Heart defects are various anomalies of the valve apparatus, septa, large vessels and individual parts of the heart, causing circulatory disorders.
There are a huge number of heart defects, each of which is dangerous to human health in its own way. Almost always, a heart defect requires surgical intervention.
1 Holter - diagnosis of heart defects
2 Diagnosis of heart defects
3 ECG for heart defects
Structural pathology of the heart can begin to develop in a person in the mother's womb - this phenomenon is called congenital heart disease . The cause is usually chromosomal abnormalities or infections suffered by the mother. From 5 to 8 babies out of a thousand are born with this defect. The defect can be detected through fetal ultrasound.
If the disease appears as a consequence of injury, infection or systemic disease, we are talking about acquired heart disease .
At its core, the defect is a collective name for diseases of different parts of the heart. Both types of heart defects have many subtypes, with varying degrees of severity and consequences for human health.
Aortic heart defects.
Surgical treatment of patients with aortic regurgitation is indicated for all symptomatic patients in NYHA functional class II or higher, with an ejection fraction >20-30% or an end-systolic diameter <55 mm.
An additional indication is also the end-diastolic diameter, approaching 70 mm. Patients with more severe damage to left ventricular contractile function have a significantly higher risk of surgery and postoperative mortality. Aortic valve replacement is indicated for all patients with aortic stenosis who have symptoms of the disease, as well as for asymptomatic patients with a high transvalvular pressure gradient (more than 60 mmHg), an orifice area ≤ 0.6 cm2, coronary or other valvular pathology, up to how left ventricular decompensation develops. Surgical correction of aortic disease is carried out using its prosthetics with mechanical, biological frame and frameless prostheses or cryopreserved allografts.
In some patients, aortic valve reconstruction may be possible. In cases of narrow aortic rings, to achieve optimal hemodynamics, plastic surgery of the aortic root with biological material is performed. Operations are performed using both standard and minimally invasive approaches.
What is heart valve disease?
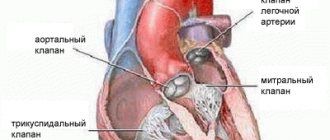
Each heart valve is a complex mechanism that, like gate leaves, opens and closes the flow of blood through the chambers of the heart and from the heart to the aorta and pulmonary artery. Valves allow blood to flow in only one direction.
The human heart consists of four cavities - two atria and two ventricles. Blood enters the atria of the heart through the veins, from the atria to the ventricles, from the ventricles to the large arteries (aorta and pulmonary artery). Along the path of its movement, at the junction of the atria into the ventricles and the ventricles into the arteries, there are heart valves - movable valves consisting of individual elements (cusps). If the heart valve does not work properly, problems with blood flow (in the form of backflow or obstructed blood flow) occur.
The nature of changes in the heart valves can be divided into two groups: - valves that do not close completely (valve insufficiency), which leads to regurgitation (backflow) of blood through the valve in the opposite direction (for example, from the aorta to the left ventricle) and - valves valves that do not open properly (valve stenosis), causing blood flow to become obstructed and restricted.
Valvular heart defects are relatively common, accounting for 20 to 25% of all organic heart diseases in adults. The most frequently detected defects are the mitral valve, the second most common are lesions of the aortic valve. In almost all cases in children and in 90% of cases in adults, the occurrence of the defect is associated with rheumatism. The second most common disease is bacterial endocarditis. Rare causes of the formation of the defect can be systemic lupus erythematosus, scleroderma, rheumatoid arthritis, and in adults - atherosclerosis, coronary heart disease.
Of particular note is a condition that often occurs in healthy people called mitral valve prolapse, or “click syndrome,” “slamming valve syndrome,” “click and murmur syndrome,” “mitral valve aneurysmal bowing syndrome,” “Barlow syndrome,” Engle’s syndrome. and others. Cuffer and Borbillon in 1887 were the first to describe the auscultatory phenomenon of systolic clicks (clicks) of the heart. The term "mitral valve prolapse", which is currently most widespread, was first proposed by J Criley.
