Allergic vasculitis is an inflammatory disease of the walls of blood vessels that occurs as a result of an allergic reaction. Allergic vasculitis can have many varieties, some of which damage individual organs, while others spread to their entire systems. With allergic vasculitis of the skin, the inflammatory process affects the vessels that are located in the subcutaneous tissue (as a rule, without involving the vessels of the internal organs in the process).
Both adults and children are susceptible to it, regardless of age.
Symptoms of the disease.
Allergic skin vasculitis (depending on the depth of the damaging process) is divided into:
- Superficial
- Deep
Symptoms of allergic skin vasculitis:
- Purpura – vascular spots in areas of hemorrhage
- Ulcers
- Vascular spots
- Papules are pink nodular lumps of skin
- Bubbles with a diameter greater than 5 mm
- Subcutaneous nodes
- Chronic urticaria
- Rash
All of the above symptoms are usually accompanied by general malaise, loss of appetite, itching and burning of the skin, fever and increased temperature.
Symptoms
There are many types of vasculitis known. They all have their own characteristics and symptoms. The most common types of this disease:
1. Periarteritis nodosa (small and medium arteries). The disease threatens stroke and mental disorders. More often diagnosed in men. Characterized by:
- muscle pain;
- elevated temperature;
- losing weight;
- abdominal pain;
- vomiting and nausea.
2. Wegener's granulomatosis (vessels of the respiratory system and then the kidneys).
Symptoms:
- sinus pain;
- nasal discharge with pus and blood;
- ulcers on the nasal mucosa;
- destruction of the nasal septum, change in the shape of the nose;
- cough (sometimes with blood);
- chest pain;
- renal failure.
3. Giant cell temporal arteritis (large vessels, most often the head). It mainly affects people of retirement age. Symptoms:
- undulating fever;
- weakness;
- weight loss;
- severe pain in the head of a pulsating nature, aggravated by chewing;
- swelling in the temple area.
4. Tokayasu disease (large arteries and aorta). Signs:
- numbness, pain in the arms and legs;
- pain in the back, stomach, etc.;
- fainting;
- blurred vision.
Specialists.
List of specialists who should be contacted for diagnosis and treatment of allergic vasculitis:
- Allergist
- Immunologist
- Therapist
Additionally, the doctor can refer the patient for a consultation with specialized specialists: a dermatologist, vascular surgeon, venereologist, rheumatologist, etc.
To diagnose, treat and prevent this disease, we invite you to the clinic of the Central Clinical Hospital of the Russian Academy of Sciences, where you can undergo all the necessary examinations.
Treatment of vasculitis
Conservative therapy for vasculitis is aimed at suppressing pathological autoimmune reactions with the production of antibodies. It is carried out in stages:
- relief of symptoms and achievement of remission;
- maintaining remission for 0.5–2 years;
- treatment of relapses.
In addition, prevention or elimination of concomitant diseases and complications is carried out.
The treatment regimen is based on the drugs of choice:
- hormones – for giant cell arteritis of GCA, polymyalgia rheumatica and Takayasu’s disease;
- hormones and cytostatics - for systemic, hemorrhagic and cryoglobulinemic vasculitis, polyarteritis nodosa and a number of others;
- immunosuppressants with hormones - for hemorrhagic vasculitis, if combination therapy with cytostatics is not effective;
- monoclonal antibodies - for systemic vasculitis, if combination therapy is not effective;
- basic antirheumatic drugs – in case of contraindications to the drugs of choice;
- immunoglobulins - for severe complications.
Diet therapy is also indicated . For functional kidney damage, plasmapheresis or hemosorption - hardware blood purification - are prescribed. In addition, according to indications, antiviral and symptomatic agents, antibiotics, drugs to maintain cardiac activity and prevent blood clotting are prescribed.
Conservative treatment of vasculitis is complex and long-term. In some forms, against the background of overgrowth, spasms and thrombosis of large vessels, surgical treatment is indicated. Without timely and correct treatment of vasculitis in children, the prognosis is unfavorable. The nature of the consequences depends on the type of disease.
Sources:
- https://academic.oup.com/ndt/article/30/suppl_1/i94/2324852 Despina Eleftheriou, Ezgi Deniz Batu, Seza Ozen, Paul A. Brogan. Vasculitis in children // Nephrology Dialysis Transplantation, Volume 30, Issue suppl_1, 1 April 2015, Pages i94–i103.
