Briefly about the treatment method
Angioplasty and stenting of the celiac trunk and mesenteric arteries is used to treat the syndrome of chronic intestinal circulatory disorder (angina abdomenalis) or for emergency surgery for acute intestinal circulatory disorder (mesenteric thrombosis).
Intestinal circulatory disorders are rarely diagnosed without a specific focus on certain complaints and are often diagnosed by an experienced clinician only after excluding other causes of abdominal pain.
Previously, when identifying narrowing of the celiac trunk or mesenteric arteries, surgeons adhered to a conservative wait-and-see approach, since open operations on these arteries are very complex and difficult for patients to tolerate. Now, thanks to the development of endovascular technologies, it has become possible to eliminate problems with visceral arteries in a low-traumatic manner.
Celiac stenosis (Dunbar syndrome) - symptoms and treatment
Treatment of stenosis can be conservative or surgical. The first option is possible at the stage of compensation and subcompensation. It is aimed at relieving symptoms. If conservative therapy is ineffective, the patient is prescribed surgical treatment.
Conservative therapy
Conservative treatment does not affect the underlying cause of the disease. It is purely symptomatic or aimed at concomitant diseases: hiatal hernia or cholelithiasis.
Various medications are used as symptomatic treatment :
- gastroprotectors - protect and restore the gastric mucosa;
- enveloping drugs - used for the same purpose immediately before meals;
- prokinetics - have a positive effect on gastric motility, prescribed for nausea while eating or gastroesophageal reflux (GERD);
- antispasmodics - affect smooth muscles, reducing pain;
- non-steroidal anti-inflammatory drugs (NSAIDs) - used for pain relief.
The next important point of conservative treatment is a gentle diet . It is important to exclude spicy, fatty and fried foods from your diet. To reduce the load on the stomach, it is recommended to eat in small portions. It is also important to avoid stress and excessive physical activity. All this helps reduce the intensity of pain after eating.
Some clinics include psychotherapy and acupuncture in complex treatment [16]. The latter treatment method does not have an unconditional evidence base, but many practitioners note its effectiveness in complex therapy.
If conservative treatment does not help, the question of surgery arises.
Surgical treatment
To find out whether a patient needs surgery, the doctor must determine the clinical stage of the disease, the severity of symptoms, the frequency of their occurrence and evaluate the results of the examination: ultrasound or CT angiography.
Then you need to choose a method of surgical treatment:
- open or laparoscopic decompression of the celiac trunk [7];
- reconstructive surgery;
- endovascular surgery;
- hybrid surgical treatment.
Open surgery is the most common method of surgical treatment. To get to the celiac trunk, the doctor dissects the abdominal wall, and then the structures pressing on it: the median arcuate ligament of the diaphragm and the tissue of the celiac plexus.
This operation is effective, but quite traumatic. After the intervention, the body recovers in about three months. Ventral hernias can form, in which internal organs are displaced outward. Sometimes stenosis developed again [17].
Laparoscopic decompression of the celiac trunk in terms of the technique of execution is not fundamentally different from open surgery. The difference is a less traumatic (minimally invasive) access and convenient display of the intervention area, which is visible to the entire operating team.
The pain in the wound after such an operation is less pronounced, the patient recovers faster: on average, he is in the hospital for 4–5 days under the supervision of a doctor, and after 3–4 weeks he returns to normal life and usual activities.
The American surgeon S. Roayaie was the first to report successful laparoscopic decompression of the celiac trunk in 2000 [19]. Since then, many surgeons have mastered this technique, but so far it has not been able to “displace” open decompression. This is due to technical difficulties during the operation and the adherence of older surgeons to the traditional, more familiar technique.
Reconstructive surgeries are recommended for severe changes that do not allow the celiac trunk to be freed from compressive tissue. They are performed by vascular surgeons in specialized centers. Doctors perform plastic surgery of the celiac trunk or replace it with a graft - artificial or natural, that is, another vessel. These operations are performed in an open manner and are tolerated by the patient in the same way as open decompression of the celiac trunk.
