Cavernoma (cavernous malformations, cavernous angiomas) is a group of rare vascular formations in the central nervous system.
The formations are represented by dense or loose multi-chamber cavities (cavities) filled with blood, with varying degrees of its disintegration. The tissue around the cavernoma is usually significantly changed, but sometimes is not affected.
Localization of tumors can occur in almost any area of the central nervous system. 70% of formations are found supratentorial (above the tentorium of the cerebellum). Cavernomas are found under the tentorium of the cerebellum in 30% of cases. Of the lobes, the frontal and temporal lobes are mainly affected. Tumors in the spinal cord are rare - up to 2%. The rarest localizations: cerebellopontine angle, dura mater of the anterior and middle cranial fossae, cavernous sinus, pituitary gland region.
Sizes can vary: from a few millimeters to 9 cm.
Formations can be single or multiple. Single ones occur in 80-90% of cases.
Many studies indicate a number of causes for the occurrence of cavernous angiomas:
- Hereditary (presence of gene mutations);
- Sporadic, i.e. tumors that arise spontaneously under unknown circumstances or in isolated cases. They account for the majority of cases, approximately 80%.
- Induced by radiological radiation. A large number of reported cases in children under 10 years of age;
- Congenital (formed at 3-8 weeks of pregnancy). Very rare.
Clinical picture
Cavernomas are often asymptomatic.
Symptoms begin to appear with hemorrhages, as well as with growth into the surrounding tissues or their compression.
Focal neurological symptoms are associated with the amount of hemorrhage, epileptic seizures or increased intracranial pressure.
The most common headaches are of various types.
When the cavernoma is located supratentorially, epileptic seizures occur in more than 55%.
After the hematomas resolve, the symptoms decrease significantly.
How to recognize cavernous hemangioma
Parents can guess that a child has a vascular tumor by the appearance of the formation. It almost always has a round shape. The color of the formation depends on the depth of its location. If the hemangioma is localized in the upper layers of the skin, it has a red or purple color. With deeper subcutaneous formations, typical cyanosis of the skin occurs.
If you feel the vascular tumor, it may shrink. This metamorphosis is due to the fact that when pressed, blood flows out from the vessels of the formation. If the child has a cough, the formation, on the contrary, increases in size and becomes brighter.
Removal of a hemangioma is necessary, if only because such a tumor tends to grow. In some babies it reaches simply gigantic proportions. We recommend that you do not delay your visit to the doctor, because the smaller the formation, the easier it will be to remove it with minimal discomfort for the child.
Diagnostics
The most accurate method is magnetic resonance imaging (MRI).
The sensitivity of this method is 100% and the specificity is 98%.
At the preoperative stage, fMRI and diffusion tensor MRI (tractography) are used.
CT is used as an auxiliary method of neuroimaging.
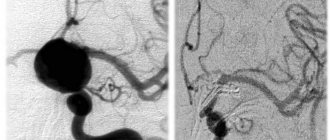
Angiography is sometimes required to study the angioarchitecture of cavernoma, as well as to carry out a differential diagnosis with other vascular diseases of the brain.
EEG to study the nature of seizures.
At the Medsi Neurosurgery Center, innovative equipment is available for a complete diagnosis of brain cavernomas.
Removal of cavernous hemangioma
Vascular tumor growth usually occurs before six to twelve months. In many cases, by the age of five, the formations are significantly reduced. Hemangiomas located in dangerous areas, for example, near the organs of vision or breathing, are subject to mandatory removal. Bleeding and injured formations are also subject to removal. It is recommended to remove the tumor if it has not gone away before the child reaches the age of seven.
One of the effective and progressive ways to remove a vascular tumor is radio wave surgery . We use the Surgitron device, with which even large formations are successfully removed. Under the influence of ionizing radiation, tumor cells die, while healthy surrounding tissues are not affected. Sometimes several procedures are required for the formation to completely disappear.
Another effective method is cryodestruction . In this procedure, the vascular tumor is specifically treated with liquid nitrogen. If the formation is small, it may disappear after the first session; in other cases, several procedures will be required. It is worth noting that when using the cryodestruction method there is a risk of scar formation, so it is rarely used when the tumor is localized in the facial area.
Unfortunately, it is impossible to prevent the appearance of a neoplasm in a child. If your baby is diagnosed with a vascular tumor, do not panic. Better come to our medical center for examination and safe removal.
Types of acquired red moles on the body
- Simple (capillary). Proliferation of newly formed capillaries, small venous and arterial vessels. Looks like a red spot.