The mitral valve blocks the reverse flow of blood from the left ventricle into the left atrium. Prolapse is a condition when the valve leaflets, at the moment of contraction of the ventricle, do not close the hole “tightly”, but bend into the cavity of the atrium, allowing blood to pass in the opposite direction. This is accompanied by a characteristic clicking sound or heart murmur. The amount of blood returning to the atrium can serve as a measure of the severity of the defect.
Depending on when the heart valve defect appeared, primary and secondary prolapse are distinguished: 1. Primary (idiopathic) valve prolapse is congenital, caused by a genetic defect in the structure of the connective tissue that makes up the valve leaflets. 2. Secondary (acquired) heart valve prolapse appears as a result of chest trauma, rheumatism, myocardial infarction and other causes. Today, some experts consider primary mitral valve prolapse to be just a variation of the norm, and not a disease at all.
Mitral heart defects.
Indications for surgery for mitral stenosis are determined by the area of the left atrioventricular orifice. Mitral stenosis with a MV area ≤1 cm2 is considered critical. In physically active patients or patients with large body weight, a narrowing of the opening of 1.2 cm2 may also be critical. Thus, the indication for surgery in patients with mitral stenosis is a reduction in MV area < 1.5 cm2 and NYHA functional class II or more. The indication for surgery for mitral regurgitation is the area of the effective regurgitation opening > 20 mm2 , degree II or more of regurgitation, and NYHA functional class II-III. Surgical treatment of mitral regurgitation should be carried out before the ESI reaches 40-50 ml/m2, since its increase ≥ 60 ml/m2 suggests an unfavorable prognosis.
Surgical correction of mitral disease is carried out using its prosthetics with artificial mechanical and biological prostheses.
When implanting prostheses in patients with severe heart failure, it is necessary to preserve the natural chordal apparatus or implantation of artificial chordae made of polytetrafluoroethylene.
In 30-40% of patients, reconstructive surgery on the mitral valve is possible. For this purpose, various reconstruction methods are used: annuloplasty with hard and soft rings, resection of valves, implantation of artificial chordae, edge-to-edge plastic surgery. Restoration of normal mitral valve function in most patients subsequently does not require lifelong anticoagulant therapy.
Surgeries on the mitral valve are performed both from a standard sternotomy and from a right-sided minithoracotomy.
Mitral-aortic pathologies
Mitral-aortic pathology is characterized by a combination of aortic and mitral defects.
Vice manifests itself in different ways. Most often diagnosed:
- double stenosis;
- insufficiency of one valve and stenosis of the second;
- two combined defects.
This type of disease refers to acquired pathologies and includes a combination of two defects:
- Reduction of the aortic duct at the exit from the heart. This is called aortic stenosis.
- Valvular damage occurs when the leaflets are unable to close completely during diastole. A reverse flow of blood towards the heart is formed.
Stenosis can cause increased blood pressure. With this deficiency, the patient's heart rhythm is disturbed and a systolic murmur appears in the heart.
Tricuspid valve defects.
The indication for surgery for tricuspid valve stenosis is an effective orifice area < 1.5 cm2, and in case of insufficiency, regurgitation of blood into the right atrium of II-III degree. When choosing a method for correcting a tricuspid defect, the presence of predictors of residual pulmonary hypertension in the patient is taken into account: PAP > 50 mm Hg, RV wall thickness > 7 mm, LA diameter > 55 mm, RV EF < 30%.
The main method for correcting relative tricuspid valve insufficiency is annuloplasty. Methods for reducing the diameter of the tricuspid valve ring include purse-string plasty and the use of rigid or flexible correction rings. In some cases, if it is impossible to perform corrective surgery, bioprosthetic valve replacement is used.
Infectious and prosthetic endocarditis.
