Dilatation of the left atrium is a special case of cardiomyopathy; it is an abnormal expansion of the organ chamber of the same name with complete or predominant absence of changes in the muscle layer.
More often it is acquired in nature, caused by certain cardiac conditions, less often endocrine, neurogenic.
Total restoration is impossible. Treatment aims to prevent progression, stabilize the general condition and prolong life.
Development mechanism
LA dilatation is not an independent process. It is not considered a nosological unit. How does such a state form?
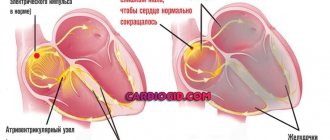
Normally, cardiac structures function continuously, acting as a large pump. The release of blood is ensured by alternating synchronous contraction of all chambers of the heart.
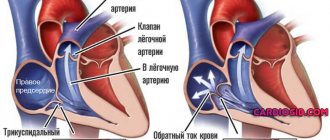
Liquid connective tissue moves in one direction: from the upper to the ventricles, no reverse flow is observed.
As a result of congenital genetic defects, acquired sclerosis of active tissues (replacement of affected areas with scars), a long inflammatory period, etc., blood is retained in the left atrium longer than it should be. Or regurgitation is observed (return of liquid connective tissue from the ventricle).
Over a long period of time, the chamber becomes stretched and the normal dimensions of the organ are disrupted.
This leads to a decrease in release into the systemic circulation, and general and local hemodynamics decrease.
Removed tissues and systems suffer from a lack of oxygen and nutrients. The process of development of organ defects and functional failure begins.
Definition of the concept
The term dilatation means to widen something. A dilated heart means that the chambers of the organ exceed their normal size due to volume or pressure overload. Well, okay, if only that was the end of it. In fact, this condition is considered pathological, leading to the development of various rhythm and conduction disorders and being a potential cause of sudden cardiac death.
Ventricular dilatation
Forms of the disease
Enlargement of the left atrium is classified according to the group of bases. Based on the origin of the pathological process, there are:
- Congenital form. The share of this condition in the total number of recorded clinical situations is 35-40%, which is a minority.
Pathological processes are diagnosed already at advanced stages, since a small patient is not able to formulate his complaints until he grows up, and parents interpret objective manifestations incorrectly due to inattention or lack of experience. The prospects for treatment are therefore somewhat worse.
- Acquired form. Caused by the course of a particular disease. An attentive patient can draw a cause-and-effect relationship between the condition suffered and the development of dilatation symptoms, which are quite pronounced from the second stage.
Degrees of dilatation
Another basis for classification is the degree of pathological abnormalities. Accordingly, they talk about 3 or 4 stages of disease development.
Lightweight
It is formed as a result of a genetic factor, intrauterine defects and acquired conditions.
It is characterized by a complete absence of a clinical picture, which makes diagnosis a matter of chance.
It is possible to identify the initial deformation of the organic plane using echocardiography. It doesn't take much qualification to state a fact.
Determining the root cause falls on the shoulders of the cardiologist and is carried out with the help of a group of measures.
Moderate dilatation
At this stage, the process is diagnosed much more often.
A bright nonspecific picture is typical: shortness of breath, chest pain, arrhythmias. These are common signs of any condition associated with impaired functioning of the heart and blood vessels.
However, the chances of early diagnosis are high, which is good news for the patient.
The prospects for a complete cure are already vague, but with a well-thought-out combination of therapy, the patient will not notice the difference. You can keep the process under complete control.
Marked dilatation of the left atrium
Considered extreme in some national classifications.
It is defined by a vivid clinical picture with a significant decrease in tolerance to physical activity, the inability to adequately work and perform household duties.
Organic defects are gross and are observed not only on the part of the heart; remote systems are also changed.
The prospects for a cure are minimal. At the same time, life expectancy during therapy rarely exceeds 3-4 years.
Terminal phase
This stage occurs quite quickly in the absence of treatment. The approximate period is 4-8 years, sometimes less. Depends on the nature of the pathological process giving rise to dilatation. Palliative care is aimed at ensuring an acceptable, minimum possible level of well-being.
These classifications play an important role in the development of diagnostic tactics and further therapy.