- E.V. Borisova. Hemorrhagic vasculitis in children // Pediatrics, No. 6, 2004, pp. 51-56.
- AND I. Lutfullin. Kawasaki syndrome: clinical algorithms and the problem of underdiagnosis of the disease // Bulletin of modern clinical medicine, 2021, vol. 9, issue 2, 52-60/
The information in this article is provided for reference purposes and does not replace advice from a qualified professional. Don't self-medicate! At the first signs of illness, you should consult a doctor.
Treatment.
Allergic vasculitis must be treated comprehensively.
- It is necessary to identify the allergen and eliminate its effect on the body (stop taking the medicine, some product, etc.)
- Take antihistamines.
- In case of acute illness, bed rest must be observed.
- Drink plenty of fluids and follow a strict diet, including the required amount of vegetables, protein foods and fruits, with the exception of those that can cause allergies (nuts, red fish, chocolate, citrus fruits, honey, etc.).
- If a chronic infection is detected, antibacterial drugs are prescribed.
- To strengthen the walls of blood vessels, vascular protectors are prescribed.
- To treat allergic skin vasculitis, it is possible to use external medicinal products (creams and ointments as prescribed by a doctor).
Classification of the disease
Vasculitis is classified based on etiology, pathogenesis, type of vessels affected and the nature of the rash. Genetic and demographic factors, clinical manifestations and predominant lesions of internal organs are also taken into account.
Based on the factors preceding the disease, primary and secondary vasculitis are distinguished. Primary - caused by inflammation of the vascular wall, secondary - in which vascular inflammation is a reaction to another disease (lupus erythematosus, rheumatism, diabetes mellitus, granulomatosis, sarcoidosis, hepatitis).
according to the diameter of the affected vessels :
- small vessels - affects capillaries and venules, arterioles and small arteries of internal organs;
- middle vessels - mainly affects the abdominal arteries and their branches. Often cause stenoses and aneurysms;
- large vessels - affect the aorta and its main branches.
In addition, there are groups of vasculitis :
- small vessels with immune complexes;
- with trigger connective tissue diseases;
- with an established etiology of a metabolic or infectious nature;
- with damage to one organ.
Hemorrhagic vasculitis against the background of actively persistent herpesvirus infections
Angiitis or vasculitis in children is a primary or secondary inflammation of the walls of blood vessels.
Primary systemic vasculitis is a group of diseases characterized by damage to the walls of vessels of various sizes (from the microvasculature to the aorta and its branches) by the type of focal inflammation and necrosis, with subsequent involvement of organs and tissues in the area of vascular damage in the pathological process.
Secondary vasculitis develops in infectious, autoimmune, rheumatic, oncohematological and other diseases [1, 2].
The etiology of most primary vasculitis is unknown. It is believed that their occurrence in a child can be facilitated by frequent acute infectious diseases, foci of chronic infection, drug allergies, and a hereditary predisposition to vascular or rheumatic diseases. Bacterial or viral infections (streptococcal, herpesvirus, parvovirus, hepatitis B or C), on the one hand, allergies or a burdened allergic history. on the other hand, according to experts, they serve as two equal factors that form the background for hypersensitization of the body or act as trigger, provoking factors.
It has now been established that Epstein-Barr virus infection (EBV) and human herpes type 6 infection are associated with a number of autoimmune diseases (classical rheumatic diseases, vasculitis, ulcerative colitis, etc.). It is known that human herpes virus type 6 in children during primary infection and during its reactivation causes erythema infectiosum with symptoms of vasculitis, which is observed 3 times more often than with EBV and cytomegalovirus infection (CMV) [3–5].
These viruses can cause chronic manifest and latent forms of the disease, similar to chronic mononucleosis. Moreover, the development of an autoimmune disease can manifest itself after a long period of time after infection.
Herpetic infection is histologically manifested by the deposition of fibrin in microvessels, while the surface conformation of the endothelium changes; on the infected endothelium, the level of thrombin production increases 2–3 times, tissue expression of thrombomodulin and activation of protein C decreases (GM Vercelotti, 1990).
Changes in the area of the damaged area of the vessel are varied - from ischemia to hemorrhage, necrosis, and infarction. The degree of vascular disorders depends on the caliber of the affected arteries and the state of collateral circulation [2].
