In Latin there is a word compensatum, which means “to balance.” Compensatory pause is a term that characterizes the diastolic pause that occurs after a heart rhythm disturbance. In terms of time, such a pause is extended. Its duration is equal to two pauses normal for heart rhythm.
A compensatory pause occurs after the ventricular extrasystole and lasts until the next independent contraction.
Reasons for the occurrence of a compensatory pause
After a ventricular extrasystole, a refractory period is observed, characterized by the fact that the ventricle does not respond to the next impulse emanating from the sinus. This leads to the fact that the ventricle contracts not after the first, but after the second sinus impulse. There are cases when the heartbeat is very rare, the end of the refractory period is observed after the extrasystole and before the next sinus impulse. Such changes in heart rhythm can lead to a lack of compensatory pause.
Heart rhythm can be nomotopic or heterotopic. Their simultaneous presence in a person is called parasystole, which can often cause compensatory pauses.
Another reason for their appearance may be extrasystolic allorhythmia, which is a serious pathology associated with impaired circulatory function and heart rhythm.
Classification
Sinus
Atrial
- atrial
- inferior atrial
- left atrial
From AV connection
- with simultaneous excitation of the atria and ventricles
- with previous excitation of the atria and ventricles:
- retrograde blockade 1st degree
- with complete retrograde block
- with complete anterograde blockade
Ventricular
- septal
- parietal
Types of compensatory pauses
There are two types of compensatory pauses:
- Full.
- Incomplete.
A complete compensatory pause after ventricular extrasystoles appears as a consequence of the fact that the passage of an extraordinary impulse through the atrioventricular node is not observed. The charge of the sinus node is not destroyed.
The next sinus impulse reaches the ventricles at the time when an extraordinary contraction occurs in them. This period is called the refractory period. The ventricles respond only to the next sinus impulse, which is equal in time to two cardiac cycles.
This means that the time indicating the intervals before and after the extrasystoles is equal to two normal intervals R - R.
An incomplete compensatory pause is characterized by the appearance of excitation in the ectopic focus. The impulse reaches the retrograde sinus node, after which the charge formed in it is destroyed. At this moment, another normal sinus impulse is formed. This means that the interval that appears after the extrasystole is equal to one normal R-R interval and the time during which the extrasystolic impulse travels from the ectopic focus to the sinus node. That is, this situation suggests that the distance from the sinus node to the ectopic focus affects the pause after the extrasystole.
The location of the ectopic focus and the atrioventricular node affects the interval of atrial extrasystole P – Q. The location of the node near the focus significantly shortens P – Q.
EXTRASYSTOLIA: clinical significance, diagnosis and treatment
Extrasystoles are called premature complexes (premature contractions) detected on an ECG. According to the mechanism of occurrence, premature complexes are divided into extrasystoles and parasystoles. The differences between extrasystole and parasystole are purely electrocardiographic or electrophysiological. The clinical significance and therapeutic measures for extrasystole and parasystole are absolutely the same. According to the location of the source of arrhythmia, electric systoles are divided into supraventricular and ventricular.
Extrasystoles are undoubtedly the most common cardiac arrhythmia. They are often recorded in healthy individuals. When conducting daily ECG monitoring, the statistical “norm” for extrasystoles is considered to be approximately up to 200 supraventricular extrasystoles and up to 200 ventricular extrasystoles per day. Extrasystoles can be single or paired. Three or more extrasystoles in a row are usually called tachycardia (“jogs” of tachycardia, “short episodes of unstable tachycardia”). Unsustained tachycardia refers to episodes of tachycardia lasting less than 30 seconds. Sometimes the definition of “group” or “salvo” extrasystoles is used to designate 3-5 extrasystoles in a row. Very frequent extrasystoles, especially paired and recurrent “jogs” of unstable tachycardia, can reach the degree of continuously recurrent tachycardia, in which 50 to 90% of contractions during the day are ectopic complexes, and sinus contractions are recorded in the form of single complexes or short short-term episodes of sinus rhythm.
In practical work and scientific research, the main attention is paid to ventricular extrasystole. One of the most well-known classifications of ventricular arrhythmias is the classification of B. Lown and M. Wolf (1971).