The etiology of infective endocarditis has changed significantly due to the active use of antibiotics throughout the world. Currently, the main role is given to staphylococci and gram-negative flora, as well as fungal infections.
From the point of view of surgery, in the pathogenesis of infective endocarditis, the fact of rapid destruction of the valvular apparatus of the heart is of greatest importance. This leads to a catastrophic increase in heart failure, since the myocardium does not have time to adapt to the sudden disruption of hemodynamics. The decision on the need for surgical treatment arises, as a rule, with the development of “complicated infective endocarditis”: changes in hemodynamic status; persistence and prevalence of infection; development of metastatic foci of infection; systemic embolisms. In these cases, surgical treatment is more successful than a therapeutic approach. The main problem of surgical treatment is to prevent recurrence of infection and the development of prosthetic endocarditis. The basis for the choice of tactics is the anatomical changes identified on the operating table: the degree of damage to the fibrous ring and surrounding tissues, as well as the presence of vegetations, abscesses, fistulas, and prosthetic separations. In recent years, particular importance has been given to reconstructive operations, especially when the mitral or tricuspid valves are affected by endocarditis. To replace valve defects after surgical treatment, plastic surgery with one’s own tissue, auto- or xenopericardium is used.
Valve structure defects
Combined and associated heart defects are associated with deformation of the valve system. The pathological process may affect the following heart valves:
- aortic;
- mitral;
- tricuspid.
A combined variant is spoken of when the disease manifests itself as stenosis and insufficiency, and it affects only one valve. Combined heart defects are characterized by the development of pathological processes in two, and sometimes in several valves at once. Complex pathologies are more severe and cause serious impairment of cardiac function. Simple defects have a milder course.
Often the defect develops simultaneously in both the mitral and aortic valves. One of the valves is overloaded and suffers more than the other. The combination of mitral and aortic heart defects makes up the majority of all cardiac defects.
Sometimes mitral and tricuspid valve defects are diagnosed; this type of defect is called mitral-triscuspid valve disease. This type of disease is rare. Sometimes the disease affects three valves at once: mitral, aortic, tricuspid; this variant of the disease is diagnosed even less frequently.
Combined heart defects can be either congenital or acquired. Birth defects account for only 1% of the total. They can be diagnosed during fetal development. The disease can lead to the death of a child.
The acquired variant is more common; it develops due to rheumatism; the cause of the disease can be infective endocarditis or trauma to the chest.
Mechanical prostheses.
At the Republican Scientific and Practical Center, two modifications of bicuspid artificial heart valves have been developed and are used in the clinic: PLANIX-T and PLANIX-E. The difference between the design of the latest version of the domestic bicuspid artificial heart valve and the previous model is that the body of the prosthesis is coated with titanium oxide, which ensures high wear resistance and biological inertness. The high height of the rotating mechanism prevents jamming of the valves by heart tissue and made it possible to increase the opening angle of the valves to 900.
Instrumental diagnostics
Today, diagnosis of valvular lesions is carried out mainly using ultrasound. X-ray diagnostics are rarely used; they are mainly needed to determine the dynamics of the heart’s condition before and after surgical intervention. The diagnosis is clarified using MRI of the heart and probing of the cavities of the heart and large vessels. In most cases, they are limited to ultrasound diagnostics. Probing of the cardiac cavities and angiography are relevant if for some reason it is impossible to use non-invasive methods or if echocardiography data and symptoms contradict each other.
Coronary angiography is prescribed for anyone over 40 years of age who is undergoing cardiac valve surgery. EchoCG can be used in two versions: transesophageal and transthoracic. The sensor in the first version is located in the esophagus, next to the basal parts of the heart. The first version of EchoCG is considered clarifying and is carried out only according to strict indications. Doppler echocardiography can detect valvular regurgitation. With good ultrasound access, the aortic valve leaflets are clearly visible on two-dimensional echocardiography. Doppler echocardiography is relevant for detecting aortic regurgitation.