Of great importance in the development of vasculitis are the formation, circulation and deposition on the walls of blood vessels of immune complexes, antineutrophil cytoplasmic antibodies, immune proliferative-destructive inflammation of the walls of arteries of various calibers, damage to the vascular endothelium, increased vascular permeability, hypercoagulation with impaired blood flow, ischemia in the area of vascular damage.
In the initial period of vasculitis, general manifestations of a nonspecific inflammatory syndrome are observed: low-grade or febrile fever, arthralgia, weight loss, symptoms of peripheral and visceral vascular disorders, moderate anemia, leukocytosis in peripheral blood, increased ESR, signs of hypercoagulation, dysproteinemia, increased levels of C-reactive protein, IgA, circulating immune complexes and cryoglobulins [2].
The originality of clinical manifestations is due to the localization of vasculitis, the caliber of the affected vessels, the prevalence of the pathological process, the characteristics of morphological changes (the predominance of destructive or proliferative processes), the degree of hemodynamic disorders and ischemia of organs and tissues.
The vascular genesis of massive hemorrhages and necrosis in herpesvirus encephalitis has been proven. Clear evidence of morphological changes in vessels that can be visualized intravitally during these infections is the data of foreign and domestic researchers, indicating the development of coronaritis after acute and, more often, against the background of chronic EBV infection, as well as systemic vasculitis (Kawasaki syndrome). Coronary lesions were found in 55% of children who had EBV infectious mononucleosis with a fever duration of more than 5 days.
It is known that during herpesvirus infection, the ability of viruses to have a cytopathic effect, exhibiting tropism for blood vessels, is important. Vascular damage in EBV is recorded in 7–30%, and in CMV in 8% [4, 6–8].
Human herpes virus type 6 in children during primary infection and during its reactivation causes erythema infectiosum with symptoms of vasculitis, which is observed 3 times more often than with EBV and CMV infections.
For several years, the authors studied the frequency of occurrence and clinical manifestations of vasculitis syndrome in children with various variants of the course of herpesvirus infections. The studies were conducted in 202 patients aged from one year to 14 years, of which 160 children with infectious mononucleosis (IM) and 42 with vasculitis syndrome without signs of myocardial infarction, who were in the somatic and infectious departments of the Morozov City Children's Clinical Hospital in Moscow .
In addition, an ultrasound examination assessed the state of the intima-media complex and the state of the vessels of the head and cervical region in 20 children aged 6 months to 14 years with actively persistent herpesvirus infections (EBV, CMV and HHV type 6 without signs of MI) in the multidisciplinary clinic Vessel Clinic.
In clinical and laboratory monitoring of patients, the following studies were carried out:
- general tests of peripheral blood, urine, blood biochemistry, coagulogram;
- bacteriological studies of microbiocenosis of the oropharynx, intestines, parasitic infections, helminths;
- serological studies were carried out using the following methods: immunofluorescence reaction (IF) to respiratory viruses and RIF with monoclonal antibodies to CMV proteins pp 65, pp 72;
- indirect immunofluorescence reaction (IRIF) to herpesvirus antigens in blood cells and enzyme-linked immunosorbent assay (ELISA) for herpesviruses 1, 2, 4, 5 and 6; mycoplasma, chlamydia, parvovirus type 19, etc.;
- polymerase chain reaction (PCR) for DNA of EBV, CMV, HSV type 1, HSV type 2; HHV type 6 in blood, saliva and urine.
Manifestations of vasculitis occurred in all etiological variants of MI in the form of a maculopapular or maculopapular rash with a hemorrhagic component, which was more often regarded as toxic-allergic in patients receiving aminopenicillin antibiotics and less often in those who did not receive such drugs (Fig. 1, 2 ).
Manifestations of vasculitis in the form of a hemorrhagic rash, similar to skin purpura, with signs of thrombovasculitis were observed in the majority of patients suffering from actively persistent herpesvirus infection without signs of infectious mononucleosis, while the rash did not have a localization characteristic of hemorrhagic vasculitis (of the Schönlein–Henoch type), the elements of which appeared on various areas of the skin: in the chest, abdomen, back, armpit, legs, which spread against the background of fever and then subsided. Pigmentation appeared in the areas of the rash in some patients.
