Classification of heart defects
Depending on different criteria, PPPs vary:
- By etiology (cause of occurrence):
- rheumatic;
due to bacterial endocarditis;
- syphilitic;
- due to expansion of the heart chambers in heart failure;
- traumatic - during injury or surgery;
- after radiation therapy, oranosis of the chest or mediastinum.
- According to the nature of damage to the heart valves:
- valve narrowing - insufficient opening, preventing the movement of blood from one chamber to another;
valve insufficiency, incomplete closure, blood returns to the heart chamber;
- combined – disruption of several valves;
- isolated – changes in the operation of one valve;
- combined - when the valve does not close tightly enough (valve insufficiency) and does not open completely (stenosis or narrowing of the valve) occur simultaneously in one valve.
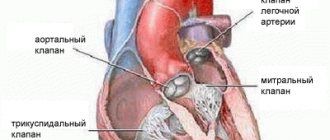
- By localization of defects:
- mitral valve;
tricuspid valve;
- pulmonary valve;
- aortic valve.
- For functional impairment:
- prolapse;
failure;
- stenosis.
- According to the state of the cardiovascular system:
- compensated – there is no circulatory failure;
subcompensated - temporary disruption of blood flow (with increased physical activity, during pregnancy, with increased temperature);
- decompensated - there is a circulatory disorder with the slightest effort and at rest.
Types of pathology
Rheumatic heart disease affects not only the valve apparatus, but also provokes myocarditis, endocarditis or pericarditis.
Emerging heart defects are classified as follows:
- Defects with stenosis. This pathology is characterized by a narrowing of the valve outlet.
- Vices with deficiency. This pathology is characterized by incomplete closure of the valve leaflets when closing.
- Combined defects. They are characterized by insufficiency and stenosis of the aortic valve.
- Combined defects. This pathology is characterized by mitral regurgitation and aortic stenosis.
Symptoms of acquired heart disease
Depending on the type of disease, symptoms may vary, but there are several ailments that are common to most heart defects:
- dyspnea;
- fast fatiguability;
- pressing pain in the heart area (especially during physical activity);
- dizziness;
- swelling of the lower extremities;
- change in skin color;
- dry cough and hemoptysis;
- interruptions in heart function;
- loss of consciousness.
If you notice similar symptoms, consult your doctor immediately. PPPs are very dangerous and can lead to serious consequences. Including heart failure. There is no need to wait until the disease goes away on its own or try to cope with it on your own. Contact the specialists of the cardiology center of the Federal Scientific and Clinical Center of the Federal Medical and Biological Agency, and we will conduct the necessary examination
2.Danger of valve pathology
Any pathology in the mechanics of one or more heart valves inevitably affects the functioning of the myocardium as a whole, and therefore the entire life support system - no matter how stable it may be. The most common negative effect in this sense is that the heart muscle, automatically compensating for blood deficiency and working with constant overload, gradually hypertrophies
– increases in volume, stretches.
As a result, the so-called heart failure to varying (sometimes life-threatening) degrees. Arrhythmia, a tendency to thrombus formation due to blood stagnation, erosion,
etc.
may occur shortness of breath
, i.e. feeling of lack of air. Actually, this is a deficiency of oxygen in the blood, which is not oxygenated or purified properly.
Visit our Cardiology page
Diagnostics
When diagnosing, it is important to collect as much information as possible about the patient: complaints, symptoms, chronic, hereditary or past infectious diseases. Next, the doctor performs a physical examination: the heart and lungs are listened to, blood pressure is measured, and the liver is palpated and measured.
If, after an initial examination and history taking, the doctor discovers characteristic symptoms of heart defects, the patient is referred for additional instrumental studies:
- ECG;
- daily ECG monitoring;
- Echocardiography – ultrasound examination of the heart;
- chest x-ray;
- CT scan of the heart;
- MRI of the heart.
Causes of the disease
As already noted, chronic rheumatic heart disease is an outcome of ARF.
Acute rheumatic fever, in turn, occurs after illnesses such as:
- pharyngitis;
- angina;
- caries.
If the infection develops into a chronic one because it remains untreated, ARF develops. In this case, the human immune system actively produces antibodies that have a damaging effect not only on streptococcus, but also on the heart.
Prevention
Prevention of PPS involves treating the underlying disease that caused the valve damage. To prevent the development of defects, a cardiotrophic diet and lifestyle correction are additionally prescribed:
- refusal of salty, spicy, fatty foods;
- complete cessation of smoking and drinking alcohol;
- moderately active lifestyle;
- control of infectious diseases, including colds;
- annual monitoring by a cardiologist.
All prescriptions and dietary adjustments must be prescribed by your doctor during the treatment process. In our center, the Federal Scientific and Clinical Center of the Federal Medical and Biological Agency, several programs have been developed that will help identify whether you have a heart defect and determine the method of its treatment. You can learn more about the programs here.
How to treat acquired heart disease
Treatment of acquired heart defects is a comprehensive approach, including drug treatment, a special diet, and lifestyle adjustments. If conservative treatment is not enough, surgical intervention is resorted to.
