developing heart failure in such patients is increased by 6 times, stroke by 3-5 times, and fatal myocardial infarction by 2-3 times. In general, mortality during long-term observations was 5 times higher than in individuals with normal blood pressure levels.
Stage II in terms of blood pressure approximately corresponds to moderate arterial hypertension. The course of the disease in some patients remains asymptomatic, but examination always reveals signs of target organ damage caused by hypertrophy of the left ventricle and arteriolar wall (see Table 37). Hypertensive crises are characteristic. In urine tests, there are often no changes, but within 1-2 days after the crisis, slight transient proteinuria and erythrocyturia can be recorded. There may be a moderate decrease in glomerular filtration and signs of a symmetric decrease in the function of both kidneys with radionuclide renography. The hemodynamic profile predominantly corresponds to the normo(eu-)kinetic profile.
Stage III of the disease is characterized by vascular complications associated both with arterial hypertension and, to a large extent, with the accelerated development of concomitant atherosclerosis. It must be borne in mind that with the development of myocardial infarction and stroke, blood pressure, especially systolic blood pressure, often persistently decreases due to a decrease in blood pressure. This type of hypertension is called “decapitated.” This is characterized by a hypokinetic hemodynamic profile. According to the recommendations of the WHO and the II Congress of Cardiologists of the former USSR, when a patient with essential arterial hypertension develops myocardial infarction, angina pectoris, cardiosclerosis and congestive heart failure, the main disease, which is placed first in the clinical diagnosis, is considered to be ischemic heart disease. Thus, the “cardiac form” of essential arterial hypertension at stage III has no place in the diagnosis.
It should be noted that the stages of essential arterial hypertension according to the WHO classification fully correspond to the gradations of the disease identified by N.D. Strazhesko (1940). He characterized stage I as functional, youthful, “silent”, stage II as organic, characterized by organic changes in the cardiovascular and other systems, and stage III as dystrophic. Defining the stages of development of hypertension (essential arterial hypertension) according to the pathogenetic principle, G.F. Lang (1947) in his classification identified a prehypertensive state, stage I - neurogenic, stage II - transitional and stage III - nephrogenic. The name of stage III reflects the scientist’s idea of the obligatory participation of renal pressor substances in the consolidation of high blood pressure. The facts accumulated by subsequent research did not confirm this position, which prompted G.F. Lang’s student A.L. Myasnikov to propose a new classification, which became widespread in our country at that time. This classification provides for the identification of 3 stages of hypertension: I - functional, II - “hypertrophic” and III - sclerotic. Each of these stages includes 2 phases (A and B), which received the following names: IA - latent, or prehypertensive; 1B - transient, or transient; IIA - labile, or unstable; Information security - stable; IIIA - compensated and ШБ - decompensated.
Stages 1B and IIA correspond to stage I of the WHO classification, PB-IIIA - stage II and SB - stage III of essential arterial hypertension. A.L. Myasnikov’s classification also provides for the identification of cardiac, cerebral, renal and mixed variants depending on the predominant organ damage, and according to the nature of the course - rapidly progressing (malignant) and slowly progressing variants. Thus, the gradations of hypertension according to AHM Myasnikov are quite close to the modern WHO classification, which is currently the only one mandatory for practical medicine.
In recent years, it has been customary to distinguish variants of essential arterial hypertension depending on the hemodynamic and humoral profiles, which, as expected, has a certain significance for assessing prognosis and a differentiated approach to treatment. At the same time, all these options are largely conditional, as they transform into each other, and theoretically based recommendations for optimal treatment are not always effective in practice. The hemodynamic type of essential arterial hypertension - hyper-, eu- or hypokinetic - is determined on the basis of the numerical values of MOS (SI) and OPSS according to rheography or echocardiography or, indirectly, by the nature of arterial hypertension. Thus, the hyperkinetic type mainly corresponds to systolic arterial hypertension, and the hypokinetic type - diastolic hypertension. The clinical characteristics of each option are presented in table. 38.
Considering the important role of the renin-angiotensin-aldosterone system in the pathogenesis of essential arterial hypertension, depending on the activity of renin in the blood plasma, 3 variants of the disease are distinguished - g and per-, normo- and hyporenin, which have certain features of the clinical course and treatment. Characteristics of extreme variants - hyper- and hyporenin - are presented in Table. 39. It is assumed that hyporenin or volume-dependent arterial hypertension is associated with excessive secretion of mineralocorticoids. Since it practically does not occur in patients under the age of 40 years and is observed in more than 50% of patients over 60 years of age, it is assumed that this variant of arterial hypertension is a certain stage of the natural course of the disease. In this case, the decrease in renin activity may be secondary due to “functional inhibition” of the juxtaglomerular apparatus as a result of prolonged exposure to elevated blood pressure. It is possible that the different activity of renin is due to the unequal sensitivity of the adrenal glands to angiotensin II: a decrease in sensitivity leads to an increase in renin secretion, and an increase leads to hyporeninemia. Hyperreninemia may be secondary to increased activity of the sympathetic-adrenal system. Borderline arterial hypertension is a functional disease caused mainly by a reversible dysfunction of the central regulators of blood pressure, which is manifested by an increase in sympathetic tone. An increase in adrenergic impulses to the heart and veins leads to an increase in MOS due to an increase in myocardial contractility, heart rate and venous inflow, and increased impulses to the arterioles prevent their compensatory expansion. As a result, self-regulation of tissue blood flow is disrupted and a relative increase in peripheral vascular resistance occurs. The following criteria for the diagnosis of borderline arterial hypertension are identified, which are based on the results of three measurements of blood pressure, preferably in an outpatient setting:
- Blood pressure never exceeds the border level, that is, 140-159/90-94 mm Hg. according to WHO (1993) or 130-139/85-89 mm Hg. according to the recommendations of the US Joint National Committee on the Definition, Evaluation and Treatment of High Blood Pressure, 1992;
- with at least 2 measurements, the values of diastolic or systolic blood pressure are in the border zone;
- absence of organic changes in target organs (heart, kidneys, brain, fundus);
- exclusion of symptomatic arterial hypertension;
- normalization of blood pressure without antihypertensive therapy.