- Cavernous. A spongy cavity with blood - a red or bluish nodule. Often forms under the skin.
- Branched (racellose). A plexus of tortuous dilated capillary trunks. They pulsate, noise and trembling are detected. It is rare and occurs on the extremities or face. If injured, life-threatening bleeding may occur.
How to identify hemangioma? Press on top of it and it should fade or disappear.
Why does hemangioma need to be treated?
The sooner a hemangioma is treated, the less consequences and residual effects can develop. This is due to the fact that the tumor can noticeably increase in a short period of time and grow into neighboring organs and tissues.
Treatment is indicated primarily for patients whose hemangioma is located in the following areas:
- In the respiratory system or near the respiratory tract;
- Around eyes;
- On the face with a risk of cosmetic defects;
- In the ear area;
- If there are ulcers (ulcers). Ulcerations can be painful and lead to scarring, sometimes very rough and disfiguring, and the presence of ulcers can lead to infection and bleeding!
Features of treatment
The method of getting rid of a tumor largely depends on its size and shape.
Small tumors (up to 5-6 cm in volume) do not require special action. They are monitored and ultrasonic controlled after 3 months from the moment of detection. In the absence of any dynamics, ultrasound diagnostics are prescribed every 6-12 months.
The need for surgical removal is determined individually. This course of events leads to:
- rapid growth of liver hemangioma - more than 50% of the original size per year;
- volume more than 5-6 cm;
- bleeding of atypical tissue;
- aggressive manifestation of symptoms;
- inaccurate determination of the benignity of the tumor.
Classification
In world medical practice, there are several varieties of this tumor:
- cavernous hemangioma of the liver, which is several free cavities connected into a single one;
- capillary hemangioma of the liver forms a large number of small cavities, each of which houses a blood or venous vessel.
Along with the most common ones, venous, cluster-shaped hemangioma, and hemangioendothelioma can also occur.
Differential diagnosis
Kvernous venous malformations should be differentiated from numerous other pathologies leading to multiple microhemorrhages, including:
- cerebral amyloid angiopathy
- chronic hypertensive encephalopathy
- diffuse axonal injury
- cerebral vasculitis
- radiation damage to the brain
- hemorrhagic metastases
- Parry-Romberg syndrome
Large malformations can simulate:
- hemorrhage into metastases
- hemorrhage into a primary tumor (eg glioblastoma)
Surgical interventions: technique and results
Planning of access and surgical intervention for removal of cerebral cavernomas generally correspond to the general principles used in surgery of space-occupying brain lesions. In the case of superficial subcortical localization, the search for malformation is greatly facilitated by the presence of post-hemorrhagic changes in the superficial cortex and meninges. The cavernoma, as a rule, is clearly demarcated from the medulla, which simplifies its isolation. If the cavernoma is localized outside functionally important areas, identifying the malformation in the area of perifocal changes and removing it in one block significantly facilitates and speeds up the operation. To improve the outcome of treatment of epilepsy, in some cases, a technique is also used to excise the macroscopically altered brain matter around the cavernoma by blood breakdown products, although information about the effectiveness of this technique is contradictory. Surgeries to remove cavernomas located in functionally significant cortical and subcortical parts of the brain, as well as in deep structures cerebral hemispheres, have a number of features. In case of hemorrhage from a cavernoma of this localization, the patient should be monitored for 2–3 weeks. The absence of regression of focal symptoms during this period provides additional justification for surgical intervention. When making a decision about surgery, you should not wait for the hematoma to resolve, since due to the processes of organization and gliosis, the operation becomes more traumatic. Internal decompression of a cavernoma by evacuation of the hematoma is a necessary step when removing cavernomas from functionally significant areas, as it allows to reduce surgical trauma. Resection of perifocal posthemorrhagic changes is impractical.