- Rare single monomorphic extrasystoles - less than 30 per hour.
- Frequent extrasystoles - more than 30 per hour.
- Polymorphic extrasystoles.
- Repeated forms of extrasystoles: 4A - paired, 4B - group (including episodes of ventricular tachycardia).
- Early ventricular extrasystoles (type “R on T”).
It was assumed that high gradations of extrasystoles (classes 3–5) are the most dangerous. However, further studies found that the clinical and prognostic significance of extrasystole (and parasystole) is almost entirely determined by the nature of the underlying disease, the degree of organic damage to the heart and the functional state of the myocardium. In individuals without signs of myocardial damage with normal contractile function of the left ventricle (ejection fraction greater than 50%), extrasystole, including episodes of unstable ventricular tachycardia and even continuously recurrent tachycardia, does not affect the prognosis and does not pose a threat to life. Arrhythmias in individuals without signs of organic heart disease are called idiopathic. In patients with organic myocardial damage (post-infarction cardiosclerosis, dilatation and/or hypertrophy of the left ventricle), the presence of extrasystole is considered an additional prognostically unfavorable sign. But even in these cases, extrasystoles do not have an independent prognostic value, but are a reflection of myocardial damage and left ventricular dysfunction.
In 1983, JT Bigger proposed a prognostic classification of ventricular arrhythmias.
- Safe arrhythmias are any extrasystoles and episodes of unstable ventricular tachycardia that do not cause hemodynamic disturbances in persons without signs of organic heart damage.
- Potentially dangerous arrhythmias are ventricular arrhythmias that do not cause hemodynamic disturbances in persons with organic heart disease.
- Life-threatening arrhythmias are episodes of sustained ventricular tachycardia, ventricular arrhythmias accompanied by hemodynamic disturbances, or ventricular fibrillation. Patients with life-threatening ventricular arrhythmias usually have significant organic heart disease (or “electrical heart disease,” eg, long QT syndrome, Brugada syndrome).
However, as noted, ventricular extrasystole does not have an independent prognostic value. Extrasystoles themselves are in most cases safe. Extrasystole is even called a “cosmetic” arrhythmia, thereby emphasizing its safety. Even “jogs” of unstable ventricular tachycardia are also classified as “cosmetic” ari (RW Campbell, K. Nimkhedar, 1990). In any case, treatment of extrasystole with antiarrhythmic drugs (AAP) does not improve the prognosis. Several large controlled clinical trials have shown a marked increase in overall mortality and the incidence of sudden death (2-3 times or more) in patients with organic heart disease while taking class I AAP, despite the effective elimination of extrasystoles and episodes of ventricular tachycardia. The most famous study that first identified the discrepancy between the clinical effectiveness of drugs and their impact on prognosis is the CAST study. The CAST study (“Cardiac Arrhythmia Suppression Study”) in patients who had suffered a myocardial infarction, against the background of effective elimination of ventricular extrasystoles with class I C drugs (flecainide, encainide and moricizine), revealed a significant increase in overall mortality by 2.5 times and the incidence of sudden death in 3.6 times compared with patients taking placebo. The results of the study forced us to reconsider the treatment tactics not only for patients with arrhythmias, but also for cardiac patients in general. The CAST study is one of the fundamental studies in the development of “evidence-based medicine.” Only when taking β-blockers and amiodarone was there a decrease in mortality in patients with post-infarction cardiosclerosis, heart failure, or resuscitated patients. However, the positive effect of amiodarone and especially β-blockers did not depend on the antiarrhythmic effect of these drugs.
Detection of extrasystole (as well as any other variant of rhythm disturbances) is the reason for an examination aimed primarily at identifying the possible cause of arrhythmia, heart disease or extracardiac pathology and determining the functional state of the myocardium.