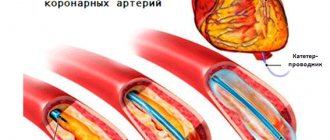
Endovascular surgery is recommended for patients over 60 years of age whose arteries are narrowed by atherosclerotic plaques. The celiac trunk is expanded using a balloon dilator or stent [18]. Both options can be performed only after preliminary surgical decompression [12].
Although endovascular operations are the most minimally invasive method of treatment, they are accompanied by certain risks: deformation, fracture, migration of stents or thrombosis of the stented artery.
Hybrid (combined) treatment is carried out if the celiac trunk is narrowed both from the inside and from the outside. It consists of the simultaneous or step-by-step implementation of two treatment methods: decompression of the celiac trunk and installation of a stent [18].
After endovascular and reconstructive operations, you need to be observed by a vascular surgeon and constantly take blood thinning medications. Dosage regimens depend on the operation performed. These mandatory measures will help avoid re-stenosis.
Advantages of treatment at the ISC
In case of pathology of the celiac trunk and superior mesenteric artery, our x-ray surgeons can perform angioplasty and stenting of narrowings of these significant arteries. The most commonly used approach is the brachial or radial artery.
In the presence of thrombosis of the mesenteric artery or celiac trunk, our clinic performs thrombectomy operations using a special Rotarex probe or selective thrombolysis. Once blood flow is restored, we perform angioplasty and stenting.
Causes of narrowing of the celiac trunk and diagnosis using duplex ultrasound scanning
Scientific interest in determining the information content of non-invasive research methods is due to the search for accessible, inexpensive methods for diagnosing and predicting organic and functional diseases of internal organs. When the visceral branches of the abdominal aorta are damaged, clinical signs characteristic of diseases of the gastroduodenal region, gall bladder, pancreas and intestines appear. In patients with diseases in this area, organic and functional changes in organs are diagnosed and treatment is carried out, despite the recurrence of symptoms of exacerbation of the disease. Study of blood flow in unpaired visceral branches of the abdominal aorta
(NVVA) - the celiac trunk, superior and inferior mesenteric arteries - often makes it possible to establish the cause of organ dysfunction and select adequate effective treatment methods. Ultrasound examinations performed on modern equipment using Doppler techniques are a new methodology for visualizing the vessels of the abdominal cavity, allowing one to study the anatomical features and blood flow throughout the arteriovenous bed and expand the possibilities for diagnosing diseases of the gastroduodenal region.
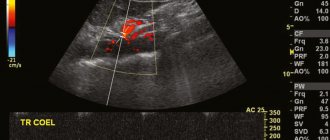
With ultrasound duplex scanning
visualize the abdominal aorta, the initial sections of the celiac trunk and its branches (common hepatic and splenic arteries), as well as the superior and inferior mesenteric arteries. The study allows you to evaluate the size of the vessels, the expansion or narrowing of their lumen, changes in wall thickness and the intima-to-media ratio, aneurysmal protrusions, the presence of atherosclerotic plaques, as well as study the speed and nature of blood flow.
To the main signs caused by circulatory disorders
in the unpaired visceral branches of the abdominal aorta, include the following:
- complete absence of blood flow in case of vascular occlusion,
- decreased blood flow velocity distal to the site of stenosis,
- increased blood flow velocity directly at the site of stenosis and turbulence at the mouth of the vessel,
- identification of collateral blood flow with the opposite blood flow during occlusion of a great vessel,
- reduction in the diameter of the affected vessel,
- post-stenotic expansion.
Using different positions of the sensor, the abdominal aorta and its unpaired visceral branches are visualized from the anterior abdominal approach in the longitudinal and transverse plane. To obtain a longitudinal image of the abdominal aorta, the sensor is placed to the left of the midline of the body along the vertical axis of the body, orienting the scanning plane perpendicular to the anterior abdominal wall and directed towards the spinal column with the patient in the supine position. The scan is performed below the xiphoid process by 1-2 cm, moving the sensor in the caudal direction. To obtain a cross-section of the abdominal aorta, the transducer must be oriented perpendicular to the left paramedian line.
