The disease belongs to the group of chronic obliterating diseases of the arteries of the legs. This is a whole group of diseases, the common symptom of which is a decrease in blood flow to the limb due to stenosis (narrowing) or occlusion (complete blockage) of the artery. The stage of arterial insufficiency and the degree of tissue ischemia (bleeding) depend on the degree of stenosis. The more pronounced the stenosis, not to mention the occlusion, the less blood volume enters the limb.
Changes in the vascular wall of the arteries, which lead to stenosis or occlusion of the vessel, occur in many diseases, but most often the cause is only four diseases:
Obliterating atherosclerosis - develops mainly in men over 40 years of age against the background of increased cholesterol levels (low and very low density lipoproteins). Mainly large and medium caliber arteries are affected, such as: aortic bifurcation; common iliac; femoral and popliteal arteries.
Obliterating endarteritis (thromboangiitis obliterans, Buerger's disease) is an inflammatory disease of the vascular wall of autoimmune origin, usually occurring at a young age. The disease is characterized by the presence of autoantibodies and circulating immune complexes in the blood. In the initial stages of the disease, mainly small and medium caliber arteries are affected, in particular, the arteries of the leg and foot. At later stages, larger arteries are involved in the pathological process - popliteal, femoral and iliac.
Nonspecific aortoarteritis (Takayasu's disease) is an inflammatory disease of autoimmune origin affecting the aorta and its large branches.
Diabetic angiopathy. Occurs in patients suffering from diabetes. Diabetic angiopathy is characterized by damage to both small and large vessels. Changes in the vascular wall occur especially often in arteries of medium and small caliber (popliteal, tibial, arteries of the foot).
In addition to the above diseases, post-embolic occlusion, traumatic thrombosis, as well as congenital diseases (hypoplasia, aplasia and fibromuscular dysplasia) are much less common.
It is generally accepted among specialists to divide the vascular bed of the lower extremities, including according to the level of disease damage, into 3 levels (segments):
- aorto-iliac;
- femoral-popliteal;
- popliteal tibial (peripheral)
The incidence of obliterating atherosclerosis and other occlusive diseases of the arteries of the lower extremities is not reliably known, since about half of patients with diseases of the peripheral arteries of the lower extremities do not have any symptoms or signs of the disease. However, the incidence of peripheral artery disease of the lower extremities is known to increase with age and at least 25% of the US population suffers from these diseases.
Causes
Vascular occlusions are associated with a state of vascular insufficiency. The occlusion process occurs:
- as a result of injuries, if the artery is compressed.
- due to the fact that the lumen is blocked by a thrombus or embolus.
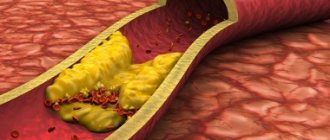
The formation of blood clots is promoted by a chronic disease - vascular atherosclerosis. As atheromatous plaques grow and increase in diameter, they interfere with normal blood flow. Atherosclerotic plaque leads to blood clotting and blood clot formation. Occlusion is caused by separated plaque fragments that move freely along the vascular bed. In addition, as a result of atherosclerosis, the walls of blood vessels lose their elasticity, become thinner and stratify under blood pressure, which causes the formation of aneurysms. Thrombosis or embolism is likely to occur in the area of the vessel where the dilatation has appeared.
Treatment methods for obliterating atherosclerosis of the arteries of the lower extremities:
Conservative therapy
In the early stages of obliterating atherosclerosis of the arteries of the lower extremities, conservative treatment is indicated, which must be comprehensive, and all unfavorable factors causing vasospasm must be excluded. A necessary condition for successful treatment is quitting smoking(!). Physical activity is of paramount importance. Patients with intermittent claudication should walk daily for 30-45 minutes - this promotes the development of small arteries, leads to an increase in muscle strength and an increase in the distance traveled without pain.
If pain and compression appear in the leg muscles, the patient should stop, and after these sensations disappear, continue walking. Often, cycling or swimming are much better tolerated than walking (however, they do not replace it). Correction of increased blood pressure, normalization of blood cholesterol levels, blood glucose levels in patients with diabetes mellitus. Drugs are used that reduce the tone of small vessels, increase the flexibility of red blood cells and prevent the formation of blood clots in the vessels. Physiotherapeutic and balneological procedures, hyperbaric oxygenation are also used.
Surgical treatment of arteriosclerosis of the arteries of the lower arteries, vessels
Reconstructive operations:
- X-ray endovascular treatment methods.