AAPs do not cure arrhythmia, but only eliminate it while taking the drugs. At the same time, adverse reactions and complications associated with taking almost all drugs can be much more unpleasant and dangerous than extrasystole. Thus, the mere presence of extrasystole (regardless of the frequency and “gradation”) is not an indication for prescribing AAP. Asymptomatic or low-symptomatic extrasystoles do not require special treatment. Such patients are advised to undergo clinical observation with echocardiography approximately 2 times a year to identify possible structural changes and deterioration in the functional state of the left ventricle. L. M. Makarov and O. V. Gorlitskaya (2003) during long-term observation of 540 patients with idiopathic frequent extrasystoles (more than 350 extrasystoles per hour and more than 5000 per day) revealed enlargement of the heart cavities in 20% of patients (“arrhythmogenic cardiomyopathy”) . Moreover, enlargement of the heart cavities was more often observed in the presence of atrial extrasystole.
Indications for the treatment of extrasystole:
- very frequent, as a rule, group extrasystoles, causing hemodynamic disturbances;
- pronounced subjective intolerance to the sensation of interruptions in the heart’s function;
- detection during repeated echocardiographic examination of worsening indicators of the functional state of the myocardium and structural changes (decrease in ejection fraction, dilatation of the left ventricle).
Treatment of extrasystole
It is necessary to explain to the patient that asymptomatic extrasystole is safe, and taking antiarrhythmic drugs can be accompanied by unpleasant side effects or even cause dangerous complications. First of all, it is necessary to eliminate all potentially arrhythmogenic factors: alcohol, smoking, strong tea, coffee, taking sympathomimetic drugs, psycho-emotional stress. You should immediately begin to follow all the rules of a healthy lifestyle.
If there are indications for prescribing AAP in patients with organic heart disease, β-blockers, amiodarone and sotalol are used. In patients without signs of organic heart damage, in addition to these drugs, class I AAPs are used: Etatsizin, Allapinin, Propafenone, Kinidin Durules. Ethacizine is prescribed 50 mg 3 times a day, Allapinin - 25 mg 3 times a day, Propafenone - 150 mg 3 times a day, Kinidin Durules - 200 mg 2-3 times a day.
Treatment of extrasystole is carried out by trial and error, sequentially (for 3-4 days) assessing the effect of taking antiarrhythmic drugs in average daily doses (taking into account contraindications), choosing the most suitable one for a given patient. It may take several weeks or even months to evaluate the antiarrhythmic effect of amiodarone (the use of higher doses of amiodarone, for example 1200 mg/day, can reduce this period to several days).
The effectiveness of amiodarone in suppressing ventricular extrasystoles is 90–95%, sotalol - 75%, class IC drugs - from 75 to 80% (BN Singh, 1993).
The criterion for the effectiveness of AAP is the disappearance of the feeling of interruptions and improvement of well-being. Many cardiologists prefer to start selecting drugs by prescribing β-blockers. In patients with organic heart disease in the absence of effect from β-blockers, Amiodarone is used, including in combination with the former. In patients with extrasystole against the background of bradycardia, the selection of treatment begins with the prescription of drugs that accelerate the heart rate: you can try taking pindolol (Wisken), aminophylline (Teopek) or class I drugs (Etatsizin, Allapinin, Kinidin Durules). Prescribing anticholinergic drugs such as belladonna or sympathomimetics is less effective and is accompanied by numerous side effects.
In case of ineffectiveness of monotherapy, the effect of combinations of various AAPs in reduced doses is assessed. Particularly popular are combinations of AAPs with β-blockers or amiodarone.
There is evidence that the simultaneous administration of β-blockers (and amiodarone) neutralizes the increased risk from taking any antiarrhythmic drugs. In the CAST study, there was no increase in mortality in patients after myocardial infarction who took β-blockers along with class IC drugs. Moreover, a 33% reduction in the incidence of arrhythmic death was found!
The combination of β-blockers and amiodarone is especially effective. With this combination, there was an even greater reduction in mortality than with either drug alone. If the heart rate exceeds 70–80 beats/min at rest and the P–Q interval is within 0.2 s, then there is no problem with the simultaneous administration of amiodarone and β-blockers. In the case of bradycardia or AV block of I-II degree, the administration of amiodarone, β-blockers and their combination requires the implantation of a pacemaker operating in DDD (DDDR) mode. There are reports of increased effectiveness of antiarrhythmic therapy when combining AAP with ACE inhibitors, angiotensin receptor blockers, statins and omega-3-unsaturated fatty acids.
