Development mechanism
LA dilatation is not an independent process.
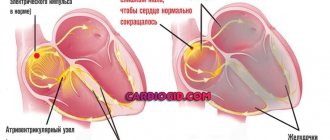
It is not considered a nosological unit. How does such a state form? Normally, cardiac structures function continuously, acting as a large pump. The release of blood is ensured by alternating synchronous contraction of all chambers of the heart.
Liquid connective tissue moves in one direction: from the upper to the ventricles, no reverse flow is observed.
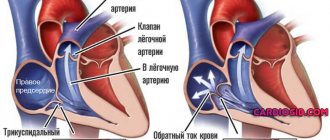
As a result of congenital genetic defects, acquired sclerosis of active tissues (replacement of affected areas with scars), a long inflammatory period, etc., blood is retained in the left atrium longer than it should be. Or regurgitation is observed (return of liquid connective tissue from the ventricle).
Over a long period of time, the chamber becomes stretched and the normal dimensions of the organ are disrupted.
This leads to a decrease in release into the systemic circulation, and general and local hemodynamics decrease.
Removed tissues and systems suffer from a lack of oxygen and nutrients. The process of development of organ defects and functional failure begins.
Possible complications
Dilatation affecting the aortic root or cardiac chamber can cause serious complications. For example, the walls of the heart will stretch and thicken.
Because of this, the following conditions will arise:
- chronic heart failure;
- infectious chronic heart diseases;
- expansion of ring valves;
- thrombosis and much more.
These pathologies worsen a person’s quality of life, and if nothing is done about them, death is possible. Therefore, when they appear, you need to seek help from a cardiologist.
Diagnostics
The examination of patients is carried out under the supervision of a cardiologist, as necessary, a group of other specialists.
- What is dilatation of the left atrium cavity: causes, symptoms, treatment and prognosis
Approximate list of events:
- Oral questioning of the patient and collection of anamnestic data. It is necessary to establish many factors that would play a role.
- Measurement of blood pressure (possibly an increase or decrease), heart rate (tachycardia is typical, flowing in parallel with various types of arrhythmias).
- Daily monitoring. Registration of blood pressure levels for 24 hours. Used for early diagnosis.
- Electrocardiography. Plays the same role. Shows the degree of deviations from the cardiac structures.
- Echocardiography. Basic technique. It makes it possible to identify organic defects at first glance, determine their degree, and predict complications.
- MRI if there is a suspicion of a tumor process in the heart.
Stress tests are not performed due to the possible cessation of muscle function and sudden death.
Symptoms
Symptoms of cardiac enlargement, if slight, are practically unnoticeable because moderate dilatation shows no signs.
If the expansion of the left atrium is too large, the work of the heart deteriorates and the following symptoms occur:
- dyspnea;
- cardiopalmus;
- heart failure;
- fibrillation;
- thromboembolism.
They cannot be called specific, and they are practically invisible. A doctor can identify such a pathology during a preventive examination.
Treatment
Mixed therapy. Conservative methods are used at an early stage, a combination of surgery and medication in the advanced phase of the pathological process.
The following medications are prescribed:
- Antiarrhythmic. Like Amiodarone, it is the safest. They are used to restore an adequate, correct heart rate.
- Antihypertensives if high blood pressure occurs. Enap, Diltiazem, Perindopril will do. The combinations are different.
- Diuretics to normalize the evacuation of fluid from the body.
- Cardiac glycosides. Stabilize myocardial contractility.
- Antithrombic drugs of various types.
Surgical intervention is aimed at stopping the root cause or installing a pacemaker for severe arrhythmia.
Excision of pathologically altered tissues against the background of tumor lesions is possible. Specific techniques are determined by a specialist based on the underlying disease.
The last resort if the heart is significantly changed is transplantation. However, this is not an easy undertaking.
In addition to the fact that finding an organ is almost impossible in the conditions of Russian reality, the operation requires the highest qualifications, which only a few have.
- Why does dilatation of the left ventricle of the heart occur?