Abdominal aorta
during ultrasound examination it looks like a tubular pulsating structure with even, smooth walls and a homogeneous anechoic lumen. The diameter of the aorta below the diaphragm is 25-28 mm, at the level of the visceral arteries - 20-24 mm. On Doppler examination, blood flow in the aorta corresponds to the main type with the presence of an acute systolic antegrade peak with a high maximum systolic velocity and reverse blood flow during early diastole.
Visualization of the celiac trunk
carried out by obtaining transverse sections from the epigastric region. The sensor moves from the xiphoid process caudally (2-3 cm) until the characteristic sign of “gull wings” appears, which is caused by the division of the celiac trunk into the common hepatic and splenic arteries. The celiac trunk is located in the form of a vessel 2-4 cm long, extending at an angle from the anterior surface of the aorta. During transverse scanning, the celiac trunk is visualized along its entire length, and the common hepatic and splenic arteries are visualized in the area of the ostia and in the proximal section. The celiac trunk and its visceral branches belong to the arteries with high peripheral resistance.
To obtain an image of the superior mesenteric artery
in the longitudinal section, the sensor is rotated 90°. The superior mesenteric artery extending from the anterior surface of the aorta is determined 1-2 cm below the celiac trunk. In transverse sections, it is located between the splenic vein and the aorta. The superior mesenteric artery is visualized above the aorta for 7 cm from its origin. To obtain the blood flow spectrum, the control volume is placed in the lumen of the vessel 1-1.5 cm from the point of origin from the aorta. Registration of the spectrum of blood flow in the superior mesenteric artery is performed at the mouth. The superior mesenteric artery is one of the arteries with high peripheral resistance.
Inferior mesenteric artery
originates directly below the renal artery from the left anterolateral surface of the abdominal aorta. Visualization of the inferior mesenteric artery is difficult due to its small diameter (3 mm or less). In some cases, its image can be obtained by scanning the abdominal aorta in a transverse or longitudinal plane, below the mouth of the left renal artery. The blood flow spectrum of the inferior mesenteric artery is characterized by high peripheral resistance.
To the criteria for narrowing or occlusion of arterial vessels
include qualitative and quantitative indicators of the spectral characteristics of the Doppler signal. Quantitative indicators reflecting the hemodynamics of the arterial bed are calculated:
- maximum, average and minimum blood flow speed,
- pulsatility index (PI),
- resistance index (RI),
- systolic-diastolic ratio (S/D).
The qualitative characteristics of the frequency spectrum of Doppler curves are assessed. An important sign of narrowing of the artery is the registration of turbulent flow with an expansion of the spectrum in systole and diastole. In the absence of a noticeable increase in the maximum amplitude of blood flow velocity during turbulent blood flow, a wide distribution of frequencies and a decrease in the area of the located “window”, characteristic of normal laminar blood flow in an arterial vessel, are recorded.
The most reliable and informative sign of narrowing of the main artery is an increase in the maximum systolic amplitude of the Dopplerogram (Fig. 1).
Maximum blood flow velocity or peak systolic blood flow velocity
(PSV) is measured in the visceral arteries at the level of the orifices and visualized segments of the celiac trunk and superior mesenteric artery. In addition to the peak systolic blood flow velocity, low-velocity blood flow indicators are assessed, reflecting changes (decrease) in cardiac output or indicating significant vasoconstriction.
An indispensable condition for accurate measurement
The peak systolic velocity of blood flow in the celiac trunk is the correction of the Doppler scanning angle of blood flow, which is 60°.
Blood flow parameters are measured during the deep inhalation and exhalation phases
. Normally, at the height of exhalation, there is an increase in the peak systolic velocity of blood flow in the celiac trunk by an average of 35.6 ± 5.9% compared to the deep inspiration phase. The average value of peak systolic blood flow velocity in the celiac trunk is 98-115 m/s, in the superior mesenteric artery - 98-142 m/s, in the inferior mesenteric artery - 93-189 cm/s. According to G.I. Kuntsevich et al., the maximum values of blood flow velocity in the celiac trunk correspond to 128 ± 12 cm/s, in the superior mesenteric artery - 136 ± 16 cm/s. The variability of blood flow speed parameters is one of the reasons for the discrepancy in results.