Under the control of X-rays using special long thin instruments, through a small puncture in the femoral artery (less often other arteries), we can reach the affected vessel (area of blood vessels) of the lower extremities. Modern technical capabilities make it possible to expand a section of the vessel from the inside with a special balloon and, if necessary, install a thin metal frame (stent) that prevents re-narrowing.
- Open surgical interventions.
For patients with blockage of a vessel lasting no more than 7-9 cm, the internal modified layer of the artery with atherosclerotic plaque and blood clots is removed (endarterectomy). With a more significant spread of the occlusive process, pronounced calcium deposition in the artery wall, a bypass of the blood flow (bypass) or resection of a section of the artery and its replacement with a synthetic prosthesis or biomaterial (prosthetics) is indicated.
Amputation
If, despite the treatment, ischemia of the affected limb increases and gangrene progresses, amputation is indicated: its level must be strictly individual and carried out taking into account the blood supply to the limb.
Occlusion of cardiac vessels
A dangerous condition is considered to be acute occlusion of the coronary arteries, which supply blood to the heart muscle. This occurs as a result of atherosclerosis of the coronary arteries and coronary heart disease. If, during the chronic course of the disease, a person experiences angina pectoris, then the acute form is fraught with a heart attack and even death of the patient. Typical signs of cardiac vascular occlusion are chest pain that lasts more than 10 minutes and does not go away with rest or after taking nitroglycerin. In this case, the concept of acute coronary syndrome is used: a patient with such symptoms should be immediately hospitalized.
The danger lies in the fact that a person initially ignores the symptoms of coronary artery disease or simply does not feel them without taking any measures. Vascular occlusion is characterized by suddenness and unexpectedness, so at the first signs of developing coronary artery disease, consult a doctor immediately.
Obliterating diseases of the aorta and arteries of the lower extremities
X
Chronic obliterating diseases of the aorta and arteries of the lower extremities (caused in most cases by atherosclerosis) account for more than 20% of all types of cardiovascular pathology, which corresponds to 2–3% of the total population [1]. Thus, in the Edinburgh study (1990) [2], patients with intermittent claudication accounted for 4.5% in the age group from 55 to 74 years, and asymptomatic lesions were noted in 8% of cases. It is significant that the attending physicians only 30–50% of patients knew about the presence of intermittent claudication in the latter [3].
The main feature of this pathology is its steadily progressive course.
, characterized by an increase in the severity of intermittent claudication and its transition to a constant pain syndrome or gangrene, which occurs in 15–20% of patients [4]. Perioperative mortality for amputations below the knee is 5–10%, above the knee – 15–20%. Mortality during the first two years after amputation ranges from 25–30%, and after 5 years – 50–75%. Moreover, after amputation of the lower leg, only 69.4% of patients walk on a prosthesis after 2 years, and only 30.3% of the hips.
Mortality after reconstructive surgery, which previously amounted to 2–13% [5], currently does not exceed 1.2% in leading Russian clinics [6]. When estimating the required number of operations for patients with obliterating diseases of the aorta and arteries of the lower extremities, we can cite the United States as an example, where in 1995 there were 400,000 hospitalizations for diseases of the peripheral arteries. 50,000 balloon angioplasties, 110,000 bypass operations, and 69,000 amputations were performed. Moreover, the costs of primary amputation in developed countries, such as the UK, were twice as high as the costs of successful revascularization [7].
According to L.A. Bokeria et al. [8], as of 1998, the need for reconstructive operations on the arterial system in Russia is 930 per 1 million population, no more than 22% of the required number is performed annually.
Pathomorphology and pathogenesis
The term “atherosclerosis” comes from the Greek words “athtre” - wheat gruel and “sclerosis” - hard. Despite the fact that the pathomorphology of atherosclerosis has been studied for more than 140 years, starting with the first works of R. Virchow (1856), the nature and features of the processes occurring in the vascular wall during this disease remain not completely clear. Even cellular and extracellular changes observed during microscopic examination in the vessel wall in the area of atherosclerotic plaque formation are interpreted differently. During the formation of atherosclerosis, the main changes occur in the endothelium and smooth muscle cells of the subendothelial layer of the intima.
There are 4 types of atherosclerotic changes in blood vessels:
1. Fatty spots or stripes, which are pale yellow areas containing lipids that do not rise above the surface of the intima. These are the earliest manifestations of atherosclerosis.
2. Fibrous plaques
- oval or round formations containing lipids, rising above the surface of the intima, often merging into continuous tuberous fields.