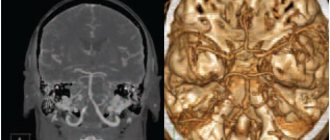
Duplex scanning of the vessels of the head and neck with actively persistent herpesvirus infections revealed ECHO signs of obstruction of venous outflow or vasospasm of the arteries of the circle of Willis, with obvious compaction of the intima-media complex (IMC) of the vessels, which indirectly indicated endothelial dysfunction, which most likely developed in as a result of long-term cytopathic effects on the vascular endothelium directly from actively persistent herpes viruses.
As a clinical example, the medical history of the child Elizaveta S., 2 years 11 months (born October 28, 2010) is presented.
The condition upon admission was severe. Body temperature - 37.2? C. The skin is pale, on the skin of the lower extremities there is a maculopapular rash with hemorrhagic impregnation, elements of different sizes that tend to merge on the feet, several elements on the upper extremities, in the elbow area.
Angioedema of the left foot, right hand, movement in the right ankle joint is difficult.
The pharynx is hyperemic, the tonsils have no plaque. Anterior and posterior cervical, submandibular lymph nodes up to 2 cm, painless, not fused with surrounding tissues.
There are no visible pathologies in other organs.
Ultrasound of the abdominal organs, kidneys, spleen from October 24, 2013: ECHO signs of moderate hepatomegaly, mesadenitis.
In other organs there were no pronounced structural changes or pathological inclusions.
Examination by an ENT doctor on October 24, 2013 - diagnosis: left-sided acute catarrhal otitis media.
The results of blood tests are presented in tables 1–3.
During his stay in the department, three waves of rashes were observed with large hemorrhagic confluent elements in the femoral and popliteal areas of both extremities and angioedema (Fig. 3).
Clinical diagnosis: hemorrhagic vasculitis, mixed form (cutaneous-articular syndrome), occurring against the background of reactivation of a mixed persistent herpesvirus infection EBV, HHV type 6 and bacterial infection.
It is recommended to include glucocorticoids and Viferon 1 million in suppositories in the treatment.
Treatment performed:
- Box mode.
- Table 15.
- Ceftriaxone 550 ml 2 times a day intravenously 10/25/2013–10/30/2013
- Suprastin 0.3 2 times a day with saline solution IV.
- Bifidumbacterin 5 doses 3 times a day by mouth.
- Prednisolone 25 mg IV at 10:00 from 10/25/2013–10/28/2013
- Prednisolone 3 times a day, by mouth after breakfast - 10 mg, after lunch - 7.5 mg, after dinner - 5 mg from October 31, 2013.
- Heparin 0.3 subcutaneously 6:00, 14:00, 22:00 from 10/25/2013–11/2013
- Curantil 25 mg tablets 3 times a day by mouth from 10/25/2013–11/2013.
- Irrigation of the pharynx with Miramistin 3 times a day.
- Toilet the nose with saline solution 3 times a day.
- Naphthyzin 0.05% 1 drop 3 times a day in the nose.
- Otipax 3 drops 3 times a day in the left ear.
- Mucaltin 1 tablet 3 times a day by mouth.
- Viferon 500,000 suppositories once a day rectally.
- Losek 5 mg 2 times a day, by mouth 30 minutes before meals, at night from 10/31/2013–11/2013.
- Infusion therapy.
The child's condition at discharge was satisfactory. Doesn't have a fever. Catarrhal phenomena stopped. The skin is clean. The pharynx is loose. The breathing in the lungs is puerile, there is no wheezing. Heart sounds of moderate volume, rhythmic. The abdomen is soft and painless. Stool and urine output are normal. There are no meningeal signs. The child was discharged home with improvement under the supervision of a local pediatrician.
Thus, in the practical work of a pediatric infectious disease specialist or family doctor, it is necessary to determine markers of active replication of herpetic viruses of types 4, 5 and 6 not only in patients with typical clinical manifestations of infectious mononucleosis, in long-term feverish, often ill patients; in children with lymphadenopathy, but also with vasculitis syndrome in order to clarify the trigger factors for its development, as well as to prevent the often unjustified and long-term prescription of antibiotics for MI and to justify adequate antiviral therapy.
Treatment is prescribed taking into account the nosological diagnosis, the phase of the disease and its clinical features.
The choice of treatment methods for vasculitis involves influencing the possible cause and underlying mechanisms of disease development. Impact on the trigger infectious agent, suppression of immune inflammation by prescribing anti-inflammatory and immunosuppressive drugs: glucocorticoids (prednisolone, methylprednisolone), cytostatics (cyclophosphamide, methotrexate).