Some controversy exists regarding the use of amiodarone. On the one hand, some cardiologists prescribe amiodarone as a last resort - only if there is no effect from other drugs (believing that amiodarone quite often causes side effects and requires a long “saturation period”). On the other hand, it may be more rational to start selecting therapy with amiodarone as the most effective and convenient drug to take. Amiodarone in low maintenance doses (100–200 mg per day) rarely causes serious side effects or complications and is likely to be safer and better tolerated than most other antiarrhythmic drugs. In any case, in the presence of organic heart disease, the choice is small: β-blockers, amiodarone or sotalol. If there is no effect from taking amiodarone (after a “saturation period” - at least 600-1000 mg / day for 10 days), you can continue taking it at a maintenance dose of 0.2 g / day and, if necessary, evaluate the effect of sequential addition Class I C drugs (Etatsizin, Propafenone, Allapinin) in half doses.
In patients with heart failure, a noticeable decrease in the number of extrasystoles may be observed while taking ACE inhibitors and Veroshpiron.
It should be noted that daily ECG monitoring to assess the effectiveness of antiarrhythmic therapy has lost its importance, since the degree of suppression of extrasystoles does not affect the prognosis. In the CAST study, a pronounced increase in mortality was noted against the background of achieving all criteria for a complete antiarrhythmic effect: a reduction in the total number of extrasystoles by more than 50%, paired extrasystoles by at least 90%, and complete elimination of episodes of ventricular tachycardia. The main criterion for the effectiveness of treatment is improvement in well-being. This usually coincides with a decrease in the number of extrasystoles, and determining the degree of suppression of extrasystoles is not important.
In general, the sequence of selection of AAP in patients with organic heart disease, in the treatment of recurrent arrhythmias, including extrasystole, can be presented as follows.
- β-blocker, amiodarone or sotalol.
- Amiodarone + β-blocker.
- Combinations of drugs:
- β-blocker + class I drug;
- amiodarone + class I C drug;
- sotalol + class I C drug;
- amiodarone + β-blocker + class I C drug.
In patients without signs of organic heart disease, you can use any drugs, in any sequence, or use the scheme proposed for patients with organic heart disease.
Brief characteristics of the AAP
β-blockers. Since the CAST study and the publication of a meta-analysis of studies on the use of class I antiarrhythmic drugs, which showed that almost all class I antiarrhythmic drugs can increase mortality in patients with organic heart disease, beta-blockers have become the most popular antiarrhythmic drugs.
The antiarrhythmic effect of β-blockers is due precisely to the blockade of β-adrenergic receptors, i.e., a decrease in sympathetic-adrenal effects on the heart. Therefore, β-blockers are most effective for arrhythmias associated with sympathetic-adrenal influences - the so-called “catecholamine-dependent” or “adrenergic arrhythmias”. The occurrence of such arrhythmias is usually associated with physical activity or psycho-emotional stress.
Catecholamine-dependent arrhythmias in most cases are simultaneously “tachydependent,” i.e., they occur when a certain critical heart rate is reached, for example, during physical activity, frequent ventricular extrasystole or ventricular tachycardia occur only when the sinus rhythm reaches 130 beats per minute. When taking a sufficient dose of β-blockers, the patient will not be able to achieve a rate of 130 beats/min at any level of physical activity, thus preventing the occurrence of ventricular arrhythmias.
β-blockers are the drugs of choice for the treatment of arrhythmias in congenital long QT syndromes.
For arrhythmias not associated with activation of the sympathetic nervous system, β-blockers are much less effective, but the addition of β-blockers often significantly increases the effectiveness of other antiarrhythmic drugs and reduces the risk of the arrhythmogenic effect of class I antiarrhythmic drugs. Class I drugs in combination with β-blockers do not increase mortality in patients with cardiac damage (CAST study).