3. Fibrous plaques with various kinds of complications:
ulceration, hemorrhage, imposition of thrombotic masses.
4. Calcinosis
– deposition of calcium salts in fibrous plaques.
The most significant atherosclerotic changes are most often localized in places of greatest hemodynamic or mechanical impact on the vessel wall: bifurcation zones, places where the main arteries depart from the aorta and in tortuous sections of the artery.
According to JSA Fuchs [9], the leading risk factors for the development of atherosclerosis include arterial hypertension, hypercholesterolemia and smoking. To a lesser extent, obesity, diabetes mellitus, hypertriglyceridemia, sedentary lifestyle, stress and heredity influence.
Modern diagnostic methods
Modern methods for diagnosing peripheral arterial circulatory disorders are distinguished by their wide range - some are used to clarify the clinical diagnosis, the nature and extent of vascular damage, others are used to assess the effectiveness of treatment or dynamic monitoring of the patient. In order to study hemodynamics in the lower extremities and topical diagnosis of lesions of the arterial bed, the following instrumental research methods are used:
Doppler ultrasound sphygmomanometry, treadmill test, ultrasound angioscanning, including duplex, and radiopaque aortoarteriography. In addition, it is necessary to determine indicators of lipid metabolism, coagulation system and rheological properties of blood.
As the first stage, all patients with suspected occlusive-stenotic lesions of the aorta or arteries of the lower extremities undergo Doppler ultrasound with measurement of the ankle-brachial index
.
This index is the ratio of the maximum pressure on one of the tibial arteries to the pressure on the brachial artery. A decrease in this indicator to less than 0.9 requires closer attention to the patient. of Doppler ultrasound and standard treadmill test seems to be one of the most promising at present.
[10].
Non-invasive research methods also include ultrasound angioscanning
, thanks to which the degree of stenotic lesion can be determined with a high degree of certainty.
Recently, duplex ultrasound angioscanning
has taken one of the leading places in the diagnostic program algorithm due to its non-invasiveness and safety, as well as high sensitivity and specificity.
According to duplex scanning data, not only the structure of the atherosclerotic plaque is determined, but also the hemodynamic degree of stenosis is assessed, which is of fundamental importance. X-ray contrast angiographic examination
currently remains the main method for diagnosing obliterating diseases of the vascular bed. Using this method, it is possible to accurately determine the location, extent, degree and nature of stenosis, the multiplicity of occlusive lesions of the main arteries of the lower extremities, assess the condition of the collateral bed, predict the nature and volume of reconstructive surgery, and also monitor the effectiveness of treatment and surgery. In the arsenal of angiologists and vascular surgeons there are also such diagnostic methods as laser Doppler flowmetry, transcutaneous O2 monitoring, photoplethysmography, radioisotope study, computed tomography and nuclear magnetic resonance.
Terminology and clinical classification
“Leriche syndrome” is often used to refer to diseases of the abdominal aorta that lead to its narrowing or occlusion.
, which summarizes the picture of damage to the bifurcation of the abdominal aorta and iliac arteries.
The main features of the clinical course of this lesion are high intermittent claudication (pain in the limb when walking), bilateral absence of pulses in the arteries and impotence.
In approximately 30% of patients with chronic arterial insufficiency of the lower extremities, the atherosclerotic occlusive process is localized in the abdominal aorta, in 70% of patients - in the arteries of the femoral-popliteal segment.
Tactical issues in choosing one or another treatment method for atherosclerotic lesions of the aorta and arteries of the limb are based on the severity of chronic ischemic syndrome, which is classified into 4 stages of the disease. The predominant assessment system is the classification of R. Fontaine and A.V. Pokrovsky.
At stage 1 of the disease
pain in the lower extremities appears only with heavy physical activity; it is not related to the distance the patient walks.
For stage 2
Characteristic is the appearance of limiting pain when walking (limiting intermittent claudication). From a tactical point of view, this stage is divided into 2A (a distance walked without pain of more than 200 m) and 2B (the appearance of pain when walking at a distance of less than 200 m).
Pain in the limb at rest characterizes the 3rd stage
, the appearance of ulcerative-necrotic changes -
stage 4 of the disease.
Surgical tactics and determination of the degree of surgical risk
The fundamental generally accepted position in choosing a treatment method in accordance with this classification is the need to restore the main blood flow using reconstructive operations, starting from stage 2B.