Considering the role of the psycho-emotional factor, at each examination of the patient it is recommended to measure blood pressure three times at short intervals and consider the lowest values as true.
Borderline hypertension occurs in 10–20% of the population and is heterogeneous in many respects. Although it is the main risk factor for the development of essential arterial hypertension, this transition occurs in no more than 20-30% of patients. In approximately the same percentage of patients, normalization of blood pressure is observed and, finally, in a significant proportion of patients, borderline arterial hypertension persists indefinitely.
The hemodynamic profile of such patients is also heterogeneous.
Along with the hyperkinetic type, which is observed in approximately 50% of patients, eukinetic is determined in 30% and hypokinetic in 20%. The variability of the course and state of hemodynamics is apparently due to the heterogeneity of the etiological factors of borderline arterial hypertension. Currently, the role of hereditary predisposition and pathology of cell membranes with an increase in the intracellular content of Na+ and Ca2+ has been proven. Obviously, there are other reasons for the occurrence of borderline arterial hypertension and further increases in blood pressure, which have not yet been established.
Depending on the most susceptible populations, the following clinical forms of borderline arterial hypertension can be distinguished: 1) juvenile; 2) psychoneurological; 3) menopausal; 4) alcoholic; 5) borderline arterial hypertension of athletes; 6) when exposed to certain occupational factors (noise, vibration, etc.). Factors of increased risk of developing essential arterial hypertension in patients with borderline hypertension are:
- burdened heredity. In this case, the transition to essential arterial hypertension is observed in approximately 50% of patients, and in the absence of this factor - in 15%;
- blood pressure level. The higher the blood pressure, the greater the likelihood of transition to essential arterial hypertension;
- excess body weight;
- the occurrence of borderline arterial hypertension after the age of 30 years.
Complications of essential arterial hypertension are caused by vascular damage of its own hypertensive and atherosclerotic origin. Hypertensive vascular complications are directly related to increased blood pressure and can be prevented by normalizing it. These include: 1) hypertensive crises; 2) malignant arterial hypertension syndrome; 3) hemorrhagic stroke; 4) nephrosclerosis and chronic renal failure; 5) dissecting aortic aneurysm and partly congestive heart failure with a “hypertensive heart”. According to the figurative expression of E.M. Tareev, atherosclerosis follows hypertension, like a shadow follows a person. Associated vascular complications are very common in patients with arterial hypertension, but cannot be prevented by lowering blood pressure alone.
They include: 1) all forms of coronary artery disease, including congestive heart failure and sudden death; 2) ischemic stroke; 3) atherosclerosis of peripheral vessels.
A hypertensive, or hypertensive, crisis is a sharp increase in blood pressure, accompanied by a number of neurohumoral and vascular disorders, mainly cerebral and cardiovascular. Abroad, this term is used in a narrower sense to refer to cerebrovascular disorders and is called “hypertensive encephalopathy.” Hypertensive crises are more typical for essential arterial hypertension than for most symptomatic ones, and may be the first clinical manifestation of the disease. According to A.L. Myasnikov, they are a kind of “quintessence” or “clot” of hypertension.
Hypertensive crises can develop at any stage of the disease. All etiological and predisposing factors to essential arterial hypertension contribute to their occurrence. These include, first of all, psycho-emotional stress, abuse of salty foods or alcohol, unfavorable environmental factors, in particular, a decrease in barometric pressure with increasing temperature and humidity. Crises can also be caused by the lack of treatment for arterial hypertension or inadequate therapy, which often occurs when the patient voluntarily violates medical recommendations.
In contrast to a simple increase in blood pressure, a crisis is characterized by a breakdown of local self-regulation with the occurrence of a syndrome of hyperperfusion, stasis, increased hydrostatic pressure in the capillaries and their permeability with tissue edema and diapedetic bleeding, up to the rupture of small vessels. These disorders are observed mainly in the cerebral and coronary bloodstream and less often affect the renal and intestinal circulations.