For so-called “vagal” arrhythmias, β-blockers have an arrhythmogenic effect. “Vagal” arrhythmias occur at rest, after eating, during sleep, against the background of a decrease in heart rate (“brady-dependent” arrhythmias). However, in some cases, for brady-dependent arrhythmias, the use of pindolol (Wisken), a β-blocker with intrinsic sympathomimetic activity (ISA), is effective. In addition to pindolol, β-blockers with BCA include oxprenolol (Trazicor) and acebutolol (Sectral), however, the internal sympathomimetic activity is expressed to the maximum extent in pindolol.
Doses of β-blockers are adjusted according to their antiarrhythmic effect. An additional criterion for sufficient β-blockade is a decrease in heart rate to 50 beats/min at rest. In previous years, when the main beta-blocker was propranolol (Anaprilin, Obzidan), there were cases of effective use of propranolol for ventricular arrhythmias in doses of up to 960 mg/day or more, for example up to 4 g per day! (RL Woosley et al., 1979).
Amiodarone. Amiodarone tablets 0.2 g (the original drug is Cordarone) has the properties of all four classes of AAP and, in addition, has a moderate a-blocking effect. Amiodarone is undoubtedly the most effective antiarrhythmic drug available. It is even called an “arrhythmolytic drug.”
The main disadvantage of amiodarone is the high frequency of extracardiac side effects, which, with long-term use, are observed in 10–75% of patients. However, the need to discontinue amiodarone occurs in 5–25% (JA Johus et al., 1984; JF Best et al., 1986; WM Smith et al., 1986). The main side effects of amiodarone include: photosensitivity, changes in skin color, dysfunction of the thyroid gland (both hypothyroidism and hyperthyroidism), increased activity of liver transaminases, peripheral neuropathies, muscle weakness, tremor, ataxia, visual impairment. Most of these side effects are reversible and disappear after discontinuation or reduction of the dose of amiodarone. Hypothyroidism can be controlled by taking levothyroxine. The most dangerous side effect of amiodarone is lung damage (“amiodarone lung disease”)—interstitial pneumonitis or, less commonly, pulmonary fibrosis. In most patients, lung damage develops only with long-term use of relatively large maintenance doses of amiodarone - more than 400 mg/day. Such doses are extremely rarely used in Russia. The maintenance dose of amiodarone in Russia is usually 200 mg/day or even less (200 mg per day, 5 days a week). B. Clarke et al (1985) report only three cases out of 48 observations of the occurrence of this complication while taking amiodarone at a dose of 200 mg per day.
The effectiveness of dronedarone, a non-iodine derivative of amiodarone, is currently being studied. Preliminary data indicate that dronedarone has no extracardiac side effects.
Sotalol. Sotalol (Sotalex, Sotahexal) tablets 160 mg is used in an average daily dose of 240–320 mg. Start with 80 mg 2 times a day. For refractory arrhythmias, sotalol up to 640 mg/day is sometimes used. The β-adrenergic blocking effect of sotalol appears starting at a dose of 25 mg.
While taking sotalol, there is an increased risk of developing ventricular tachycardia of the “pirouette” type. Therefore, it is advisable to start taking sotalol in a hospital. When prescribing sotalol, it is necessary to carefully monitor the QT interval, especially in the first 3 days. The corrected QT interval should not exceed 0.5 s. In these cases, the risk of developing pirouette-type tachycardia is less than 2%. With an increase in the dose of sotalol and the degree of prolongation of the QT interval, the risk of developing torsade de pointes (TdP) increases significantly. If the corrected QT interval exceeds 0.55 s, the risk of torsade de pointes reaches 11%. Therefore, if the QT interval prolongs to 0.5 s, it is necessary to reduce the dose of sotalol or discontinue the drug.
The side effects of sotalol correspond to the typical side effects of β-blockers.
Ethacizin. Etatsizin tablets 50 mg. The most studied domestic drug (created in the USSR). It has been used for the treatment of arrhythmias since 1982. The rapid achievement of a clinical effect makes it possible to successfully use Etatsizin in people without organic heart disease for the treatment of ventricular and supraventricular rhythm disturbances: extrasystoles, all types of paroxysmal and chronic tachyarrhythmias, including atrial fibrillation, and Wolff syndrome. Parkinson-White. Etatsizin is most effective in patients with nocturnal arrhythmias, as well as with ventricular extrasystoles. The average daily dose of Etatsizin is 150 mg (50 mg 3 times a day). The maximum daily dose is 250 mg. When ethacizine is prescribed to prevent recurrence of atrial fibrillation, supraventricular and ventricular tachycardias, its effectiveness, as a rule, exceeds that of other class I FGAs. The drug is well tolerated, the need for discontinuation occurs in approximately 4% of patients. Main side effects: dizziness, headache, numbness of the tongue, impaired gaze fixation. Typically, adverse reactions are observed relatively rarely, and their severity decreases after the first week of taking Etatsizin.