In the diagnosis of stenosis
unpaired visceral branches of the abdominal aorta, the most common include the criteria proposed by GL Moneta et al. The authors showed that the maximum blood flow velocity in the celiac trunk is 200 cm/s or more, in the superior mesenteric artery - 245 cm/s or more, which indicates hemodynamically significant stenoses (> 70%). The sensitivity, specificity, and predictive value of the celiac axis test were 75%, 89%, and 85%, respectively.
In addition to changes in peak systolic blood flow velocity, the value of end-diastolic blood flow velocity
with hemodynamically significant stenosis of the superior mesenteric artery. Since the diastolic component increases, acquiring the character of a main-altered type, with stenosis of more than 75%, the appearance of the Dopplerogram of the superior mesenteric artery changes. A comparative analysis of the results of Dopplerography and arteriography showed the informative value of end-diastolic blood flow velocity in the diagnosis of stenosis of the celiac trunk and superior mesenteric artery. As a result of the studies, it was established that for unpaired visceral branches of the abdominal aorta, arterial stenosis of more than 50% is hemodynamically significant.
There are various etiological factors
, causing anatomical changes and hemodynamic disturbances in the unpaired visceral branches of the abdominal aorta.
There are often two main groups of reasons leading to changes in the lumen of the vessel: intravasal and extravasal. Intravasal changes
are caused by congenital or acquired arterial diseases.
Congenital
abnormalities include vascular developmental anomalies - hypo-, aplasia, fibromuscular dysplasia, arteriovenous malformations
; acquired
- atherosclerosis, nonspecific aortoarteritis, thromboangiitis obliterans, post-embolic occlusion . The following forms of arterial damage are distinguished: occlusion, pathological tortuosity, aneurysm, and there are also combined and combined forms. The degree of narrowing of the vessel is considered as stenosis up to 50%, hemodynamically significant stenosis - > 50%, 75-90%, > 90%.
Extravasal compression
unpaired visceral branches of the abdominal aorta are primarily associated with the structural features and development of the aortic opening of the diaphragm, formed anteriorly and laterally by the tendinous edges of the right and left legs of the diaphragm, connected by the median arcuate ligament of the diaphragm, and posteriorly by the vertebral bodies. Compression of the vessels occurs by the median arcuate ligament of the diaphragm, its internal legs, and the effect on the celiac trunk is noted more often than on the superior and inferior mesenteric arteries. The reasons for frequent compression of the celiac trunk are the topographical features of the artery. Since the median arcuate ligament of the diaphragm is located at the level of the mouth of the celiac trunk or 2/3 of the vertebra below, during respiratory movements it moves and comes into contact with the celiac trunk. As a result of the interaction of the celiac trunk and the arcuate ligament on exhalation, compression of the mouth and the trunk itself occurs (Fig. 2).
Sometimes compression of the celiac trunk occurs when there is a high origin of the vessel from the aorta or a low attachment of the diaphragm with a normal level of origin of the artery. In addition, blood flow disturbances occur when the celiac artery is bent, which can occur as a result of its low origin from the aorta.
Another common cause of compression of the unpaired visceral branches of the abdominal aorta is extravascular compression
nerve ganglia of the solar plexus, neurofibrous tissue of the celiac plexus, tumors.
According to pathological studies, changes in the unpaired visceral branches of the abdominal aorta are observed in 19.2-70% of cases, according to angiography results - 4.4-53.5%. In groups of study patients that are heterogeneous in age and gender, the incidence of compression of the unpaired visceral branches of the abdominal aorta and the causes of its development vary significantly.
I. A. Komissarov et al. observed 538 children aged 5-18 years with abdominal pain. According to the results of a comprehensive study, including ultrasound duplex scanning, compression of the celiac trunk was detected in 109 children (20.2%), including 65 (59.7%) girls and 44 (40.3%) boys. Among the causes of compression of the celiac trunk
in children, extravasal effects of the arcuate ligament of the diaphragm, its internal legs, as well as compression of the celiac plexus by neurofibrous tissue were revealed.