Diagnostic signs of a hypertensive crisis are: 1) sudden onset (from several minutes to several hours); 2) an increase in blood pressure to a level that is usually not typical for this patient (diastolic blood pressure is usually above 115-120 mm Hg); 3) complaints of a cardiac (palpitations, cardialgia), cerebral (headache, dizziness, nausea, vomiting, visual and hearing impairment) and general vegetative (chills, trembling, feeling hot, sweating) nature. According to the classification of N.A. Ratner et al (1956), depending on the clinical course, hypertensive crises can be type I (adrenal), type II (noradrenal) and complicated.
Type I hypertensive crises are associated with the release of catecholamines, mainly adrenaline, into the blood as a result of central stimulation of the adrenal glands. Their sympathetic-adrenal origin determines the predominance of symptoms of a general vegetative nature. Blood pressure does not reach very high numbers; there is a predominant increase in systolic pressure. Crises of this type usually develop rapidly, but are relatively short-lived (up to 2-3 hours) and stop relatively quickly, after which polyuria is often observed. Complications are rare.
Type II hypertensive crises are most typical for severe and malignant arterial hypertension. There are no clinical signs of hyperactivity of the sympathetic-adrenal system. Their main manifestation is hypertensive encephalopathy due to cerebral edema, which occurs against the background of a very significant increase in blood pressure, mainly diastolic (120-140 mm Hg or more). Characterized by a gradual increase in cerebral symptoms, which reach significant severity, up to stupor and coma. Focal neurological disorders are also often observed. The pulse is usually slow. When examining the fundus, exudates and initial signs of papilledema are detected. Such crises are usually long-lasting, but with timely antihypertensive therapy, the symptoms are in most cases reversible. Without treatment, hypertensive encephalopathy can be fatal. During a crisis, regardless of its nature, the ECG often shows transient depression of the ST segment with thickening or inversion of the T wave of “overload” or ischemic origin. After its relief, proteinuria, erythrocyturia, and sometimes cylindruria may be observed. These changes are more pronounced in type II crises. A complicated hypertensive crisis is characterized by the development of acute left ventricular failure, acute coronary circulatory disorders, and cerebrovascular accidents such as dynamic, hemorrhagic or ischemic stroke. Depending on the hemodynamic profile, hyper-, eu- and hypokinetic crises are distinguished, which can often be distinguished without instrumental examination based on the characteristics of the clinical course.
A hyperkinetic crisis is observed mainly in the early stage 1 of essential arterial hypertension and in its picture more often corresponds to a type I crisis. Characterized by a sudden sharp increase in blood pressure, mainly systolic, as well as pulse, with bright vegetative coloring and tachycardia. The skin is moist to the touch, and red spots often appear in the face, neck and chest. Eukinetic crisis develops more often in stage II of essential arterial hypertension against the background of a persistent increase in blood pressure and, in its manifestations, is a severe adrenal crisis. Both systolic and diastolic blood pressure were significantly elevated. A hypokinetic crisis in most cases develops at stage III of the disease and the clinical picture is similar to a type II crisis. Characterized by a gradual increase in cerebral symptoms - headache, lethargy, deterioration of vision and hearing. The heart rate is unchanged or slow. Diastolic blood pressure increases sharply (up to 140-160 mm Hg) and pulse rate decreases.
Etiology of the disease
Essential hypertension is classified as a chronic disease of unknown etiology. It is generally accepted that the main factor in the development of the disease is hereditary predisposition.
There are also additional risk factors:
- Insufficient physical activity. With physical inactivity, the functional and adaptive capabilities of the circulatory system are reduced.
- Excess weight. Obese people have a tendency to spasm blood vessels and narrow their lumen due to cholesterol deposits.
- Excessive salt intake. An adult needs only 4 grams of salt per day, but the average European resident consumes about 3 times more than this amount. Excess salt causes increased production of adrenaline and vasospasm.
- Lack of magnesium and calcium. These microelements prevent spasm of the heart muscle and blood vessels, thereby stabilizing blood pressure (BP).
- Alcohol consumption. If you do not exceed the recommended dose (that is, approximately 60 grams of alcoholic drinks with a strength of 40% for men and 40 grams for women), alcohol does not cause an increase in blood pressure. Exceeding this dose will lead to an increased release of norepinephrine and renin into the blood, due to which the pressure will begin to rise rapidly.
- Smoking. The effect of nicotine on the functioning of the cardiovascular system is in many ways similar to the effect of alcohol: it provokes the production of adrenaline and norepinephrine, which cause vasospasm, which in turn causes an increase in blood pressure.
- Age. As the body ages, the functional state of the systems that regulate normal blood pressure levels deteriorates.
Often the trigger for exacerbation is a stressful situation, which provokes the release of adrenaline and norepinephrine. That is why people who regularly experience nervous tension are more often predisposed to essential hypertension than others.
Other trigger mechanisms are also possible:
- poisoning;
- taking psychostimulants;
- use of hormonal contraceptives;
- pregnancy;
- kidney diseases;
- injuries, tumors and inflammatory diseases of the brain.