Removal of antigens and circulating immune complexes using intravenous administration of antibodies, plasmapheresis synchronously with pulse therapy with glucocorticoids and/or cytostatics. Correction of hemostasis: prescription of anticoagulants, antiplatelet agents. Symptomatic therapy.
The effect of treatment is assessed by the dynamics of clinical syndromes and laboratory parameters. Treatment in the acute phase of the disease is carried out in a hospital, then continues on an outpatient basis with mandatory dispensary observation and control.
Literature
- Lyskina G. A. Systemic vasculitis. In the book: Pediatric rheumatology. Guide for doctors / Ed. A. A. Baranova, L. K. Bazhenova. M.: Medicine, 2002. pp. 221–270.
- Vanhoutte PM, Mombouli JV Vascular endothelium: vasoactive mediators // Prog. Cardiovasc. Dis. 1996. V. 39. R. 229–238.
- Yamashita S., Murakami C., Izumi Y. Severe chronic active Epstein-Barr virus infection accompanied by virus-associated hemophagocytic syndrome, cerebellar ataxia and encephalitis // Psychiatry Clin. Neurosci. 1998. Aug; 52(4):449–452.
- Kragsbjerg P. Chronic active mononucleosis // Scand. J. Infect. Dis. 1997. 29 (5): 517–518.
- Okano M. Epstein-Barr virus infection and its role in the expanding spectrum of human diseases // Acta Paediatr. 1998. Jan; 87 (1): 11–18.
- Tolstikova T.V., Bregel L.V., Kiklevich V.T., Subbotin V.M. Coronaritis in children // Sib. honey. magazine 2009. No. 2. P. 67–69.
- Nakagawa A., Ito M., Iwaki T. et al. Chronic active Epstein-Barr virus infection with giant coronary aneurysms // Am. J. Clin. Pathol. 1996. Vol. 105. N6. P. 733–736.
- Egorova O.N., Balabanova R.M., Chuvirov G.N. The significance of antibodies to herpetic viruses determined in patients with rheumatic diseases // Therapeutic archive. 1998. No. 70 (5). pp. 41–45.
F. S. Kharlamova*, 1, Doctor of Medical Sciences, Professor N. Yu. Egorova*, Candidate of Medical Sciences O. V. Shamsheva*, Doctor of Medical Sciences, Professor N. L. Waltz** A. V. Denisova** *
* GBOU VPO RNIMU im. N. I. Pirogova Ministry of Health of the Russian Federation, Moscow ** Morozovskaya State Budgetary Institution of Children's City Clinical Hospital of the Department of Health of the Russian Federation, Moscow *** Vessel Clinic, Moscow
1 Contact information
2. Reasons
Allergic arteriolitis is considered a polyetiological disease, the causes and risk factors of which include acute and chronic infections (and the localization of the trigger focus can be almost any, but more often it is the nasopharynx and/or oral cavity), as well as circulatory disorders, for example, with varicose veins or chronic heart failure. Some authors describe the mechanism of development of Reiter's vasculitis as infectious-allergic, others emphasize the role of immune or autoimmune factors.
Visit our Allergology page
Diagnostics
Since the disease can occur individually in each patient, the variety of clinical symptoms requires the collection of a detailed history, laboratory tests, and sometimes histological analyzes of the elements of the rash and skin are necessary. It is important to notice in time an increase in immunoglobulin E (IgE) due to the formation of immune complexes on the vascular wall.
After scratching the allergic rash and bursting the blisters, accompanying pathogenic bacteria may join. To determine their type, the method of inoculation on a Petri dish is used, and the level of sensitivity to various antibiotics is also established.
What are the risk factors for the disease?
The cause of allergic vasculitis can easily be dangerous infections that are caused by one of the following pathogens or factors:
- streptococcus;
- α1-antitrypsin deficiency;
- leprosy;
- HIV infection;
- hepatitis A, and;
- staphylococcus;
- influenza virus;
- primary biliary cirrhosis of the liver;
- diabetes mellitus type 2;
- Koch bacillus (tuberculosis);
- gout;
- exposure to radiation;
- regular colds, sinusitis and ARVI;
- fibrosis of the retroperitoneal space;
- herpes virus;
- relapsing polychondritis;
- excess weight.
At risk are people with food allergies, patients taking antibiotics, contraceptives (from the oral category) and large doses of vitamins. The disease is also dangerous for those who work with chemical industry products - detergents, antiseptics, gasoline and other petroleum products.