L. A. Zvenigorodskaya et al. according to the results of a study of 236 patients (average age 53.5 ± 2.7 years) with chronic ischemic circulatory disease showed that in most cases (76.8%) there is intravascular damage to the unpaired visceral branches of the abdominal aorta, caused by the atherosclerotic process in the arteries . In other cases, extravasal compression of the celiac trunk was associated with the impact of the falciform ligament of the diaphragm.
A.V. Pokrovsky pointed out that according to the results of Doppler ultrasound, radiographic and pathoanatomical studies in patients with atherosclerosis of the coronary arteries, atherosclerotic lesions of the unpaired visceral branches of the abdominal aorta are detected in 73.5% of cases.
According to A.I. Kanaev et al., who studied 325 patients aged 17-72 years (average age 35.5 ± 0.8 years) with compression of the celiac trunk, disturbances in blood flow in the celiac trunk are caused by hemodynamic factors resulting from isolated stenosis of the celiac trunk or in combination with impaired blood flow in the superior mesenteric artery. Other pathogenetic factors of hemodynamic disturbances in the unpaired visceral branches of the abdominal aorta included mechanical irritation of the median arcuate ligament of the diaphragm and the pulse wave of the celiac plexus. In most patients with hemodynamic disorders in the celiac trunk, diseases of the stomach, duodenum, and pancreas were detected.
According to many researchers, in addition to compression of the unpaired visceral branches of the abdominal aorta, the state of collateral blood flow
. Collateral blood flow between the celiac trunk and the superior mesenteric artery is provided by the pancreaticoduodenal arcade. In the case of stenosis of the celiac trunk, which is the main arterial vessel supplying blood to the region, circulatory failure is compensated by redistributing blood in the zones: from the zone of the superior mesenteric artery to the zone of the celiac trunk. Failure of collateral blood flow during blood redistribution leads to ischemia in both zones (steal syndrome).
One study suggests a common causal relationship between hemodynamic disturbances in the celiac trunk and excessive development of the mitral valve leaflets and clinical signs of mitral valve prolapse. L. Arcari, having examined 1560 patients with ultrasound, revealed in 3.7% of cases (57 people - 23 men and 34 women) disturbances of blood flow in the celiac trunk. Mitral valve prolapse was diagnosed in 47 (82.4%) patients with impaired blood flow in the celiac trunk and 118 (7.9%; p < 0.001) without such signs. In the majority of patients with compression of the celiac trunk (average age 35 ± 12 years), no obvious reasons for extra- or intravasal compression of the artery were identified. The author, using multivariate statistical analysis, showed that hemodynamic disturbances in the celiac trunk are a sex- and age-independent factor associated with mitral valve prolapse.
Mitral valve prolapse
and other variants of minor cardiac anomalies are often identified in individuals with signs of hereditary connective tissue dysplasia, characterized by systemic changes. Among systemic disorders, developmental features, functional and organic diseases of the stomach, duodenum, and intestines are noted. Since with hereditary connective tissue dysplasia, in addition to cardiac architectonics, the structure and functional state of the vascular bed changes, disturbances in blood flow in the celiac trunk may be due to the peculiarities of the structure and metabolism of connective tissue.
T. Scholbach examined the celiac trunk with ultrasound in 3449 patients from 0 to 18 years old with complaints of abdominalgia. In 1.7% (59 patients aged 22 months - 19 years, including 81% females), signs of celiac trunk compression syndrome were detected. The results of sonography were confirmed in 21 patients using magnetic resonance imaging. In addition to abdominal pain, compression of the celiac trunk was accompanied by symptoms of chest pain (22%), nausea (29%), heartburn (17%), vomiting (15%), weight loss (15%), postprandial worsening symptoms (15% ), diarrhea (14%), respiratory discomfort (14%), syncope (12%), systolic murmur over the artery (15%).