Traditional methods
If you have been diagnosed with the initial stage of essential hypertension, you can get rid of it with the help of traditional medicine. The use of some extracts and infusions normalizes blood pressure levels and restores the walls of blood vessels. The most popular and effective prescriptions against essential hypertension are:
- Mix in equal proportions
- To prepare the next medicine you will need beets, honey and marsh cudweed. This will require 800 grams of the first two ingredients and 100 mg of the last. Mix the ingredients thoroughly, then add one bottle of vodka to them. The resulting mixture is stirred until a homogeneous paste is obtained, then placed in a dark place for 2 weeks. You need to take the medicine one tablespoon 3 times a day.
Symptoms of the disease
The manifestations of essential hypertension have much in common with other diseases of the cardiovascular system. In addition to persistently elevated blood pressure, the following symptoms are distinguished:
- Headache (mainly in the temporal and occipital region).
- Rapid heartbeat (over 90 beats per minute).
- Dyspnea. Usually occurs as a consequence of deterioration in the functional capacity of the heart, which can lead to deterioration of blood supply to the brain and lungs.
- Feeling of coldness in the extremities. This condition is caused by impaired peripheral blood supply.
- Dizziness. Due to vascular spasm, the brain does not receive enough oxygen.
- Swelling of the limbs. They arise due to thinning of blood vessels, which leads to the accumulation of fluid in the tissues.
- Deterioration of vision. They arise due to impaired blood supply to the retina.
- Noise in ears. Occurs due to impaired blood supply to the brain.
- Fast fatiguability. It occurs as a result of a decrease in the functional capacity of the heart.
- Facial redness. Caused by increased tone of peripheral blood vessels.
Causes
Essential arterial hypertension can occur as a result of acute and chronic emotional stress, brain hypoxia of various origins, age-related neurohumoral changes, and salt abuse.
Predisposition factors: genetic, disorders of the nervous and endocrine systems, obesity, alcohol abuse, smoking, physical inactivity, old age. Occupational factors: noise, vibration; hormonal factors: increased renin levels, decreased nitric oxide production.
Blood pressure increases due to an imbalance between pressor and depressor factors, leading to changes in arterioles and capillaries, restructuring and functional disorders of cell membranes, including arterioles and smooth muscle cells, disruption of the activity of the calcium pump, an increase in the concentration of ionizing calcium in the cytoplasm and, finally, increased vascular resistance.
When to see a doctor
None of the above symptoms should be ignored. If the pressure readings approach 180/110, you should call an ambulance. If even a slight increase in blood pressure is observed over the course of several days, you should make an appointment with a therapist or cardiologist.
Formally, the upper limit of normal is considered to be a blood pressure of 140/90, but it is important to understand that these are rather arbitrary figures. For example, some patients do not feel discomfort even at 150/100, while for others 135/85 causes a significant deterioration in well-being. Therefore, it is important to focus primarily on your own condition.
Figure 1. How to protect yourself from hypertension. Source: MedPortal
How to prevent the development of hypertension
Primary prevention of high blood pressure and arterial hypertension includes measures and actions aimed at preventing the occurrence of the disease. Prevention and non-pharmacological treatment include:
- lifestyle changes;
- achieving and maintaining optimal body weight;
- reducing fat consumption (for example, replacing whole milk products with low-fat ones, consuming cheeses with a fat content of less than 30%);
- reducing alcohol and salt consumption (avoid foods such as sausages, canned and instant foods, mineral waters with high salt content);
- often eating raw food instead of processed food.
Regime measures also include increased physical aerobic activity and smoking restrictions. Hypertension (high blood pressure) is highly dependent on mental stress, especially feelings of anger, apathy, and disappointment. Therefore, primary prevention includes regulation of social relationships, self-regulation, and increasing self-esteem.
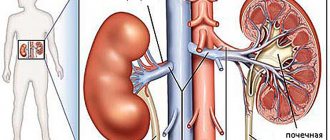
Target organs for essential hypertension
This definition is usually understood to mean those organs that are most susceptible to the negative effects of the disease (in this case, persistently elevated blood pressure). Target organs for essential hypertension:
- Heart. With increased load on this organ, hypertrophy of the left ventricle occurs. This creates the preconditions for insufficient oxygen supply to the myocardium, which can lead to the development of heart failure.
- Kidneys. Impairments in blood flow and glomerular filtration can eventually lead to renal failure, a syndrome in which the functional state of the kidneys significantly deteriorates. Over time, they may stop removing waste products normally, so it is important to start treatment on time.
- Vessels. Due to constant tension, they lose the ability to relax, which can lead to atherosclerosis of the arteries and peripheral vessels. A feeling of coldness in the extremities with high blood pressure occurs precisely for this reason.
- Brain. Stroke is a common complication of essential hypertension. They can be either hemorrhagic (bleeding in the brain) or ischemic (local disruption of the blood supply to the brain, leading to the death of its cells).
- Eyes. Impaired blood supply to the retina can lead to irreversible visual impairment, so the sooner treatment is started, the better the prognosis.
Is it possible to distinguish essential hypertension from other types based on symptoms?
