Introductory part
Before heart surgery, a person has many questions. Some of them we ask the doctor, and some we cannot even formulate. When we understand what is happening to our body and what we can do to restore health, it is easier for us to endure all procedures.
Acquired heart valve defects
- these are diseases that are based on morphological and/or functional disorders of the valve apparatus (valve leaflets, annulus fibrosus, chordae, papillary muscles), developed as a result of acute or chronic diseases and injuries, disrupting the function of the valves and causing changes in intracardiac hemodynamics.
Valve defects can be congenital or acquired.
Congenital defects occur when the structures of the heart are formed incorrectly during intrauterine development; sometimes they do not make themselves felt until adulthood. Acquired defects arise due to rheumatism, infection, metabolic disorders (when calcium is deposited in the valves), trauma and other reasons.
The main types of heart valve defects:
- mitral stenosis
- mitral valve insufficiency
- mitral valve prolapse
- aortic stenosis
- aortic valve insufficiency
- tricuspid stenosis
- tricupidal insufficiency
The normal functioning of the heart largely depends on the functioning of its valve apparatus.
Obstacles to the passage of blood cause overload, hypertrophy and expansion of the structures above the valve. Obstructed heart function disrupts the nutrition of the hypertrophied myocardium and leads to heart failure.
Etiology and pathogenesis
Etiology of stenosis
and combined rheumatic disease,
insufficiency
- usually rheumatic, rarely septic, atherosclerotic, traumatic, syphilitic.
Stenosis is formed as a result of cicatricial fusion or cicatricial rigidity of the valve leaflets and subvalvular structures; valve insufficiency - due to their destruction, damage or scar deformation.
Failure
valve damage occurs due to destruction or damage to its valve flaps. Valve insufficiency is characterized by incomplete closure of the leaflets and occurs as a result of their wrinkling, shortening, perforation or expansion of the fibrous valve ring, deformation or separation of the chordae and papillary muscles. In some cases, valve insufficiency develops as a result of dysfunction of the valve apparatus, in particular the papillary muscles.
Often stenosis and insufficiency develop on one valve (the so-called combined defect
).
In addition, there are cases when the defects affect two or more valves - this is called combined
heart disease.
Affected valves form an obstacle to the passage of blood - anatomical in case of stenosis, dynamic in case of insufficiency. The latter is that although some of the blood passes through the hole, it returns back in the next phase of the cardiac cycle.
A “parasitic” volume is added to the effective volume, performing a pendulum-like movement on both sides of the affected valve. Significant valvular insufficiency is complicated by relative stenosis (due to increased blood volume). Obstruction to the passage of blood leads to overload, hypertrophy and expansion of the overlying chambers of the heart.
The expansion is more significant with valve insufficiency, when the overlying chamber is stretched by additional blood. With stenosis of the atrioventricular orifice, the filling of the underlying chamber is reduced (left ventricle with mitral stenosis, right ventricle with tricuspid stenosis); There is no hypertrophy or expansion of the ventricle.
With valve insufficiency, the filling of the corresponding ventricle is increased, the ventricle is dilated and hypertrophied. Difficulty in the functioning of the heart due to improper functioning of the valve and degeneration of the hypertrophied myocardium leads to the development of heart failure.
to the top of the page
Mitral stenosis (mitral valve stenosis)
From the first rheumatic attack to the appearance of complaints characteristic of mitral stenosis in countries with temperate climates, an average of 20 years passes, so complaints usually appear at 30-40 years of age. Increasingly, there are patients in whom the connection between the disease and rheumatism cannot be established. According to data obtained before the widespread use of cardiac surgery, the period from the onset of dyspnea at rest to death usually takes 2-5 years. In developing countries (South and Southeast Asia, Central America, the Middle East), the disease progresses faster and often appears by the age of 20. At the same time, in Western Europe and the USA, slowly progressive mitral stenosis in the elderly is increasingly being detected.
With mild stenosis, there are often no complaints, although physical examination reveals many symptoms of the defect. However, even with a slight increase in the transmitral pressure gradient at rest, an increase in cardiac output (during physical and emotional stress, sexual intercourse, fever, severe anemia, paroxysmal tachycardia, pregnancy, thyrotoxicosis) sharply increases PAWP, causing shortness of breath and cough. A sharp increase in blood flow against the background of severe stenosis leads to pulmonary edema. In the lying position, congestion in the lungs increases, orthopnea and nocturnal attacks of cardiac asthma occur. The smaller the area of the mitral valve opening, the worse patients tolerate physical activity and the higher the likelihood of atrial arrhythmias - extrasystole, paroxysmal tachycardia, atrial flutter, atrial fibrillation.