Thus, the true prevalence of blood flow disorders
in the unpaired visceral branches of the abdominal aorta has not been determined; literature data indicate variability of results due to heterogeneity in age, gender, and clinical manifestations of the patients studied. Ultrasound diagnostics, including duplex color mapping, is an accessible method, comparable to angiographic studies, recommended for screening patients with circulatory disorders in visceral vessels. In a comprehensive study of patients with circulatory disorders in the unpaired visceral branches of the abdominal aorta, difficulties arise in identifying the only cause of extravasal compression of the celiac trunk, which often prevails in circulatory disorders in the unpaired visceral branches of the abdominal aorta, since hemodynamic disorders arise under the influence of many factors.
Trisvetova E. L., Varanitskaya N. M.
Belarusian State Medical University, 432nd Main Military Clinical Medical Center of the Armed Forces of the Republic of Belarus. Magazine "Medical Panorama" No. 9, October 2009.
Indications and contraindications for the treatment method
Indications:
Celiac stenosis more than 60% with chronic abdominal ischemia syndrome
Stenosis of the superior mesenteric artery more than 60% (symptoms of intestinal vascular insufficiency are not a mandatory indication, the fact of stenosis is sufficient)
Stage of endovascular treatment of acute mesenteric obstruction (mesenteric thrombosis)
Contraindications:
- Allergy to iodine
- Thoracoabdominal aortic aneurysm (without aneurysm surgery)
- Stage of intestinal necrosis with mesenteric thrombosis
Preparing for treatment
Standard examination before surgery:
- Clinical blood and urine tests, biochemical blood test.
- Coagulogram, platelet aggregation
- Gastroscopy (examination of the stomach)
- X-ray of the lungs
- ECG
- ECHO cardiography
- Ultrasound of the abdominal organs, aorta and arteries of the extremities
- Multislice computed tomography with contrast of the aorta and its branches
Before surgery, you must abstain from eating for 8 hours and liquids for 2 hours. No other preparation activities are required.
The celiac trunk (lat. truncus coeliacus) is the most important artery that feeds all the organs of the abdominal cavity, or rather its upper floor. It arises from the aorta at the level of the twelfth thoracic vertebra in the area of the aortic opening of the diaphragm. This is a fairly short, about 2 cm, but rather thick artery. After its origin, the trunk divides into three branches at the upper edge of the pancreas.
The first branch is the left gastric artery (lat. a. gastrica sinistra). This vessel goes to the stomach, its lesser curvature, feeding it, and also gives off branches to the abdominal part of the esophagus.
Next, the celiac trunk becomes the source of another one - the common hepatic artery (lat. a. hepatica communis). It goes to the duodenum, where, after giving off the gastroduodenal artery (lat. a. gastroduodenalis), it continues its course in the form of its own hepatic artery (lat. a. hepatica propria) and reaches the gate of the liver. This artery lies in the hepatoduodenal ligament, where its neighbors are the portal vein and, of course, the common bile duct. At the porta hepatis, the vessel divides into two branches, corresponding to the lobes of the liver: right and left. From the right branch originates the cystic artery (lat. a. cystica), which goes to the gallbladder. In addition, the right gastric artery (lat. a. gastrica dextra) begins from the common or proper artery of the liver, which goes to the stomach, or rather its lesser curvature, connecting there with the vessel of the same name on the left side. The previously mentioned gastroduodenal artery gives rise to two branches: the superior pancreatoduodenal (lat. a. pancreatoduodenalis superior) and the right gastroepiploic artery (lat. a. gastroepiploica dextra). The first of them goes to the stomach, its greater curvature, and gives branches to it and the omentum. The second most often represents a group of stems that branch in the pancreas and, in addition, in the duodenum.
And finally, the third branch is the splenic artery (lat. a. lienalis). It goes to the spleen, giving small branches along the way to the pancreas. Approaching the gate of the spleen, it divides into 5-8 small arteries, which branch in the organ. Before division, the left gastroepiploic artery (lat. a. gastroepiploica sinistra) is separated from it, which anastomoses on the greater curvature with the vessel of the same name on the right side. In addition, short gastric arteries (Latin aa. gastricae breves) go to the stomach from the splenic artery.