It is possible to determine the differences between EAH and the manifestations of high rates in other types of hypertension, but they are few. First of all, the following factors are taken into account:
- age of the patient - the age of 35-45 years is typical for the development of essential hypertension; other types of disease are typical for other age groups;
- stability of indicators - with essential hypertension, pressure indicators are steadily increased, they are easy to treat;
- research results - with essential hypertension there are no characteristic test findings typical for other types of disease.
Diagnosis of hypertension
First of all, the patient himself should pay attention to the regularity of the appearance of symptoms associated with arterial hypertension and the level of increase in blood pressure. Results above 140/90 more than 3 times within 2 weeks should be cause for concern.
The doctor begins the diagnosis by collecting an anamnesis, that is, the history of the patient’s life and illness. As a rule, he clarifies the following points:
- Does the patient or his close relatives have kidney disease?
- How often does a person use pharmacological drugs (particular attention is paid to anti-inflammatory drugs, nasal sprays, contraceptives, antibiotics, hematopoietic drugs, as well as any psychostimulants).
- Does the patient have sudden episodes of muscle weakness, cramps, headaches, or paresthesia (nerve sensation such as tingling, burning, etc.)
After this, laboratory and hardware diagnostics are prescribed:
- Urine tests: general
- according to Nechiporenko
- according to Zimnitsky
- detection of free cortisol in daily urine.
- general
Diagnostics
Types of diagnosis of essential hypertension are as follows:
- analysis of patient complaints. The doctor clarifies how long ago the patient had problems with blood pressure, what measures he took, and whether he went to the hospital for treatment. It is also important to clarify what the patient’s working pressure is. Each person’s body is individual, therefore, in some cases, pressure indicators in one person are higher or lower than accepted standards, but do not carry any pathology;
- lifestyle analysis: a specialist must conduct research regarding the patient’s diet, physical activity, exposure to harmful production factors, etc.;
- the presence of essential hypertension in the patient’s relatives is analyzed;
- during the examination, the doctor identifies heart murmurs, wheezing in the lungs, signs of an increase in the mass and size of the left ventricle of the heart, insufficiency of the contractile function of the left ventricle, loss of elasticity and hardening of the arterial walls;
- general blood analysis. Allows you to identify signs of inflammation in the body. This fact is evidenced by an increased level of leukocytes in the blood;
- blood chemistry. Its results make it possible to assess the state of lipid, protein, carbohydrate, and mineral metabolism. Based on the level of microelements in the blood, one can assess the functioning of many systems and organs;
- urinalysis: low urine density is determined, indicating problems with the kidneys;
- ECG (electrocardiography): reveals an increase in the size of the left ventricle of the heart, as well as the degree of its “overload”;
- EchoCG (echocardiography): makes it possible to assess the size of the heart, the condition of the valves, the presence of disorders of the contractile function of the heart;
- ABPM (24-hour blood pressure monitoring): the examination is carried out using a special device. It is attached to the patient's belt and connected to a cuff placed on the shoulder using a thin flexible hose. At certain intervals, the device pumps air into the cuff and measures blood pressure. All research results are stored in the device’s memory. Such measures make it possible to accurately determine changes in pressure during the day and evaluate the effectiveness of treatment;
- X-ray examination of the chest organs: detect pathologies in the lungs, expansion of the cavity of the left ventricle, changes caused by thickening of the walls of blood vessels and a number of other complications;
- Ultrasound examination of the kidneys: makes it possible to track pathological processes caused by the disease;
- examination of the fundus using an ophthalmoscope. The method allows you to identify changes in blood vessels that are a consequence of high blood pressure.
Our clinic performs any type of diagnostics. The experience of doctors and modern medical equipment make it possible to diagnose the disease at an early stage of its development and prevent complications.
Classification of hypertension by stages
The stage of arterial hypertension is determined based on the severity of symptoms and involvement of target organs.
First stage. Symptoms are mild and sometimes completely absent. As a rule, the onset of the disease is signaled only by a slight increase in blood pressure. There is no evidence of end-organ involvement.
Second stage. Symptoms characteristic of hypertension regularly occur, pathological changes in the blood vessels and moderate hypertrophy of the heart muscle are noted, which at this stage does not yet affect the functional state.
Third stage. It is also called the stage of organ changes, since in addition to pronounced symptoms, pathological changes in target organs are noted.
Stages and causes of hypertension development
The classification of the stages of development of essential hypertension is based on the criterion of the boundaries of pressure indicators. In total, it is customary to distinguish 3 types, each of which has its own symptoms and the nature of its effect on the human body.
The latter is characterized by very high blood pressure levels, which is accompanied by negative pathological disturbances in the functioning of vital systems and a decrease in the effect of medications.
The degree of violations that have occurred is determined by measuring indicators; the number of recorded cases is of great importance. What is important is not the one-time fact of recording a deviation from the norm, but the repetition of the event 3 or 4 times a month.
Primary
Primary essential hypertension occurs in 90% of people and is often detected during a medical examination. It is characterized by a slight excess of the following indicators:
- upper no more than 159;
- the bottom ranges from 90 to 99.