When deciding on surgical treatment, it is necessary to take into account the multifocal nature of the atherosclerotic lesion and the presence of concomitant pathology that aggravates the condition of the patients. According to our data, about 70% of patients suffer from coronary heart disease, every 4th is diagnosed with post-infarction cardiosclerosis and chronic cerebral circulatory failure, half of the patients have hypertension in combination with chronic lung diseases. 35% have gastrointestinal tract diseases and every 7th person has diabetes mellitus.
Based on all of the above, treatment of patients with atherosclerosis should be comprehensive
, aimed both at restoring blood circulation in the aorta and main arteries of the limb, and at correcting concomitant pathology. The main goal - restoration of blood circulation - should be achieved with minimal trauma to the patient.
Principles of conservative treatment
One of the main directions of conservative treatment is to improve the rheological properties of blood.
And this is not accidental, since patients have pronounced deviations in rheological characteristics: an increase in the level of fibrinogen in plasma, an increase in platelet aggregation time, blood and plasma viscosity, a decrease in the fibrinolytic activity of the blood and a change in thromboelastogram parameters towards hypercoagulation.
Among the drugs used for conservative therapy, several groups are distinguished.
1. Antispasmodics:
peripheral myolytics (papaverine, drotaverine, bencyclane), drugs blocking a-adrenergic receptors or preganglionic impulse transmission (caffeine, prazosin), central cholinomyolytics (tolperisone, baclofen), substances with versatile effects (abana).
2. Disaggregants:
pentoxifylline, acetylsalicylic acid, xanthinol nicotinate, ticlopidine, rheopolyglucin.
3. Antiatherosclerotic agents:
drugs that block the absorption of cholesterol from the intestine (cholestyramine), inhibiting the biosynthesis and transfer of cholesterol and triglycerides (fibric acid derivatives - clofibrate, ciprofibrate) and statins (lovastatin, simvastatin), other drugs (nicotinic acid).
4. Metabolic drugs:
solcoseryl, actovegin, etc.
5. Angioprotectors:
pyricarbate, etc.
I would especially like to emphasize that dosed walking
– health path, which promotes the development of collateral circulation.
Purely conservative treatment is indicated for patients with chronic arterial insufficiency of stage 1 and 2A; in patients with stage 2B and critical ischemia with the development of ulcerative-necrotic lesions, the question arises about the need to restore the main circulation. Thanks to the capabilities of modern technologies, in recent years a lot of work has appeared on the use of balloon angioplasty.
in patients with different localization of occlusive-stenotic lesions of the arteries of the pelvis and lower extremities.
However, it is not possible to use balloon repair in all cases due to aortic occlusion or common arterial occlusions. Attempts at recanalization in these cases are dangerous by the development of thrombosis of the main arteries (often with thrombosis of the peripheral bloodstream), which inevitably leads to amputation of the limb in 60% of cases, and often to death.
Types of reconstructive surgical interventions
In case of high occlusion of the aorta, bilateral damage to the arteries of the extremities, depending on the severity of the patient’s condition, operations are performed from aortofemoral bifurcation or linear bypass to axillary or subclavian-femoral bifurcation bypass. If critical ischemia is present only on one side, then if the iliac and femoral arteries are affected on the contralateral limb, a unilateral cross-iliac-femoral, axillary or subclavian-femoral bypass
.
At the present stage, reconstructive operations occupy a leading place in the treatment of these patients. The number of such operations is constantly increasing, their scope is expanding significantly, which makes it possible to save a limb even in severe forms of chronic arterial insufficiency. Contractubex is effective for resolving keloid scars that occur after surgery.
, which has fibrinolytic, antithrombotic and keratolytic effects.
Meanwhile, performing a full-fledged reconstruction often conflicts with the patient’s ability to undergo surgery. Operations in these cases should be minimal in terms of trauma and duration, since the vast majority of this group of patients have severe concomitant diseases that sharply limit the functional reserve capabilities of the body [11]. Using the combined operations method
, including balloon angioplasty in combination with open surgery under epidural or local anesthesia, can significantly reduce the volume of intervention and eliminate complex surgical reconstruction in several segments.
Clinical case
Patient Z., 68 years old, was admitted with complaints
for aching pain in the right leg and foot at rest, intermittent claudication after 30 m.
Doppler ultrasound:
a significant decrease in the main blood flow in the right common femoral artery, collateral blood flow in the popliteal and tibial arteries.
Ankle-brachial index
left 0.59, right 0.35.