Prevention
All children suffering from vasculitis are registered at the dispensary and undergo regular examinations by a rheumatologist. First every month, and then once every 3 months. Such regularity of visits is necessary in order to prevent possible exacerbations.
All parents have the power to protect their child from vasculitis. To do this, you need to closely monitor the baby’s health, promptly treat all infections from qualified specialists, and under no circumstances resort to self-treatment. You can protect your child from serious illness through vaccination.
Classification
Today there is no unified classification of skin vasculitis. These include several dozen dermatoses that have clinical similarities. The simplest division is related to the source of the disease.
- Primary vasculitis is an independent disease caused by the direct action of an allergen: medicine, intoxication, food, hypothermia or, conversely, prolonged exposure to the sun. For example, toxic-allergic vasculitis, which manifests itself as a reaction to the action of a substance. Treatment in such cases comes down to stopping contact with the allergen.
- Secondary - occurs as a result of some diseases, for example, rheumatic.
The following type of classification is based on the degree and depth of vascular damage in tissues and organs:
| Dermal form, or vasculitis of the skin | Affects mainly small vessels located in the upper layers of the dermis. The mildest form, which causes virtually no complications with timely treatment. |
| Dermo-hypodermal form | Damage to the vessels of the dermis, reaching the deep layers. Sometimes small vessels of soft tissues are affected. |
| Hypodermal form | It is characterized by damage to large vessels - veins and arteries. One of the most dangerous variants of the disease, requiring hospital treatment. |
When it comes to skin lesions, the following types are distinguished:
- rheumatic (systemic) – directly related to lupus and arthritis;
- hemorrhagic (synonyms used in the medical field - anaphylactic purpura, Henoch-Schönlein disease, sometimes called capillary toxicosis);
- polymorphic vasculitis (doctors call it Ruiter's allergic arteriolitis);
- leukocytoclastic - breakdown of leukocyte nuclei, detected by histological examination;
- urticarial vasculitis (in medical circles known as necrotizing urticarial vasculitis);
- papulo-necrotic vasculitis (a disease similar to Werther-Dümling syndrome);
- giant cell – leads to severe damage to large arteries;
- granulomatous - granules form inside the vessels, slowing down or stopping the flow of blood;
- vasculitis nodosum (erythema nodosum, rarely caused by medications);
- nodular-ulcerative vasculitis (three times the name is chronic erythema nodosum).
Diagnosis of vasculitis is based not so much on recording symptoms, but on assessing the rate of change. A histological examination of the affected area and consultation with the necessary specialists are mandatory.
Vasculitis in children
Vasculitis in children is a rather rare phenomenon, but all varieties have characteristic features that are characteristic only of childhood.
Kawasaki syndrome
A systemic form of the disease in children under 7 years of age with damage to the heart vessels, lymph nodes, and respiratory tract mucosa. The clinical picture is characterized by a rapid, acute onset with a temperature of 38 to 41 degrees and the following symptoms (in order of gradual appearance):
- debilitating fever;
- skin lesions with a scarlet-like rash with erythematous plaques;
- damage to the mucous membranes of the respiratory tract, nose, eyes;
- thickening and redness of the skin on the soles and palms of the hands;
- enlarged lymph nodes in the neck;
- crimson tongue color;
- peeling of the skin around the nails, on the phalanges of the fingers;
- damage to the cardiovascular system in the acute phase, aneurysm.
Kawasaki syndrome can be cured with timely diagnosis, the consequences are eliminated after 5-8 years.
Hemorrhagic vasculitis
While hemorrhagic vasculitis in adults can be caused by pathologies during pregnancy, diabetic nephropathy, liver cirrhosis, malignant neoplasms, the cause of this form of the disease in children is most often upper respiratory tract infections, measles, paratyphoid fever, drug or food allergies.
Hemorrhagic vasculitis in children is divided into the following forms: cutaneous, cutaneous-articular, abdominal, renal and cutaneous-renal. Each of them has specific symptoms:
- skin form - severe swelling against the background of cold urticaria, purpura, rash localized on the feet, legs gradually spreading to the hips, pain in the joints;
- abdominal form: severe with severe abdominal pain localized near the navel;
- renal form - the presence of proteins and globulins in the urine.
Hemorrhagic vasculitis is dangerous due to complications, relapses and a tendency to generalization - spreading to the vessels of internal organs.