With a slight deviation from the norm, the patient does not feel much discomfort and for a long period may not be aware of the occurrence of a problem. The diagnosis is made based on the tonometer points. The first stage is associated with a high risk of various complications due to diabetes or problems with the functioning of internal organs. The high-risk group includes patients with a history of ischemic attacks or a stroke.
Second stage
The stage of progressive hypertension is characterized by a significant increase in blood pressure. Diagnosis criteria:
- upper 160-179;
- lower 100-109.
At stage 2, changes in the vascular walls are diagnosed and signs of hypertrophic changes in the myocardium appear. Such changes are not capable of significantly affecting the condition and functioning of internal organs. If self-treatment is attempted or there is no timely treatment, a person’s condition may worsen, and the disease may progress to the final stage, which is dangerous to health.
Third stage
The stage is considered the most severe, and the indicators are 180/110 or higher. Due to the risk of pathological changes, it is often called the “stage of organ change,” since with a high blood pressure value, pathological changes in the structure of blood vessels and organs are clearly visible. The totality of the nature of the lesion and existing risk factors determines the likelihood of complications.
Treatment of essential hypertension
Treatment tactics will be primarily aimed at eliminating the cause that provoked the disease. In addition, it is important to take into account the age, general condition of the patient and the severity of hypertension.
Drugs
Treatment should begin with small doses, taking into account possible contraindications (which is why the attending physician should prescribe drugs).
Diuretics
Drugs with a diuretic effect are prescribed for hypertension in order to reduce the total volume of fluid circulating in the body and eliminate edema. In addition, diuretics have a direct vasodilatory effect. Most often, thiazide diuretics are prescribed for essential hypertension:
- indapamide
- hydrochlorothiazide.
Loop diuretics have a rapid, pronounced, but short-term effect. Therefore, they are used much less frequently - as a rule, during hypertensive crises, as well as in patients with chronic renal and/or heart failure. The most common drugs in this group:
- furosemide;
- torasemide;
- ethacrynic acid.
Beta blockers
The hypotensive effect when using drugs in this group is achieved primarily by suppressing the activity of beta-adrenaline receptors and the production of renin by the kidneys, which prevents vasospasm and an increase in pressure. Typically, the following drugs are used in the treatment of hypertension:
- propranolol;
- nadolol;
- atenolol;
- metoprolol
Angiotensin-converting enzyme (ACE) inhibitors
These drugs block the work of ACE, which converts biologically inactive angiotensin I into the hormone angiotensin II, which has a pronounced vasoconstrictor effect. This helps to lower the concentration of angiotensin II in the blood, which causes an increase in blood pressure. They also help reduce the secretion of aldosterone and vasopressin, which narrow the lumen of blood vessels. For patients suffering from metabolic syndrome, ACE inhibitors are considered the drugs of choice as they improve lipid and carbohydrate metabolism. For hypertension, the following are indicated:
- captopril;
- enalapril;
- spirapril;
- ramipril
Sartans
The action of sartans (angiotensin II receptor antagonists) is in many ways similar to ACE inhibitors - they block angiotensin receptors. The key difference in the action of these two groups of drugs is that sartans block the final phase of the reaction, when angiotensin tries to cause vasospasm, but the body simply ignores its signals. As a result, this helps to avoid vasospasm and an increase in blood pressure. Preparations:
- candesartan;
- losartan;
- eprosartan;
- valsartan.
Calcium channel blockers
When treating hypertension, calcium receptor blockers help reduce vasospasm, reduce the oxygen demand of the heart muscle and reduce the heart rate.
Important! These are effective but potent drugs, the advisability of which can only be determined by a specialist, since if used incorrectly, calcium receptor blockers can cause cardiac arrhythmias and cardiac arrest.
It is recommended to use the following drugs in this group:
- amlodipine;
- verapamil;
- felodipine;
- nicardipine.
Non-drug treatments
Despite the apparent simplicity of recommendations for lifestyle changes, the importance of non-drug treatment can hardly be overestimated, since it largely determines the effectiveness of the main therapy. That is why it is always prescribed to all patients with hypertension, regardless of the severity of the disease. Only a complex effect will give a noticeable result with a persistent increase in blood pressure.
Basic recommendations:
- Regular dynamic loads. Most often, walking is recommended (at least 30 minutes a day). With moderate severity of hypertension (if the pressure does not exceed 150/100 mm Hg), exercises with free weights (dumbbells or barbell) of medium intensity are allowed, without using maximum working weights.
- Normalization of body weight. If the patient is overweight, then it will be important to get rid of it. This is achieved both by physical exercise and by following a proper diet.
- Minimizing stress. Conflict situations and excessive experiences should be avoided, since the success of treatment will largely depend on this. You also need to sleep at least 8.5 hours a day.
- Rejection of bad habits. Patients who are prone to drinking alcohol and/or smoking need to wean themselves from these habits. A doctor can help with this.
Principles of therapy
Treatment of essential hypertension is aimed at normalizing blood pressure and restoring the functions of affected organs. Therapy should be comprehensive and include mandatory changes in lifestyle, eating habits, and giving up alcohol and smoking.