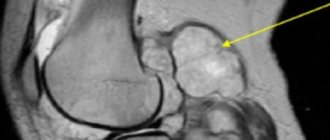
Aortoarteriography:
critical stenosis of the common iliac artery (CIA) on the right; stenosis of the deep femoral artery (DFA) on the right; occlusion of both superficial femoral arteries (SFA), segmental occlusion of the right popliteal artery for 5 cm (Fig. 1).
Rice.
1. Angiograms of patient Z.: a — stenosis of the abdominal cavity on the right; b — stenosis of the GBA on the right, occlusion of both SBAs; c — after balloon angioplasty (absence of an area of stenosis of the right PA). Atherosclerotic lesion of arteries (case history).
Concomitant diseases: coronary heart disease, atherosclerotic cardiosclerosis, angina pectoris, chronic bronchitis, pneumosclerosis, pulmonary emphysema.
coronary heart disease, atherosclerotic cardiosclerosis, angina pectoris, chronic bronchitis, pneumosclerosis, pulmonary emphysema.
The first stage was balloon angioplasty of the right abdominal organ, and the second stage, under epidural anesthesia, was lateral plasty of the gastrointestinal tract on the right (Fig. 2).
Rice.
Fig. 2. Scheme of stages of surgical treatment of patient Z.: a - before surgery; b — balloon angioplasty of the right PCA; c — condition after plasty of the GBA and balloon angioplasty of the abdominal organ on the right. As a result,
positive dynamics were noted: the ankle-brachial index on the right increased to 0.71 (initially 0.35). The patient was discharged in satisfactory condition for outpatient treatment.
You can find a list of references on the website https://www.rmj.ru
References:
1. Pokrovsky A.V., Koshkin V.M., Kirichenko A.A. et al. Vasaprostan (prostaglandin E1) in the treatment of severe stages of arterial insufficiency of the lower extremities. A manual for doctors. M., 1999; 16.
2. Fowkes FG, Housley E, Cawood EH et al. Edinburgh artery study: prevalence of asymptomatic and symptomatic peripheral arterial disease in the general population. Int J Epidimiol 1991; 20: 384–92.
3. Burakovsky A.I., Bockeria L.A. Cardiovascular surgery. M., 1989; 750.
4. Dormandy J., Mahir M., Ascady G. et al. Fate of the patient with chronic leg ischemia. J Cardiovasc Surg 1989; 30:50–7.
5. Stoffers HEJH. Kaiser V. and Knottnerus JA Prevalence in the general practice. In: Fowkes FGR, ed. Epidemiology of peripheral vascular disease. London: Springer Verlag. 1992; 109–13.
6. Spiridonov A.A., Fitileva E.B., Arakelyan V.S. Ways to reduce mortality in surgical treatment of chronic ischemia of the lower extremities. J. Annals of Surgery. 1996; 1:62–6.
7. Bead J.D. Amputation or reconstruction for critical ischemia. J. Angitology and Vascular Surgery 1998; 1 (4): 72–82.
8. Bockeria L.A., Gudkova R.G. Surgery of the heart and blood vessels in the Russian Federation. M., 1998; 43.
9. Fuchs JSA. Atherogenesis and the medical management of Atherosclerosis. In: Rutherford RB, ed. Vascular surgery. Philadelphia: W. B. Saunders Company. 1996; 1:222–35.
10. Zatevakhin I.I., Tsitsiashvili M.Sh., Yudin R.Yu. Treadmill in the diagnosis and treatment of chronic arterial insufficiency. M., 1999; 87.
11. Siskin G., Darling RC III, Stainken B. et al. Combined use of Iliac artery angioplasty and infrainguinal revascularization for treatment of multilevel atherosclerotic disease. Annals of Vascular Surgery. St. Louis. 1999; 13 (1): 45.
Peripheral vascular occlusion
Large arteries of the extremities, more often the lower ones, are susceptible to vascular occlusion. Occlusions are an unpleasant consequence of vascular diseases of the legs. At the same time, the threat of an acute occlusive process in this area is dangerous due to the development of tissue necrosis, which leads to amputation of the affected limb. Characteristic signs of thromboangiitis obliterans, atherosclerosis of leg vessels and other common pathologies are:
- pain in the legs that does not go away with rest;
- pallor of the skin of the extremities;
- coldness in the legs;
- tingling sensation, numbness in the limb;
- impairment of motor functions of the limb.
If these symptoms appear, it is recommended to immediately examine and treat the vessels of the extremities: the slightest delay can result in the development of gangrene. In the early stages of the development of the disease, treatment of obliterating atherosclerosis of the lower extremities and other pathologies of sclerotic origin is carried out using conservative methods, whereas in an advanced form it is difficult to fight the disease.