The celiac trunk, thanks to the numerous anastomoses of its branches, provides adequate and complete blood supply to the organs of the upper floor. Unfortunately, this important vessel is not immune to problems. One of them is stenosis. The celiac trunk, despite its thickness, under the influence of certain factors can narrow the lumen, which causes health problems. The narrowing can occur as a result of the deposition of atherosclerotic plaques on the inner wall of the trunk. This pathology is manifested by vague abdominal pain, bloating and other characteristic phenomena. Diagnosed using angiography. Not only this can cause stenosis of the celiac trunk. There is a disease called Dunbar syndrome. Due to a congenital anomaly of one of the diaphragm ligaments, compression of this important branch of the aorta occurs. Angiography shows stenosis at the site of compression and expansion immediately after it. The celiac trunk, having become a victim of this anomaly, gives the following clinical picture. Patients note aching abdominal pain, nausea, flatulence and vomiting, and sometimes diarrhea occurs. In addition, symptoms inherent in acute pancreatitis are possible: severe pain, vomiting, fever.
Stenosis of this artery is very dangerous because it supplies important organs: liver, spleen, stomach, etc. Lack of blood supply can cause serious and irreversible consequences, even death. Therefore, every person should pay full attention to unexplained abdominal pain.
How the treatment method works
The operation is performed under local anesthesia in the access area. Perhaps access will be on the thigh or in the elbow area. The surgical field is treated with an antiseptic and covered with sterile sheets.
The surgeon performs local anesthesia at the puncture site, after which the artery is punctured with a special needle and a short tube is installed - an introducer.
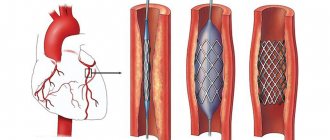
All further work with the vessels is carried out through the introducer. A special guide is inserted into the abdominal aorta, then a catheter is passed through it, through which a contrast study of the celiac trunk and mesenteric artery is performed. This stage is called selective angiography. It is the definitive diagnostic method. If narrowing of the arteries is confirmed, then the guidewire is inserted below the narrowing site. A balloon with a stent is passed through the guidewire. By expanding this balloon, the narrowing of the artery is eliminated, and the stent strengthens the arterial wall.
After stent implantation, control angiography is required to exclude possible complications. The catheter and introducer are removed from the access site, and bleeding is stopped by pressing or using a special Angiosil suturing device.
Possible complications during treatment
Complications of the operation itself:
- Rupture of a narrowed artery with bleeding requires emergency open surgery or installation of a special covered stent (stent graft). Fortunately, it is very rare.
- Thrombosis of the reconstructed artery is a rare complication that occurs with increased blood clotting. If preoperative preparation is carried out using antiplatelet preparation, then the risk is minimal. If thrombosis is observed during the intervention, then thrombectomy or thrombolysis (administration of drugs that resolve the clot) is performed. If signs of intestinal circulatory disorders are observed after surgery, the patient is taken back to the operating room and blood clots are removed using Rotarex or special aspiration catheters.
Complications of vascular access:
- Hematoma in the puncture area
- Arterial thrombosis in the puncture area
- Damage to nerves in the puncture area
These complications are extremely rare and can be easily eliminated if detected early.
Observation program after treatment method
The results of angioplasty and stenting of visceral arteries are monitored using ultrasound control after 3 months and then annually.
One year after the intervention, it is advisable to perform multislice computed tomography with contrast of the abdominal aorta and its branches.
After treatment, the patient is prescribed antithrombotic drugs. Most often these are aspirin and clopidogrel (Plavix). These medications must be taken regularly, and doctors must be notified before performing any other interventions.
Variant anatomy of the celiac trunk and hepatic artery
Key words: common hepatic artery, celiac trunk, pancreas, portal vein.
Introduction. Expanding the possibilities of surgical treatment of various diseases of the liver and biliary system requires a detailed study of the variant anatomy of the hepatic artery, portal vein, and biliary tract [1].
Vascular complications constitute the leading cause of postoperative morbidity and mortality in patients undergoing hepatic, pancreatic, or duodenal surgery. In this regard, obtaining information about the anatomy and topography of blood vessels before surgery is especially important when choosing the most adequate volume of surgical or endovascular intervention. This leads to a significant increase in the role of spiral computed tomography, which makes it possible to study the arterial blood supply of the pancreas and liver, as well as the variant anatomy of the elements of the hepatoduodenal ligament [2, 3].