Antihypertensive drugs
Antihypertensive drugs are prescribed to treat essential hypertension. The medications must be taken strictly as prescribed by the doctor, following the treatment regimen. With regular use of antihypertensive drugs, blood pressure normalizes.
Self-medication with antihypertensive drugs is excluded, as it can lead to a deterioration in general health, serious consequences and complications. The drugs are prescribed in combination or as monotherapy.
For complex therapy of high blood pressure, combined antihypertensive drugs are prescribed:
- diuretics help with the development of a crisis;
- ACE inhibitors reduce the load on internal organs and reduce the likelihood of complications;
- blockers of slow calcium channels relieve vascular tension, vasospasm, they are prescribed for ischemia;
- beta blockers reduce the load on the heart;
- alpha blockers normalize blood flow;
- imidazoline receptor agonists are prescribed for malfunctions of the endocrine system and normalize metabolism;
- Angiotensin 2 receptor antagonists effectively lower blood pressure.
For atherosclerotic vascular disorders, statins, antiplatelet agents, nitrates, and anticoagulants are additionally prescribed. Drug therapy is combined with non-drug methods.
Non-drug treatment
Diet correction
Dietary nutrition for high blood pressure must become part of the life of a patient with high blood pressure. It is necessary to limit daily salt intake to 5 g. The diet involves a complete abstinence from alcohol, coffee, strong tea, and fatty foods.
The diet should be dominated by fruits, vegetables, potassium- and magnesium-containing foods: legumes, buckwheat, oatmeal, nuts, dried fruits, spinach, mushrooms, pumpkin, watermelon, apricots, tomatoes, citruses, seaweed, potatoes, cocoa, bran.
A special diet is recommended for hypertensive patients
Phytotherapy
You can lower your blood pressure with decoctions of valerian, sage, and eucalyptus. For high blood pressure, the following herbs are contraindicated: St. John's wort, eleutherococcus, lemongrass, goat's rue. Herbal medicine is carried out in courses lasting at least a month. You cannot use herbal infusions without a doctor's prescription.
Physiotherapeutic techniques
For essential hypertension, it is recommended to attend electrosonotherapy sessions. Physiotherapy is carried out in a sanatorium or at special resorts.
Basic physiotherapy techniques:
- galvanotherapy;
- electrophoresis;
- low frequency magnetic therapy;
- aromatherapy;
- UHF therapy;
- darsonval;
- laser therapy;
- massage;
- baths.
Treatment of essential hypertension in adults with physiotherapy and herbal medicine is carried out only at the initial stage. In the future, mandatory prescription of medications is required.
Traditional medicine against hypertension
It is quite difficult to draw clear conclusions regarding the effectiveness of traditional methods in the treatment of essential hypertension, since along with safe and effective methods you can find a lot of recommendations that, at best, will be useless.
For example, eating a variety of seeds and nuts is a safe and relatively effective method. These foods contain large amounts of omega-3 fatty acids. Due to this, they help prevent the formation of cholesterol and narrow the lumen of blood vessels.
As for mustard plasters on the shin and other “home-grown” procedures, the advisability of their use should always be discussed with a doctor, since sometimes there are contraindications, and the methods themselves often do more harm than good.
Diet
Source: freepik.com/senivpetro
If you are prone to hypertension, you must first limit the amount of salt consumed (to about 4 g per day). The calorie content of the daily diet should not exceed 2500 kcal for men and 1800 kcal for women. You should give up sweets or at least minimize their consumption. Foods rich in carbohydrates are best consumed in the first half of the day.
Eating before bed is allowed, but in such cases, preference should be given to low-fat protein foods (for example, cottage cheese with yogurt or a small piece of boiled chicken fillet with salad).
Avoid eating spicy, fatty and fried foods. It is important to limit your consumption of coffee, as well as sugary drinks and canned foods.
Recommended products for hypertension:
- lean meats and fish;
- whole grain cereal products;
- low-fat dairy products;
- vegetables, fruits, berries, nuts.
Prevention
Disease prevention measures include:
- correct lifestyle;
- giving up bad habits - smoking and alcohol abuse;
- maintaining a proper diet and nutrition regimen. You should eat more foods containing fiber and minimize fatty, spicy and fried foods;
- physical activity. In this case, we are not talking about the fact that every person should exhaust himself with daily physical activity in the gym. To keep the body normal, it is enough to take daily walks in the fresh air at a moderate pace for thirty minutes;
- regularly undergo preventive medical examinations, during which the patient’s blood pressure level is necessarily measured.
To avoid complications, you need to promptly seek help from the Yusupov Hospital, where the pathology will be diagnosed and treated.
The quality of services provided in the hospital is at the European level. All diagnostic and treatment procedures are performed using the latest medical equipment. The rooms are equipped with maximum comfort for patients.
Do not put off going to the doctor and for any manifestations of increased intracranial pressure, seek help from highly qualified doctors at the Yusupov Hospital. Call by phone and the coordinating doctor will answer all your questions.
Complications of the disease
Complications associated with essential hypertension affect the target organs that we described above - the kidneys, cardiovascular system, brain and eyes.