The high frequency of ventricular contraction during atrial fibrillation causes a sharp increase in shortness of breath. The appearance of a permanent form of atrial fibrillation is a critical moment in the course of the disease; its progression after this is noticeably faster.
Hemoptysis with mitral stenosis occurs due to rupture of the pulmonary veins when the pressure in them increases - usually with high pressure in the left atrium in the absence of a significant increase in pulmonary vascular resistance. Such hemoptysis is almost never fatal; over time, the pulmonary veins thicken and the hemoptysis goes away. It is necessary, however, to distinguish it from other types of hemoptysis, also often found with mitral stenosis and caused by pulmonary edema, pulmonary infarction or bronchitis.
As the disease progresses and pulmonary vascular resistance increases (or due to the addition of tricuspid stenosis or insufficiency), symptoms of pulmonary congestion often weaken, pulmonary edema and hemoptysis occur less frequently and are easier. However, pulmonary hypertension increases the afterload of the right ventricle, and right ventricular failure occurs: weakness, heaviness in the abdomen (due to hepatomegaly), edema, ascites, hydrothorax (usually right-sided).
Repeated pulmonary embolism, sometimes with pulmonary infarction, is one of the main causes of death in mitral stenosis.
Bronchitis, bronchopneumonia, and lobar pneumonia are common. Infectious endocardium is not typical for isolated mitral stenosis, but when stenosis is combined with mitral insufficiency it occurs quite often.
10% of patients have chest pain, usually caused by pulmonary hypertension or coronary artery disease, but often the cause is never found.
Changes in the lungs. In addition to pulmonary hypertension, sclerosis and thickening of the capillaries and alveolar septa often develop. Vital capacity, total lung capacity, maximum ventilation and the ratio of oxygen uptake to MOD decrease. The latter indicator in patients with severe mitral stenosis does not increase during exercise, as it should normally.
The increase in pulmonary capillary pressure during exercise further reduces lung compliance. Sometimes airway resistance increases. All this increases the work of breathing and causes shortness of breath. Due to sclerosis of the alveoli and decreased capillary blood flow, the diffusion capacity of the lungs may decrease, especially during exercise. Effusion into the interstitial space and alveoli also plays a role. Excess fluid is removed due to increased lymphatic drainage, which prevents alveolar pulmonary edema. Due to high pressure in the left atrium, perfusion of the lower parts of the lungs in the standing position is reduced, and the upper parts are increased.
Thromboembolism. Blood clots can occur in the left atrium, especially in its dilated appendage. This is fraught with thromboembolism of the arteries of the brain, kidneys, spleen, and limbs. The risk of thromboembolism is higher in patients with atrial fibrillation, the elderly, low cardiac output, and a history of thromboembolism. Thromboembolism is possible even with mild mitral stenosis and is its first manifestation. After a recent thromboembolism, the likelihood of detecting a thrombus in the left atrium (for example, during surgery) is lower than in the absence of thromboembolism; this suggests that thromboembolism is usually caused by fresh rather than old blood clots. Occasionally, large thrombi on a narrow base and free thrombi block the opening of the mitral valve; the symptoms in this case (fainting, chest pain, dependence of heart murmurs on body position) resemble left atrial myxoma.
Classification. The most widespread classification of mitral stenosis proposed by A.N. Bakulev and E.A. Damir. It includes 5 stages of development of the defect:
- I – stage of complete compensation of blood circulation. The patient does not make any complaints, but an objective examination reveals signs characteristic of mitral stenosis. The area of the mitral orifice is 3-4 cm2, the size of the left atrium is no more than 4 cm.
- II – stage of relative circulatory failure. The patient complains of shortness of breath that occurs during physical exertion, signs of hypertension in the pulmonary circulation are detected, venous pressure is slightly increased, but no pronounced signs of circulatory failure are detected. The area of the mitral orifice is about 2 cm2. The size of the left atrium is from 4 to 5 cm.
- III – the initial stage of severe circulatory failure. At this stage there are phenomena of stagnation in the pulmonary and systemic circulation. The heart is enlarged. Venous pressure is significantly increased. There is an enlargement of the liver. The area of the mitral orifice is 1-1.5 cm2. The size of the left atrium is 5 cm or more.