During the treatment process, also during the recovery period, which lasts a lifetime, you need to minimize the amount of salt in the diet (6-7 grams), give up smoking, alcohol, and normalize physical activity (maximum: walking in good weather).
Symptoms
Moderate dilatation of the left heart is not accompanied by any symptoms. But with strong expansion, the following signs already appear:
- dyspnea;
- change in heart rate;
- fatigue;
- decreased ability to cope with mental stress;
- constant feeling of weakness;
- swelling of the limbs.
People who engage in professional sports or heavy physical labor have an enlarged left atrium. This is considered normal and does not require treatment. Sometimes patients learn that the chambers are dilated only during a routine examination and do not attach any importance to it because they feel well.
If such a pathology continues to progress, then the person feels not only shortness of breath in a calm state, but also a cough, pain in the chest, increased sweating and surges in blood pressure.
Degrees of dilatation
Another basis for classification is the degree of pathological abnormalities. Accordingly, they talk about 3 or 4 stages of disease development.
Lightweight
It is formed as a result of a genetic factor, intrauterine defects and acquired conditions.
It is characterized by a complete absence of a clinical picture, which makes diagnosis a matter of chance.
It is possible to identify the initial deformation of the organic plane using echocardiography. It doesn't take much qualification to state a fact.
Determining the root cause falls on the shoulders of the cardiologist and is carried out with the help of a group of measures.
Moderate dilatation
At this stage, the process is diagnosed much more often.
- Myogenic dilatation of the heart
A bright nonspecific picture is typical: shortness of breath, chest pain, arrhythmias. These are common signs of any condition associated with impaired functioning of the heart and blood vessels.
However, the chances of early diagnosis are high, which is good news for the patient.
The prospects for a complete cure are already vague, but with a well-thought-out combination of therapy, the patient will not notice the difference. You can keep the process under complete control.
Marked dilatation of the left atrium
Considered extreme in some national classifications.
It is defined by a vivid clinical picture with a significant decrease in tolerance to physical activity, the inability to adequately work and perform household duties.
Organic defects are gross and are observed not only on the part of the heart; remote systems are also changed.
The prospects for a cure are minimal. At the same time, life expectancy during therapy rarely exceeds 3-4 years.
In patients with AF, the main, and sometimes the only finding is pathology of the atria of the heart.
Hypertrophy (thickening of the fibers) and dilatation (expansion of the cavity) of the atria can be both a cause and a consequence of AF, and can occur due to any heart disease. It is assumed that two main mechanisms are involved in the development of AF, which can coexist separately and simultaneously:
1. The presence of one or more focuses with fast impulses. (Focus is a region of the myocardium that can initiate arrhythmia.) Foci are most often located in the area of the superior pulmonary veins flowing into the left atrium. Foci are also found in the area of the muscular couplings of the pulmonary veins, in the right atrium and rarely in the superior vena cava or coronary sinus, as well as in the Marshall ligament. Dilatation (expansion) of the pulmonary veins is one of the important anatomical factors in the occurrence of AF.
2. The presence of one or many small waves (loops) of excitation of the re-entry type (re-entry is re-entry of excitation). Unlike other arrhythmias, which typically involve a single re-entry loop, multiple loops may be involved in the underlying cause of AF because the dissipation of the wave front as it travels through the atria results in the generation of self-sustaining “daughter waves.”
Electrical remodeling of the atria. If the duration of AF is less than 24 hours, then restoration of sinus rhythm is usually completed successfully, while a longer duration of AF reduces the likelihood of restoration and maintenance of sinus rhythm. These observations gave rise to the popular expression “atrial fibrillation begets atrial fibrillation.” The increased susceptibility to AF is associated with a gradual shortening of the effective refractory period as the duration of the attack increases. This phenomenon is called “electrical remodeling.”
Atrioventricular conduction. The atrioventricular node limits impulse conduction in AF (in the absence of an additional pathway). The frequency of ventricular contractions in AF depends on the properties of the node, as well as the drugs acting on it and the activity of the sympathetic and parasympathetic nervous system.
Clinical conditions predisposing to AF
AF is associated with a variety of cardiovascular conditions that can maintain the arrhythmia.