Occlusive processes occur in the arteries of the kidneys, resulting in the development of renovascular hypertension and kidney dysfunction. The aorta is also affected, since it is the largest vessel. Read about the consequences of aortic atherosclerosis by clicking on the link.
Symptoms of obliterating atherosclerosis of the arteries of the lower extremities
Pay attention to the following symptoms in yourself or your loved ones:
- fatigue in the calf muscles or thigh muscles when walking 500 meters or less,
- a feeling of leaden heaviness in the legs or muscle pain that makes you stop when walking,
- changes in the skin on the legs in the form of peeling, thinning, hair loss.
Important!
These are signs of atherosclerotic damage to the arteries of the lower extremities. An examination by a vascular surgeon is required in the near future. Do not be surprised if, when diagnosing lesions of the arteries of the lower extremities, your carotid arteries are checked and a cardiological examination is prescribed. Atherosclerosis is a systemic disease, and, as a rule, different groups of blood vessels are affected.
If sharp pain in the foot or lower leg occurs simultaneously with paleness and coldness of the skin, you must immediately call an ambulance, otherwise you may not have time to save the limb.
Occlusion of blood vessels supplying blood to the brain
Occlusive processes in the arteries supplying the brain are fraught with dangerous consequences. Impairment of cerebral blood supply is fraught with the development of a stroke or ischemic cerebral infarction, and this often ends in the patient’s death, paralysis or dementia. A common cause of this is carotid artery occlusion. It is accompanied by loss of consciousness, nausea and vomiting, impaired coordination, speech and vision, weakness and numbness of the limbs. A harbinger of strokes are transient (cerebral) ischemic attacks, which we described in detail earlier.
The main methods for diagnosing obliterating atherosclerosis of the arteries of the lower extremities:
- measurement of the ankle-brachial index (the ankle-brachial index is a parameter that allows you to assess the adequacy of arterial blood flow in the lower extremities);
- duplex scanning of the arteries of the lower extremities is the “gold standard” for screening patients (detection and follow-up);
- MSCT angiography of the aorta and arteries of the lower extremities is the “gold standard” of preoperative examination and in cases where information from ultrasound scanning is insufficient;
- X-ray contrast angiography.
Causes of femoral artery occlusion
The cause of occlusion of the femoral artery in the majority (75-80%) of cases is obliterating atherosclerosis. Atherosclerosis is a disease in which cholesterol plaques are deposited on the walls of the artery, which over time block the lumen of the vessel. Also, occlusion of the femoral artery can be caused by injury, blood clot, and some other reasons.
Factors contributing to the development of occlusion
, are:
- smoking;
- high blood pressure;
- hereditary predisposition;
- improper diet (fatty foods);
- diabetes.
Is preparation required for the procedure?
Ultrasound examination of the arteries of the lower extremities does not require special preparation. But still, for maximum information content, experts give some recommendations:
- If you are taking any medications that affect blood vessels, they should be discontinued a day before the procedure (of course, this must be agreed with your doctor);
- Two days before the procedure, it is necessary to exclude alcohol-containing drinks;
- 5 hours before the test you should not smoke;
- On the day of ultrasound diagnosis and the day before, try not to perform heavy physical activity and avoid long walks;
- 2-3 days before the procedure, it is advisable to limit black tea, coffee and other tonic drinks;
If you have previously had vascular examinations of the lower extremities, take the results with you. Also don't forget your passport and outpatient card.
How is ultrasound of the arteries of the lower extremities performed?
Upon arrival to the ultrasound diagnostic room, the patient must remove clothing below the waist. The doctor will then ask you to lie down on a flat couch with your legs as relaxed as possible. A special gel is applied to the skin. Please note that the lower limbs must be motionless during diagnosis - movement may distort the results of the study. Depending on the purpose of this procedure, the doctor may ask you to change your body position, strain your leg, stand up, sit down, etc.
Usually the study takes no more than 20 minutes. The results are delivered to the patient in printed form. If deviations were detected, an image with a localized pathological process is attached to the protocol.
Dopplerography of the vessels of the lower extremities
Doppler is often used when examining blood vessels. Dopplerography allows you to assess the condition and functioning of blood flow. This research method shows the speed of blood flow.
Dopplerography is mandatory for the following complaints:
- With regular leg cramps;
- With severe swelling;
- With a tendency to hematomas.
- For reliable results, the skin of the legs must be smooth. Therefore, it is necessary to get rid of vegetation on the lower extremities.