Materials and methods
Of the 16,839 patients included in the “Registry of Coronary Angiography Operations” [5] from 1998 to 2013, patients with stenosis of >75% of the lumen of at least one coronary artery, without acute or anamnestic myocardial infarction, without congenital and acquired heart defects: 75 patients with RV dilatation and 1134 without it. The transverse size of the pancreas in the parasternal position was 26 mm or less [6]. For a clearer division of the groups, patients with pancreatic dilatation included patients with a pancreatic size of 30 mm or more; patients with a slight enlargement of the pancreas (>26 and <30 mm) were not included in the study. A clinical, comprehensive echocardiographic examination was performed (one-dimensional, two-dimensional, Doppler echocardiography using Imagepoint NX ultrasound devices, Agilente Technologies, Phillips, USA; Vivid 3, 4, 7, 9 Systems, Vingmed-General Electric - Horten, Norway), determination of lipid composition of blood serum, Holter monitoring, selective coronary angiography according to Judkins (1967) (angiographic complexes Diagnost ARC A, Poly Diagnost C, Integris Allura, Phillips, Holland). Linear echocardiography (EchoCG) parameters were indexed to height; myocardial mass, calculated using the Devereux formula, to the body surface area [7]. Echocardiographic syndromes were diagnosed according to standard criteria: the LV was considered dilated when its end-diastolic diameter index was more than 32 mm/m2 in women and more than 33 mm/m2 in men [2], LV systolic function was reduced when the LV ejection fraction was less than 50%, hemodynamically significant mitral regurgitation (≥II degree) - with an effective area of the regurgitant orifice ≥0.2 cm2, regurgitant volume ≥30 ml [8].
Statistical processing of data was carried out using a package of applied statistical programs (SPSS Inc., version 17.0). Indicators are presented in the form M
±
SD
_
The distribution of variables was determined using the Kolmogorov–Smirnov test. To compare values with their normal distribution, t
; for a non-normal distribution, the nonparametric Mann-Whitney test was used.
When analyzing qualitative indicators, Pearson's χ2 test was used. Differences at p
<0.05 were assessed as statistically significant. Multivariate analysis was performed - binary logistic regression analysis with calculation of odds ratio (OR).
How dangerous is the pathology?
The condition threatens the development of a group of complications, including:
- Myocardial inflammation. They are formed as a result of blood stagnation and muscle malnutrition.
- Atrial fibrillation and then ventricular fibrillation. Characterizes severe arrhythmia, the functioning of cardiac structures is disrupted. The parallel course of the two processes determines the increased risks of death.
- Formation of blood clots, blockage of large vessels with a blood clot. A typical consequence of dilatation, since stagnation of blood contributes to its thickening.
- Congestive heart failure. In essence, this is dysfunction of a muscular organ of varying severity. It is determined by a group of species that differ in clinical manifestations, prognosis, and recovery prospects.
- Heart attack. Acute malnutrition of cardiac structures and, as a result of tissue necrosis, replacement of functionally active myocyte cells capable of contracting and conducting electrical impulses with rough scars. It is essentially dead tissue. The more it is, the worse the heart works.
- Paroxysmal arrhythmia. Usually of the type of tachycardia (acceleration of the activity of cardiac structures).
- Mitral insufficiency. It suggests possible regurgitation (reverse flow of blood from the ventricles into the atria), disruption of the functional activity of the organ and blood output, and a drop in hemodynamics. Lethal outcome is a matter of time.
- Cardiogenic shock. Acute, urgent condition. Requires urgent assistance, but the chances of the patient returning are almost negligible. Even if you are lucky, death will occur within a few years. Exceptions can be counted on one hand throughout the entire solid practice of doctors around the planet.
- Heart failure. Asystole.
Preventing the development of complications is one of the goals of treatment at any stage. It is best addressed early.
Causes
Factors are always pathological. Some of them are brought to life by the patient himself.
Excessive exercise
Lead to the formation of the so-called athlete's heart. This is a combination of dilatation of several chambers with an increase in mass in the muscle layer.
Truncated options are possible. Both professionals and outdoor enthusiasts suffer. In principle, this is a relatively normal condition. The body adapts to changes.
But more often, gross asymmetry occurs, since physical activity and its mode are selected incorrectly. Inadequate loads result in dysfunction.
Any pathology of the mitral valve
Accompanied by reverse reflux of blood (regurgitation of the MV). Usually these are congenital malformations of the anatomical structure: prolapse, stenosis.
Slightly less often, the condition turns out to be secondary, acquired as a result of inflammatory pathologies, rheumatism and other similar ones, associated with gross tissue destruction over a long or short period of time (heart attack).
Burdened heredity
A predisposition to cardiac pathologies is transmitted. The more relatives suffering from diseases of the cardiovascular system are present in the history, the higher the likelihood. At the same time, no one gives a guarantee of pathology.
Perinatal developmental disorders, genetic syndromes
They are formed at the time of the formation of cardiac structures. The latter are more often characterized by generalized disorders of many organs and systems.
Recovery is very difficult, and in some cases it is completely impossible.
Arterial hypertension
It provokes an increase in the load on the heart and blood vessels, leading to a decrease in tissue elasticity and gross organic defects.