Arterial hypertension is the most common underlying condition in patients with AF; is found in approximately 2/3 of all patients with AF according to various examinations. Insufficient blood pressure control is a risk factor for the occurrence (first detection) of AF in patients with hypertension and a risk factor for complications of AF: stroke and systemic thromboembolism, even in patients on anticoagulant therapy.
Chronic heart failure, defined as heart failure with dyspnea on exertion (HYHA class II-IV), is detected in 30% of patients with AF. In turn, AF is found in 5-50% of patients with HF. The prevalence of AF increases with the clinical progression of CHF: in patients with NYHA class IV CHF, AF is detected in almost 50% of cases.
Valvular pathology of the heart, especially mitral valve defects (stenosis and insufficiency), which cause overload of the left atrium with pressure or volume and, thus, provoke AF.
Cardiomyopathies (hypertrophic, dilated, right ventricular), including primary electrical heart diseases (long QT syndrome, short QT syndrome, Brugada syndrome and catecholaminergic VT), carry a high individual risk of developing AF.
Congenital heart disease (CHD) and atrial septal defect (ASD), according to studies, are associated with AF in 10-15% of patients.
Other congenital heart defects are often associated with AF. Patients with a single ventricle, patients who have undergone atrial repair surgery (Masterda procedure), transposition of the great arteries, or patients who have undergone a Fontan procedure have an increased risk of developing AF. Altered atrial anatomy due to primary abnormalities, surgery, or subsequent hemodynamic abnormalities may be a major predisposing factor in the development of AF. In these patients, AF can be severely symptomatic and often difficult to treat.
IHD is present in 20% of cases among patients with AF. Whether CAD itself predisposes to the occurrence of AF is unknown. But it is necessary to take into account that AF in coronary artery disease can be caused by CHF after a myocardial infarction (MI), arterial hypertension. AF is rare in patients with stable coronary artery disease and preserved LV function, but its presence indicates a poor prognosis after MI.
Thyroid dysfunction is an important cause of AF. Studies have shown the relationship between AF, both with hypo- and hyperfunction of the thyroid gland, and with subclinical hyperthyroidism. Free T4 concentration was independently associated with AF.
Obesity is detected in 25% of patients with AF. A meta-analysis of population-based cohort studies found that obese individuals had a 49% higher risk of developing AF compared with nonobese individuals. Among other factors, obesity is associated with hypertension, sleep apnea, COPD and diabetes mellitus. Obesity is the most likely marker of cardiovascular risk associated with, among other things, AF.
Many patients with metabolic syndrome develop AF; on the other hand, this association depends on conditions predisposing to AF (arterial hypertension, obesity).
Sleep apnea is associated with increased intraatrial pressure and dilatation and may predispose to the development of AF.
High height is associated with AF. The mechanism of this phenomenon is unclear, but it is assumed that mechanical distension of the pulmonary veins (PV) and dilatation of the left atrium may contribute to the development of arrhythmia.
Diabetes mellitus, as a condition requiring treatment, is found in 20% of patients with AF. Poorly controlled diabetes may potentially promote atrial cell death and “structural remodeling” and thus be responsible for the maintenance of AF.
Chronic obstructive pulmonary disease (COPD) is detected in 10-15% of patients with AF. In some patients, lung disease may be more a marker of cardiovascular risk in general than a specific predisposing factor for AF. Bronchial cancer can also occur with AF.
Chronic renal failure (CRF) is present in 10-15% of patients with AF. ESRD may increase the risk of complications associated with AF, especially cardiovascular complications. ESRD, diabetes mellitus, and COPD are even more common in patients with persistent AF.
Consequences of AF
Hemodynamic consequences of AF. In AF, three factors can affect hemodynamics: lack of atrial synchrony, erratic ventricular response, and excessively high heart rate. Due to deterioration of atrial contractile function, a significant decrease in cardiac output may be observed, especially in patients with decreased ventricular diastolic filling, arterial hypertension, mitral stenosis, hypertrophic or restrictive cardiomyopathy. In addition to affecting atrial function, the persistently accelerated ventricular rate in AF may cause dilated cardiomyopathy (an arrhythmogenic cardiomyopathy caused by tachycardia).