- IV – stage of pronounced circulatory failure with significant stagnation in the systemic circle. The heart is significantly enlarged in size, the liver is large and dense. High venous pressure. Sometimes slight ascites and peripheral edema. This stage also includes patients with atrial fibrillation. Therapeutic treatment gives improvement. The mitral orifice is less than 1 cm2, the size of the left atrium exceeds 5 cm.
- V – corresponds to the terminal dystrophic stage of circulatory failure according to V.Kh. Vasilenko and N.D. Strazhesko. There is a significant increase in the size of the heart, a large liver, sharply increased venous pressure, ascites, significant peripheral edema, and constant shortness of breath, even at rest. Therapeutic treatment has no effect. The area of the mitral orifice is less than 1 cm2, the size of the left atrium is more than 5 cm.
Anatomy of the heart
A healthy heart is a strong, continuously working organ, about the size of a fist and weighing about half a kilogram.
In addition to maintaining steady, normal blood flow, it quickly adapts and adapts to the body's ever-changing needs.
For example, the heart pumps more blood when it is active and less when it is at rest. During the day, the heart produces an average of 60 to 90 beats per minute - 42 million beats per year!
The heart is a two-way pump that circulates blood throughout the body. It consists of 4 chambers.
A muscular wall called the septum divides the heart into left and right halves. Each half has 2 chambers.
The upper chambers are called atria, the lower chambers are called ventricles. The right atrium receives all the blood returning from the upper and lower parts of the body.
Then, through the tricuspid valve, it sends it to the right ventricle, which in turn pumps blood through the pulmonary valve to the lungs.
In the lungs, the blood is enriched with oxygen and returns to the left atrium, which sends it through the mitral valve to the left ventricle.
The left ventricle pumps blood through the arteries through the aortic valve throughout the body, where it supplies the tissues with oxygen. Oxygen-depleted blood returns through the veins to the right atrium.
Four valves (tricuspid, pulmonary valve, mitral, aortic) act as a door between the chambers, opening in one direction.
These valves help blood move forward and prevent it from flowing in the opposite direction.
The petals of a healthy valve are thin, flexible tissue of perfect shape. They open and close when the heart contracts or relaxes.
Heart valves can become abnormal due to birth defects. They can become damaged or scarred due to rheumatic fever, infection, hereditary factors, age or heart attacks.
The mitral valves are most susceptible to such changes.
Regardless of the case, the heart valve can become stenotic (narrowed opening) or insufficient (does not close completely).
With valve stenosis, the heart must work harder to pump the required amount of blood through the narrowed opening.
Valve insufficiency causes blood to flow backwards through the valve after it closes. Once again, the heart has to work harder to pump enough blood for the body's needs to make up for the deficiency caused by the backflow of blood.
Both cases - stenosis and failure - force the heart to work harder to pump the required amount of blood. This extra work can weaken the heart, cause it to enlarge, and cause various diseases.
to the top of the page
Diagnosis of heart valve diseases
After listening to the symptoms you describe and examining your medical record, the doctor will measure your pulse and blood pressure and listen to your heart using a stethoscope.
If your doctor suspects that you have a heart disease, he may ask you to undergo a series of special diagnostic tests that will help make an accurate diagnosis and prescribe the necessary treatment.
One of these research methods is a non-invasive method, i.e. which does not require any internal intervention.
Another type of research is invasive: with the help of instruments inserted into the body, which, as a rule, causes only minor inconvenience to the patient.
Chest X-ray
This test allows the doctor to obtain valuable information about the size of the heart, heart chambers and the condition of the lungs.
Electrocardiogram (ECG)
An electrocardiogram monitors the electrical current passing through the heart and stimulates the chambers to contract. An ECG is especially useful in diagnosing abnormal heart rhythms and rates.
These studies also show muscle enlargement or damage, and the presence of congestion on one side or another of the heart.
Echocardiogram (EchoCG)
This test is carried out using a “small” microphone placed on the surface of the chest, which emits high-frequency sound waves.
Sound waves are reflected back (hence the term "echo") from each layer of the heart wall and valves and then displayed on a monitor screen. The “echo” image from different points allows you to see a cross-section of the heart at the moment of its operation.
During the echo, the speed of blood flow is also recorded, the direction of blood movement is monitored: is the blood moving in the normal forward direction or is there a reverse movement (as in the case of valve insufficiency).