Classic anatomical changes in cardiac structures are left ventricular hypertrophy (proliferation of the muscle layer without increased activity), as well as dilatation of the corresponding atrium.
The guarantee of preventing such an outcome is determined by early treatment of the underlying disease with the use of antihypertensives and protectors.
Neoplastic processes in cardiac structures
Relatively rare, but possible. More often, tumors of this localization turn out to be benign, but this characteristic is very conditional: compression and a decrease in the intensity of the work of cardiac structures are observed. Dilatation of the left atrium chamber is a relatively late complication.
Long-term dangerous forms of arrhythmia
From fibrillation to atrial extrasystole. The development of the pathological process is associated not with the violation of the frequency of contractions itself, but with organic tissue defects.
Narrowing of the aorta
Congenital forms of deviation or an acquired process are possible.
It is characterized by insufficient release of blood into the main artery of the body. Hence the congestion in the ventricle.
At an advanced stage of the process, there is so much liquid connective tissue that it puts pressure on the atrium valve and eventually flows back into the previous chamber, stretching and increasing its volume.
This is a chain process that needs to be stopped at an early stage.
Inflammatory pathologies of the heart
Usually the myocardium is affected, less often other structures. They are of infectious origin, and to a lesser extent autoimmune. Both options are dangerous and require hospital treatment.
“Bonus” are pathological factors of a subjective, controllable kind: smoking, consumption of alcoholic beverages, coffee, excessive stress on a long-term basis, drug addiction, improper treatment with certain drugs.
The causes of left atrium dilatation are eliminated by preventive methods: management of the underlying disease or elimination of an addiction as a priority.
A paradoxical phenomenon is often observed: the pathological process starts for a specific reason and aggravates itself.
Discussion
It is known that ventricular dilatation after MI is more pronounced in patients with a larger area of LV myocardial damage [9]. Therefore, in patients with coronary artery disease, one can expect to find a connection between RV dilatation and multiple coronary stenoses or with a larger size of LV asynergia. RV MI often develops as a result of damage to the proximal part of the non-dominant right coronary artery [10, 11], so RV dilatation in our patients could be associated with damage to this localization in the left type of coronary circulation. However, there were no intergroup differences in the type of coronary circulation, the prevalence or localization of coronary lesions, and the LV asynergia index. The negative relationship between right ventricular dilatation and the FC of angina pectoris necessitates further study.
An increase in the size of the pancreas in patients with coronary artery disease can serve as a sign of increased pulmonary vascular resistance and load on the pancreas, determined by the condition of the left chambers of the heart [2]. Left ventricular dysfunction, causing postcapillary pulmonary hypertension, is the most common cause of right ventricular dilatation [8]. In the present study, LV systolic dysfunction was observed in 25% of patients with dilated RV, and it was the strongest predictor of RV enlargement in multivariate analysis.
The risk of RV dilatation also increased with NRPS, significant mitral regurgitation and with an increase in the FC of CHF - the same as in patients with MI [3].
Among the factors associated with RV dilatation and not related to the LV condition were male gender and an increase in BMI (the same connections were found in patients with MI [3]). The fact is that obese patients often develop obstructive sleep apnea syndrome due to hypoventilation and hypercapnia, accompanied by the development of pulmonary hypertension and, as a consequence, pancreatic dilatation [12]. Perhaps it is this factor that explains the connection between pancreatic dilatation and obesity.
A limitation of this study was that the only parameter of the pancreas was analyzed - its transverse size in the parasternal position. This is explained by the fact that the collection of data for the Register began in 1998, when not all patients had other indicators characterizing the structure and function of the pancreas. The point of our study is to use a large amount of material to study the general patterns of the course of IHD, in particular the factors associated with pancreatic dilatation in a specific population. Inclusion in the analysis only of patients with a complete set of pancreatic characteristics would significantly reduce the sample and would not allow obtaining the most reliable result. Thus, limitations of the study stem from its retrospective nature. Since P.Zh. is a chamber that is extremely sensitive to changes in afterload, and the assessment of the size of the pancreas is an integral part of the characteristics of its function [13], we consider it possible to judge the state of the pancreas by assessing its linear size alone.
Symptoms
An approximate list of signs is as follows:
- General weakness, decreased performance, inability to adequately perform current duties around the house and in everyday life in general.
- Dyspnea. Disruption of normal gas exchange. First, in a state of intense or moderate physical activity, then at complete rest. This affects the quality of life and productivity in various areas.
- Swelling of the lower extremities. As a result of impaired functional (filtering) activity of the kidneys. The volume of circulating blood increases, and fluid is poorly evacuated from the body. The intensity of the symptom depends on the stage of the pathological process.