Thromboembolic consequences of AF. Stroke is the most devastating consequence of AF. Approximately every 5-6th stroke occurs due to AF. The main source of disabling ischemic strokes of cardioembolic etiology in patients with AF are considered to be thrombi that form in the left atrial appendage as a result of blood stasis. Up to 25% of strokes associated with AF may be a consequence of pre-existing cerebrovascular disease and may develop due to thromboembolism from other cardiac sources or atherosclerotic plaques of the aorta.
The mechanism of thrombus formation is associated with a decrease in blood flow velocity in the left atrium. In AF, there is no full atrial systole, the left atrial appendage empties passively, as a result of which the speed of blood flow in its cavity decreases. With a decrease in the LV ejection fraction, the blood flow in the left atrial appendage slows down even more, up to complete stasis (stagnation) of the blood, and the size of the left atrium increases, which in turn promotes thrombus formation.
The quality of life. The quality of life of patients with AF is reported to be significantly worse than that of individuals in the same age group without AF. Restoring and maintaining sinus rhythm is associated with improved quality of life and better exercise capacity in some studies, but not all. In typical studies, the majority of patients with paroxysmal AF perceived that the arrhythmia interfered with their lifestyle, but this perception was not associated with either the duration or frequency of attacks accompanied by clinical manifestations.
Revishvili A. Sh. “Clinical cardiology: diagnosis and treatment”, 2011. edited by Bockeria L.A., Golukhova E.Z.
Dilatation of the left ventricle (LV)
The main reasons for the development of left ventricular dilatation include:
- Overload of the ventricle with excess blood. From the left atrium, blood is pushed into the left ventricle and then into the aorta, the largest arterial vessel in the body. Thus, this chamber is a kind of pump that pumps blood through the systemic circulation. With aortic stenosis or narrowing of the aortic valve, the ventricle has difficulty pushing blood and dilates from overload.
- Pathology of the muscular wall of the ventricle itself, as a result of which it becomes thinner and stretched.
- Myocarditis (inflammatory disease of the heart muscle), arterial hypertension, IHD (coronary heart disease). All these misfortunes thin the muscular wall of the left ventricle, make it flabby and lead to stretching.
However, sometimes the disease begins without any reason. When this develops, it is called dilated cardiomyopathy. This diagnosis is made after excluding all possible causes of dilatation.
How to treat?
As in the case of treatment of atrial dilatation, dilatation of the left ventricle is cured by eliminating the causes that caused it: ischemic heart disease, defect, hypertension. Sometimes irreversible sclerotic or scarring changes can occur in the heart muscle; treatment in this case is aimed at slowing down the development of the disease.
The treatment of moderate dilatation may be based on metabolic therapy, which affects metabolic processes in cells and tissues, but severe cases still require a more serious approach.
The danger of LV dilatation can come from:
- Heart failure;
- Arrhythmias;
- Mitral insufficiency.
Not all forms of LV dilatation can be completely cured, but timely identification of the problem and proper treatment stops the development of the pathology and prolongs the patient’s life.
Right atrium (RA) enlargement
If a person suffers from bronchopulmonary diseases, his bronchi may spasm. The pressure in the vessels of the pulmonary circulation increases, and the right atrium expands compensatoryly. Other causes include: infectious myocardial lesions, pulmonary hypertension, disorders of the pulmonary blood vessels, pathological changes in the heart muscle.
Heart defects (congenital and acquired) can cause an increase in the amount of blood in the atrium and, consequently, dilatation.
To save the patient from pathology, it is necessary to stop the causes that caused it. The fight against dilatation comes down to the fight against the underlying disease that led to it . If the disease progresses, the heart muscle will also suffer. Dilated hypertrophy will develop, and ultimately heart failure.
One of the ways to correct an enlarged right atrium is surgery. However, without treating the underlying disease, a positive effect from the operation cannot be expected. In severe heart failure accompanying dilatation, heart transplantation is recommended.