A narrowed (or stenotic) valve causes increased blood flow. The degree of valve stenosis is in many cases accurately determined by the increased blood flow velocity.
This test will not only show how the heart valves work, it will also provide useful and comprehensive information about the size of the heart chambers, as well as the thickness and function of the heart muscle.
Cardiac catheterization and angiogram
These tests are done by inserting a thin, hollow tube (catheter) through a vein or artery in the arm or groin area and into the chambers of the heart, using X-rays.
During catheterization, the pressure in the chambers of the heart is measured and the volume of blood in the bloodstream is determined.
Angiography consists of the injection of a radiopaque contrast agent, which is visible using X-rays and allows you to evaluate the work of the heart in pumping blood, the function of the valve and the patency of the arteries (coronary) that supply blood to the heart muscle.
Despite the fact that similar studies have been routinely carried out before, it is not at all necessary that they are needed in your case if the information obtained by echocardiography is complete and accurate.
In many cases, the only invasive test required before surgery is a coronary angiogram if it is determined that the patency of one or more arteries is impaired.
If there are blockages in the coronary arteries, the doctor will usually perform bypass surgery at the same time as heart valve surgery.
to the top of the page
Heart valve surgery
Often heart defects do not manifest themselves for a long time, because the heart adapts to working under overload. In the case where the heart defect is “moderate” and does not lead to serious overload of the heart, in some cases they are limited to observation or drug therapy. But when the defect is severe, it must be treated surgically.
The following operations are performed on heart valves: reconstruction or complete replacement of a damaged valve.
Heart valve reconstruction
Sometimes during surgery it is possible to preserve the valve flaps and only correct their shape. This procedure is called valve repair.
.
Sometimes the shape of the valve can be restored by strengthening its base with threads, or by sewing a special ring to the base, while the valve’s own flaps are preserved. This procedure is called annuloplasty.
, it is possible only for the mitral and tricuspid valves.
Valve reconstruction can largely restore its function. For severe heart valve damage, valve replacement surgery may be the only treatment option. The results of these operations exceed the effect of drug therapy. Today, heart valve surgery can be performed on patients of any age group.
Access for operations on the aortic valve or on several valves simultaneously is made through an incision in the center of the sternum. When performing operations on the mitral valve, it is possible to use the “keyhole technique,” when surgical access is made through a small incision in the projection of the mitral valve: on the side and below the chest.
When it is impossible to save the leaflets of the native valve, or if they are preserved, there is a high probability of the defect returning and repeated surgery, the native valve is excised and implanted in its place
artificial
valve prosthesis
.
The most commonly performed surgeries are mitral valve reconstruction. In this case, the own valve is preserved - this is very important.
, Ross surgery is performed to treat aortic disease.
. The damaged aortic valve is replaced with the patient's own pulmonary valve, which is similar in structure, and an artificial prosthesis is implanted instead of the excised pulmonary valve.
When the aortic valve and aortic wall are damaged, it may be necessary to replace the ascending aorta with a valve-containing aortic graft
(sometimes called a conduit). In this case, not only the aortic valve is replaced, but also the adjacent ascending aorta.
Your attending physician will inform you about the possibility of reconstructive surgery on the heart valve in your case. In some cases, the question of the possibility of valve reconstruction is decided during the operation: if reconstruction is not possible, then an operation is performed to replace the damaged valve.
Cardiac surgery for mitral valve defects
Return to section:
Cardiac surgery department
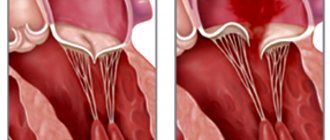
The mitral valve is located between the left atrium and the left ventricle.
Normally, it opens in diastole, allowing arterial blood to pass from the left atrium into the left ventricle, and closes in systole under the influence of blood pressure during contraction of the left ventricle, preventing the reverse flow of blood from the left ventricle into the left atrium.
There are 3 types of mitral valve defects:
1) Mitral insufficiency. With pathology of connective tissue or changes in the heart muscle, a disturbance in the structure of the mitral valve occurs, which leads to “bending” of its valves into the cavity of the left atrium during contraction of the left ventricle, part of the blood flows back into the atrium.
2) Mitral stenosis. Due to infectious diseases such as rheumatism, the MV narrows, which leads to disruption of the flow of blood from the left atrium to the left ventricle.
3) Combined MV defect (insufficiency + stenosis).