| Removal of a small cavernoma using neuronavigation |
To improve the outcomes of cavity removal, various instrumental intraoperative auxiliary techniques are used. In the absence of clear anatomical landmarks, it is advisable to use intraoperative navigation methods. Ultrasound scanning in most cases allows you to visualize the cavity and plan the access trajectory. A significant advantage of the method is the provision of information in real time. Ultrasound imaging of cavernomas can be difficult for small lesions. Frameless neuronavigation based on preoperative MRI data allows for the most accurate planning of access and craniotomy of the required (minimum possible for a given situation) size. It is advisable to use the technique to search for small caverns. Stimulation of the motor area with assessment of the motor response and M-responses should be used in all cases of possible intraoperative damage to the motor cortex or pyramidal tracts. The technique allows you to plan the most gentle access to the cavernoma and evaluate the possibility of excision of the zone of perifocal changes in the medulla. Intraoperative use of ECoG to assess the need for excision of distant foci of epileptiform activity is advisable in patients with a long history of epilepsy and drug-resistant seizures. In the case of epileptic lesions of the medial temporal structures, the technique of amygdalohippocampectomy under ECoG control has shown high effectiveness. For any location of the cavernoma, one should strive for complete removal of the malformation due to the high frequency of repeated hemorrhages from partially removed cavernomas. It is necessary to preserve venous angiomas found in the immediate vicinity of cavernomas, since their excision is associated with the development of disturbances in the venous outflow from the medulla adjacent to the cavernoma. In most cases, cavernomas, even very large ones, can be completely removed, and the outcomes of operations are usually favorable: most patients do not experience neurological disorders. In patients with epileptic seizures, improvement is noted in 75% of cases, and in 62% of cases, seizures do not recur after removal of the cavernoma. The risk of developing postoperative neurological complications depends largely on the location of the formation. The incidence of defects in cavernomas located in functionally insignificant parts of the cerebral hemispheres is 3%. With cortical and subcortical cavernomas of functionally significant areas, this figure increases to 11%. The risk of the appearance or worsening of a neurological deficit in the case of removal of a deep-seated cavity reaches 50%. It should be noted that the neurological defect that occurs after surgery is often reversible. Postoperative mortality is 0.5%.
Dimensions and location
| Cavernoma of the spinal cord at the Th2 level |
The sizes of caverns can be very different - from microscopic to gigantic. The most typical cavernomas are 2–3 cm in size. Cavernomas can be located in any part of the central nervous system. Up to 80% of cavernomas are found supratentorially. Typical localization of supratentorial cavernomas is the frontal, temporal and parietal lobes of the brain (65%). Rare cases include cavernomas of the basal ganglia and thalamus opticum - 15% of cases. Even less common are cavernomas of the lateral and third ventricles, the hypothalamic region, the corpus callosum, and the intracranial sections of the cranial nerves. In the posterior cranial fossa, cavernomas are most often located in the brain stem, mainly in the tegmentum of the pons. Isolated midbrain cavernomas are quite rare, and medulla oblongata cavernomas are the least common. Cerebellar cavernomas (8% of all cavernomas) are most often located in the cerebellar hemispheres, less often in the vermis. Cavernomas of the medial parts of the cerebellar hemispheres, as well as the vermis, can spread to the fourth ventricle and to the brain stem. Spinal cord cavernomas in our series accounted for 2.5% of all cavernomas. Taking into account the location of cavernomas in terms of difficulty of access and the risk of surgical intervention, it is customary to divide supratentorial cavernomas into superficial and deep. Among superficial cavernomas, there are those located in functionally important zones (speech, sensorimotor, visual cortex, insula) and outside these zones. All deep cavernomas should be considered as located in functionally significant zones. According to our data, cavernomas of functionally significant areas of the cerebral hemispheres make up 20% of supratentorial cavernomas. For cavernomas of the posterior cranial fossa, all localizations, with the exception of cavernomas of the lateral parts of the cerebellar hemispheres, should be considered functionally significant. CNS cavernomas can be single or multiple. The latter are detected in 10–20% of patients. According to our data, patients with multiple cavernomas made up 12.5% of those examined. Single cavernomas are typical for the sporadic form of the disease, and multiple ones are typical for the hereditary form. The number of cases of multiple cavernomas in the hereditary form reaches 85%. The number of cavernomas in one person varies from two to 10 or more. In some cases, the number of cavernomas is so large that it is difficult to count.
Answers to common questions
What is the prevention for hemangiomas?
Since the exact cause of hemangioma has not been determined, a competent preventive measure is to conduct an ultrasound diagnosis of the liver once a year. If there is any doubt, an additional CT or MRI should be done.
Is it necessary to follow a diet for liver hemangioma?
Proper selection of nutrition is mandatory if the patient is determined for a positive result. Eating foods that are unacceptable in the diet of a sick person can provoke a sharp growth and rupture of the hemangioma.
Why is liver hemangioma dangerous?
Its main danger is possible tissue rupture and subsequent bleeding. There is also a possibility that due to the large size of the tumor, neighboring organs will be compressed, and therefore their functioning will be disrupted.
How to treat liver hemangioma?
Treatment for this disease is selected depending on its size and growth rate. The specialist can select hormonal therapy, minimally invasive methods (for example, radiation therapy), as well as surgery. To consolidate the effect of treatment, you must follow a special diet.