When you contact the center of the Federal Scientific and Clinical Center of FMBA, our doctors will quickly diagnose your disease and prescribe therapeutic treatment. The center has a therapeutic department, where you will be under the constant supervision of specialists. If after the examination it is determined that surgical correction is needed, you will be referred for a consultation with a cardiac surgeon, who will determine whether you need surgery.
Surgical methods:
- Catheter balloon valvuloplasty is the expansion of a narrowed lumen by inserting a balloon catheter. As a result of the operation, the fusion between the valve leaflets is separated, and the obstruction to blood flow is eliminated;
- Valvotomy (commissurotomy) – dissection of fused valves;
- Valve replacement is the replacement of a damaged valve with an implant. Open heart surgery using a machine that temporarily replaces the work of the heart;
- Percutaneous aortic valve replacement.
The main thing in treatment is timely diagnosis. Don’t put off your health for later, seek advice right now.
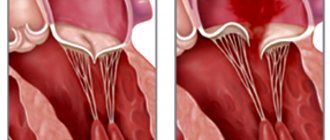
Mitral valve prolapse - symptoms and treatment
Diagnosis criteria
Mitral valve prolapse is most often diagnosed using non-invasive examination methods - the doctor takes into account the patient’s complaints and heredity. But the final diagnosis is made using transthoracic echocardiography.
Instrumental diagnostic methods
During auscultation (listening to the heart) with a stethoscope, the doctor may hear a characteristic systolic click and/or late systolic murmur over the apex of the heart. With the patient standing, the systolic click and murmur appear at the beginning of systole (contraction). With the patient lying or squatting, these sound phenomena are reduced.
The electrocardiogram can detect nonspecific changes in the ST segment and T wave in leads III and aVF. In the presence of mitral valve prolapse, the ECG can diagnose the phenomenon of pre-excitation (“short PQ syndrome”), supraventricular (atrial) tachycardia, and ventricular extrasystole.
chest x-ray Cardiac enlargement may be diagnosed in some patients with a very small anteroposterior chest size.
Transthoracic echocardiography ( Echo-CG) . It is carried out using an ultrasound sensor placed by a doctor on certain points of the chest. It is the most important routine examination in the diagnosis of mitral valve prolapse. Distinctive and important echocardiographic signs of this pathology include deflection of the posterior or both leaflets of the mitral valve into the cavity of the left atrium in mid-systole, in late systole or throughout systole. Deflection (sagging) of the mitral valve in mid-systole is more common, which corresponds to the data obtained by auscultation and angiography.
There are other echocardiographic signs, they are nonspecific, but highly sensitive:
- dilatation (expansion) of the mitral ring;
- increased range of motion of the mitral valve, diastolic contact of the leaflets with the interventricular septum;
- an increase in the range of diastolic divergence of the leaflets and the speed of opening of the anterior valve leaflet;
- systolic displacement of the anterior and posterior leaflets of the mitral valve (more than 3 mm) into the left atrium below the closure of the mitral line;
- thickening of the mitral valve leaflets;
- signs of disruption of the internal structure of the valve tissue (myxomatous valve degeneration);
- reverse blood flow;
- signs of increased pressure in the pulmonary artery.
Transthoracic echocardiography is recommended every 6 to 12 months in all asymptomatic patients with moderate to severe mitral regurgitation. This is necessary to assess the ejection fraction (pumping function of the heart, normally it should be at least 55%) and end-systolic size.
Transesophageal echocardiography. This is an ultrasound test in which a probe is inserted into the esophagus. Indicated only in the absence of contraindications in the following cases:
- Echo-CG does not assess the severity and mechanism of mitral regurgitation and/or the state of left ventricular function;
- The patient is about to undergo valve surgery; during the examination, the question of the nature of the surgical intervention is decided.
A type of prolapse is the so-called valve . It is usually detected by rupture of the chordae or avulsion of the papillary muscle (more common in acute myocardial infarction). With echocardiography in B-mode, the freely moving papillary muscle and the “dangling” mitral valve leaflet are clearly visible. The valve makes irregular, voluntary movements during diastole (the period of relaxation of the heart muscle) and “falls” into the cavity of the left atrium during ventricular systole. In M-mode, characteristic echocardiographic signs of such a valve are the presence of:
- additional echo signals from the mitral valve leaflet in the cavity of the left atrium during the period of ventricular contraction;
- diastolic vibration of the anterior valve leaflet or paradoxical movement of the posterior mitral leaflet in systole and diastole.
Radionuclide equilibrium ventriculography is performed to assess ejection fraction and assess the severity of heart failure. The method is based on the intravenous administration of a radionuclide with its fixation on red blood cells and subsequent quantitative assessment of the contractility of the heart.
Differential diagnosis
The strategy and tactics of patient management depend on the origin of the prolapse - congenital or acquired, therefore differential diagnosis is carried out only between these types of mitral valve prolapse.