Knowledge of the arterial blood supply to the liver is of paramount importance in patients who are planning to undergo liver transplantation or local tumor treatment methods.
Currently, the generally accepted classification is N. Michels, which includes 10 options for blood supply to the liver. In this classification, normal blood supply to the liver refers to the origin of the common hepatic artery from the celiac trunk. From the common hepatic artery originates the proper hepatic artery, which is divided into the right and left hepatic arteries. The normal (typical) anatomy of the celiac trunk is understood as its origin from the abdominal aorta and division into 3 branches: the left gastric, common hepatic and splenic arteries [4].
However, the literature describes many options for the arterial blood supply to the liver that do not fit into the framework of this classification, and the N. Michels classification does not fully meet the modern requirements of general, X-ray endovascular surgery and transplantology.
Target. Determination and assessment of the prevalence of variants of the anatomy of the celiac trunk and common hepatic artery according to contrast-enhanced spiral computed tomography.
Materials and methods of research. A retrospective, single-center, cohort study was conducted. The material for the study was a series of sections of the abdominal cavity, which were obtained during contrast-enhanced computed tomography in 250 patients who were treated at the 9th City Clinical Hospital in Minsk from 2014 to 2017.
The topographic and morphometric characteristics of the celiac trunk and common hepatic artery were studied. Using eFilmWorkstation V.4.2 software (MergeHealthcare), images taken in coronal, axial and sagittal projections were analyzed.
Statistical analysis was performed using Statistica 10 dialog software, Microsoft Excel.
Research results. Eight types of celiac trunk anatomy have been identified. Normal (typical) anatomy of the celiac trunk was observed in 222 of 250 patients (88.80%). Six anatomical variants of the celiac axis were identified in 24 (9.60%) patients. In the remaining 4 (1.60%) patients, the anatomy of the celiac trunk was classified as unclear, since the common hepatic artery was absent due to the separate origin of the proper hepatic artery and the gastroduodenal artery.
In 5 cases of normal origin of the common hepatic artery, the artery coursed behind the portal vein (n=4) or through the pancreatic tissue (n=1). In 1 case, the common hepatic artery departed from the left gastric artery and passed into the liver parenchyma through the gap of the venous ligament. In 8 cases, the common hepatic artery originated from the superior mesenteric artery. In this case, it was possible to trace the various topographic-anatomical relationships of the artery with the pancreas, superior mesenteric and portal vein. In 1 case, the common hepatic artery departed from the aorta and had a normal course: it passed above the pancreas, along the anterior surface of the portal vein.
Conclusions. The arterial blood supply to the liver is characterized by individual variability, which must be taken into account when performing surgical interventions on the liver, pancreas and duodenum.
The most common variant of branching of the celiac trunk is the normal (typical) variant with the formation of three branches: the common hepatic, splenic and left gastric arteries (88.80%).
Contrast-enhanced spiral computed tomography is an informative research method that allows a detailed assessment of the topography of the celiac trunk and common hepatic artery.
Literature:
- Adamthwaite JA, Pennington N, Menon KV (2007) Anomalous hepatic arterial anatomy discovered during pancreaticoduodenectomy. Surg Radiol Anat 9:269–271
- Gumus H, Bukte Y, Ozdemir E, Sentu¨rk S, Tekbas G, Onder H, Ekici F, Bilici A (2013) Variations of the celiac trunk and hepatic arteries: a study with 64-detector computed tomographic angiography. Eur Rev Med Pharmacol Sci 17:1636–1641
- Koops A, Wojciechowski B, Broering DC, Adam G, Krupski-Berdien G (2004) Anatomic variations of the hepatic arteries in 604 selective celiac and superior mesenteric angiographies. Surg Radiol Anat 26:239–244
- Michels NA Newer anatomy of the liver and its variant blood supply and collateral circulation. Am. J. Surg. 1966; 112(3):337–347