- Heart: angina pectoris, heart failure, myocardial infarction.
- Central nervous system: stroke, cerebrovascular insufficiency.
- Kidneys: hypertensive nephropathy and renal failure.
- Eyes: retinal damage, hypertensive retinopathy.
- Vascular: In addition to hypertonicity of the peripheral blood vessels, there is a risk of dissecting aortic aneurysm, a condition that can be fatal.
Such complications must be avoided, as they can significantly impair the quality of life. To do this, it is important to comply with the doctor’s requirements regarding taking medications, adjusting your diet and lifestyle.
Symptoms
The disease can be benign or malignant. In the first case, the patient’s blood pressure level increases infrequently, and after taking antihypertensive drugs it quickly returns to normal. The malignant form of the disease is distinguished by the fact that blood pressure rises significantly and frequently, the patient quickly develops damage to internal organs, and medications are usually ineffective.
A long asymptomatic course of the disease is possible. Before complications develop, the only symptom of the disease is often high blood pressure, manifested by headache.
The main clinical sign of the pathology is headache of varying intensity - from a feeling of a “heavy head” to extremely intense. The pain is usually localized in the back of the head, accompanied by tinnitus and spots in front of the eyes.
The symptoms are especially pronounced during a hypertensive crisis. This is a condition caused by a rapid and significant increase in pressure, manifested by intense headache, dizziness, nausea, vomiting, pain in the heart, and weakness.
As the pathological process progresses and target organ damage occurs, patients may experience signs of coronary heart disease, hypertensive encephalopathy, and intermittent claudication.
Sources
- Miazgowski T., Miazgowski B., Kaczmarkiewicz A., Kopeć J. Associations of circulating irisin with 24-h blood pressure, total and visceral fat, and metabolic parameters in young adult hypertensives. // Arch Endocrinol Metab - 2021 - Vol - NNULL - p.; PMID:33905629
- Volnuhin AV., Siburina TA., Knyazev AA. . // Probl Sotsialnoi Gig Zdravookhranenniiai Istor Med - 2021 - Vol29 - N2 - p.306-312; PMID:33901373
- Trubetskov AD., Zhyrov KS. [“The effect of healthy worker” in various areas of occupational medicine: the publications review]. // Probl Sotsialnoi Gig Zdravookhranenniiai Istor Med - 2021 - Vol29 - N2 - p.254-259; PMID:33901364
- Alfieri F., Ancona A., Tripepi G., Crosetto D., Randazzo V., Paviglianiti A., Pasero E., Vecchi L., Cauda V., Fagugli RM. A deep-learning model to continuously predict severe acute kidney injury based on urine output changes in critically ill patients. // J Nephrol - 2021 - Vol - NNULL - p.; PMID:33900581
- Cao N., Tang H., Tian M., Gong X., Xu Z., Zhou B., Lan C., Chen C., Qu S., Zheng S., Ren H., Fan C., Jose PA ., Zeng C., Xia T. Genetic variants of GRK4 influence circadian rhythm of blood pressure and response to candesartan in hypertensive patients. // Clin Exp Hypertens - 2021 - Vol - NNULL - p.1-7; PMID:33899625
- Weinstein S., Leibowitz A. . // Harefuah - 2021 - Vol160 - N4 - p.256-259; PMID:33899377
- Wang AP., Yang F., Tian Y., Su JH., Gu Q., Chen W., Gong SX., Ma XF., Qin XP., Jiang ZS. Pulmonary Artery Smooth Muscle Cell Senescence Promotes the Proliferation of PASMCs by Paracrine IL-6 in Hypoxia-Induced Pulmonary Hypertension. // Front Physiol - 2021 - Vol12 - NNULL - p.656139; PMID:33897463
- Ansbro E., Homan T., Qasem J., Bil K., Rasoul Tarawneh M., Roberts B., Perel P., Jobanputra K. MSF experiences of providing multidisciplinary primary level NCD care for Syrian refugees and the host population in Jordan : an implementation study guided by the RE-AIM framework. // BMC Health Serv Res - 2021 - Vol21 - N1 - p.381; PMID:33896418
- Hieda S., Ishimaru N., Ohnishi J., Mizuki S., Kanzawa Y., Kawano K., Nakajima T., Kinami S. Posterior reversible encephalopathy syndrome complicating hyperosmolar hyperglycemic syndrome. // Am J Emerg Med - 2021 - Vol - NNULL - p.; PMID:33895041
- Pierre Niyonsenga S., Park PH., Ngoga G., Ntaganda E., Kateera F., Gupta N., Rwagasore E., Rwunganira S., Munyarugo A., Mutumbira C., Dusabayezu S., Eagan A., Boudreaux C., Noble C., Aimee Muhimpundu M., Gilles Ndayisaba F., Nsanzimana S., Bukhman G., Uwinkindi F. Implementation outcomes of national decentralization of integrated outpatient services for severe non-communicable diseases to district hospitals in Rwanda. // Trop Med Int Health - 2021 - Vol - NNULL - p.; PMID:33892521