- Arrhythmias. Subjectively, it makes itself felt as an acceleration of the heart rate, skipping beats, fluttering in the chest with a feeling as if cardiac activity is about to stop.
- Paleness of the skin.
- Cyanosis of the nasolabial triangle. It always develops and does not characterize the degree of pathological activity.
At the first and second stages, there are no generalized disorders, therefore there are no symptoms at all or they are scanty (the moderate phase gives a chance to recognize the condition).
The patient becomes a hostage to the situation. Even at stage 2, physical activity can cause death due to cardiac arrest.
Signs of dilatation are not specific enough: they are characterized by manifestations from the muscular organ itself, the nervous system and the excretory tract.
How is the presence of dilatation determined?
Minor dilatation is, as a rule, an asymptomatic pathology. In this case, patients do not present any complaints that could lead one to suspect the presence of enlargement. But if, as a result of this pathological process, the pumping function of the heart decreases, then the patient may show signs of heart failure: weakness, fatigue, shortness of breath, swelling of the extremities, etc.
Signs of dilatation can be determined by the results of an ECG, but it is impossible to accurately identify it only with the help of this examination. The main method for this is ultrasound of the heart. It helps to detect a previous heart attack or heart defects, and this, in turn, indicates the presence of enlargement. Using ultrasound, the diameter of the ventricle is also measured (in other words, its end-diastolic size - EDS).
However, it should be taken into account that the GDR is not an absolute indicator. With an average norm of 56 mm, it can vary depending on the height, weight and physical fitness of a particular person. If for a two-meter athlete weighing more than 100 kg the norm may be 58 mm, then for a woman weighing 45 kg and reaching a height of only 155 cm, this figure is already a sign of dilatation.
- What is dilatation of the left atrium cavity: causes, symptoms, treatment and prognosis
Diagnostics
The examination of patients is carried out under the supervision of a cardiologist, as necessary, a group of other specialists.
Approximate list of events:
- Oral questioning of the patient and collection of anamnestic data. It is necessary to establish many factors that would play a role.
- Measurement of blood pressure (possibly an increase or decrease), heart rate (tachycardia is typical, flowing in parallel with various types of arrhythmias).
- Daily monitoring. Registration of blood pressure levels for 24 hours. Used for early diagnosis.
- Electrocardiography. Plays the same role. Shows the degree of deviations from the cardiac structures.
- Echocardiography. Basic technique. It makes it possible to identify organic defects at first glance, determine their degree, and predict complications.
- MRI if there is a suspicion of a tumor process in the heart.
Stress tests are not performed due to the possible cessation of muscle function and sudden death.
Treatment
Mixed therapy. Conservative methods are used at an early stage, a combination of surgery and medication in the advanced phase of the pathological process.
The following medications are prescribed:
- Antiarrhythmic. Like Amiodarone, it is the safest. They are used to restore an adequate, correct heart rate.
- Antihypertensives if high blood pressure occurs. Enap, Diltiazem, Perindopril will do. The combinations are different.
- Diuretics to normalize the evacuation of fluid from the body.
- Cardiac glycosides. Stabilize myocardial contractility.
- Antithrombic drugs of various types.
Surgical intervention is aimed at stopping the root cause or installing a pacemaker for severe arrhythmia.
Excision of pathologically altered tissues against the background of tumor lesions is possible. Specific techniques are determined by a specialist based on the underlying disease.
The last resort if the heart is significantly changed is transplantation. However, this is not an easy undertaking.
In addition to the fact that finding an organ is almost impossible in the conditions of Russian reality, the operation requires the highest qualifications, which only a few have.
During the treatment process, also during the recovery period, which lasts a lifetime, you need to minimize the amount of salt in the diet (6-7 grams), give up smoking, alcohol, and normalize physical activity (maximum: walking in good weather).
Forecast
At an early stage, also with a moderate degree of dilatation of the left atrium, the outcome is most favorable. In this case, the patient may exist and be unaware of the problem for decades.
The survival rate over a 10-year period is no more than 25%, in extreme cases it is slightly higher, but this is rather an error. Without treatment, even less.
The general prognosis is unfavorable. Once symptoms of heart failure appear, there is no hope of recovery.
Signs
Slight or moderate atrial dilatation occurs without any clinical symptoms and is usually detected incidentally during an examination for another reason, and is essentially a diagnostic finding.
The main symptom of atrial dilatation is arrhythmias
Significant expansion of the atria is accompanied by a deterioration in their pumping function, which leads to the appearance of arrhythmia and the development of chronic heart failure. Symptoms:
- heart rhythm disturbance;
- dyspnea;
- increased fatigue;
- swelling of the limbs.