Currently, in modern cardiac surgery for mitral valve defects, reconstructive (valve-preserving) operations are performed, as well as operations to replace (prosthetics) valves with a mechanical or biological prosthesis. Reconstructive operations are performed both for stenosis and mitral valve insufficiency.
Reconstructive surgeries
| Fig. 1 . Mitral annuloplasty on a support ring. |
An example is annuloplasty, which involves restoring the function of the affected valve using a rigid or elastic support ring.
It is fixed to the walls of the heart at the level of the opening connecting the atrium to the ventricle. As a result of sewing in such a support ring, the diameter of the atrioventricular orifice decreases, which ensures more complete closure of the valves and normalizes intracardiac blood flow.
Another option for reconstructive surgery on heart valves is surgery using various suture techniques.
During this procedure, the surgeon performs plastic surgery on the valve leaflet tissue, removes calcified deposits, or restores the structure of the altered chordae tendineae, which control the movement of the leaflets.
Rice. 2 .
Suture plasty of the mitral valve. A, B – resection of the altered portion of the posterior mitral valve leaflet; C, D, E – stages of eliminating the gap in the valve.
MK prosthetics.
A radical method of treating the mitral valve is its replacement. Modern mechanical (artificial heart valves) and biological valves are used.
| Mechanical prosthesis MK | Biological prosthesis MK |
Fig.3 . Mechanical (left) and biological (right) mitral valve.
In the case of pronounced morphological changes in the patient’s own valve, when it is no longer possible to preserve it, the valve is removed followed by prosthetics. Surgical replacement of the mitral valve is performed on a non-functioning heart using a heart-lung machine.
Mechanical (artificial heart valves) are very reliable, last a lifetime and do not need to be replaced, but require constant use of special medications to reduce blood clotting.
Biological valves (of animal or human origin) can deteriorate over time, and the lifespan of these valves is highly dependent on the age of the patient and his concomitant diseases. With age, the process of destruction of biological valves slows down greatly. The decision about which valve is the best option in a particular situation is made individually before surgery in a mandatory conversation between the surgeon and the patient.
Technical progress in cardiac surgery, namely the introduction into daily surgical practice of new instruments that make it possible to modify surgical approaches to the heart, inevitably puts forward the goal of performing them with minimal intraoperative trauma for the patient.
Choosing the most rational access to various parts of the heart is one of the necessary conditions for solving this problem.
Online access should ensure the solution of the main tasks:
- provide the surgeon with sufficient space for ease of manipulation in the surgical area;
- surgical access should preferably be less traumatic for the patient.
The traditional surgical approach to the heart is a longitudinal median sternotomy (Fig. 4).
| Diagram of median sternotomy | Type of postoperative scar |
On the one hand, it allows the surgeon to perform the necessary surgical procedures on the heart for various forms of its pathology and is as convenient as possible for connecting a heart-lung machine.
On the other hand, this access may not be optimal. This is due to a number of reasons:
- Greater trauma, the integrity of the chest is compromised, which requires a longer period of healing of the postoperative wound.
- High risk of postoperative complications (sternal instability). These complications are especially dangerous in elderly patients.
- Questionable cosmetic effect.
Fig.5 . View of the surgical field during reconstructive interventions on the mitral valve from a minimally invasive approach to the heart.
All cardiac surgeons will agree that mitral valve reconstruction through a minimally invasive approach (right minithoracotomy) should be performed on the patient with the same skill and quality as when performing operations through a median full sternotomy.
Correction of the mitral valve from a right-sided minithoracotomy is performed in the 4th intercostal space, 6 cm long, in the projection of the 4th intercostal space on the right.
| Scheme for performing a right minithoracotomy | Type of postoperative scar |
Benefits of Minimally Invasive Valve Surgery
- Less pain syndrome. Since access to the heart is through a right lateral minithoracotomy, where the length of the skin incision is about 7 cm, the frame function of the chest is also preserved, i.e. its integrity is not compromised than with the traditional approach - median sternotomy, where the length of the skin incision is about 20 cm, and to perform surgical manipulation of the heart it is necessary to saw the sternum along the midline.
- Reduced risk of complications. Since the chest wall maintains its integrity, the risk of developing complications such as postoperative sternal instability is eliminated.
- Faster recovery and return to normal activities. Less surgical trauma and preservation of the frame function of the chest after minithoracotomy allows for early activation and rehabilitation of patients, which helps reduce the length of hospital treatment.
- The scar is less noticeable. Most patients are very satisfied with the cosmetic results after surgery.
← Back