Allapinin. The domestic drug Allapinin, 25 mg tablets (also created in the USSR) has been used in clinical practice since 1986. Prescribed 25–50 mg 3 times a day. The maximum daily dose is 300 mg. Allapinin is quite effective for supraventricular and ventricular arrhythmias. The main side effects are dizziness, headache, impaired gaze fixation. The need for withdrawal occurs in approximately 6% of patients. One of the features of allapinin and theoretically its disadvantage is the presence of a β-adrenergic stimulating effect.
Propafenone (Ritmonorm, Propanorm), tablets 150 mg, ampoules 10 ml (35 mg). Prescribe 150–300 mg 3 times a day. If necessary, the dose is increased to 1200 mg/day. Propafenone, in addition to slowing conduction, slightly lengthens refractory periods in all parts of the heart. In addition, propafenone has a slight β-adrenergic blocking effect and calcium antagonist properties.
The main side effects of propafenone include dizziness, impaired gaze fixation, ataxia, nausea, and a metallic taste in the mouth.
Quinidine. Currently, in Russia they mainly use Kinidin Durules, table. 0.2 g each. A single dose is 0.2–0.4 g, the average daily dose is from 0.6 to 1.0 g. The maximum daily dose of quinidine in previous years (when quinidine was the main antiarrhythmic drug) reached 4. 0 g! Currently, such doses are not used and the approximate maximum daily dose of quinidine can be considered 1.6 g.
In small doses (600–800 mg/day), quinidine is well tolerated. Side effects usually occur at higher doses. The most common side effects when taking quinidine include gastrointestinal dysfunction: nausea, vomiting, diarrhea. Headache, dizziness, and orthostatic hypotension are less common. The most dangerous complication from taking quinidine is the occurrence of ventricular tachycardia of the “pirouette” type. According to the literature, this complication occurs in 1–3% of patients taking quinidine.
P. Kh. Janashia , Doctor of Medical Sciences, Professor S. V. Shlyk , Doctor of Medical Sciences, Professor N. M. Shevchenko , Doctor of Medical Sciences, Professor of Russian State Medical University, Moscow
How does such a phenomenon threaten human health?
A compensatory pause is a cause for concern, and its occurrence always negatively affects the pumping function of the heart. This condition can appear after emotional excitement, drinking a lot of coffee, nicotine abuse, or sleep disturbances.
Of particular danger are compensatory pauses resulting from signals in the area of ischemic and infarct zones. Such cases, judging by statistical data, often lead to the development of spontaneous ventricular fibrillation, which, in turn, ends in the death of the patient.
A compensatory pause may be evidence of serious illnesses:
- heart defect,
- myocarditis,
- ischemic disease,
- myocardial infarction,
- arterial hypertension,
- chronic heart failure.
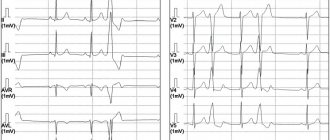
Form
As one might expect, the shape of ventricular extrasystoles depends on the part of the ventricles in which they arise. Extrasystoles from the right ventricle usually resemble LBP block in shape, since the excitation of the left ventricle occurs after the right. Ventricular extrasystoles from the left ventricle, on the contrary, usually resemble PNPG block. The shape of extrasystoles from the interventricular septum is also often similar to LBP blockade.
Treatment
In order to get rid of compensatory pauses, it is important to cure the underlying disease that provoked them. For this purpose, beta-blockers, sedatives and tranquilizers are used, with the help of which extrasystoles are reduced. Drugs based on quinidine cope well with arrhythmia.
In addition, sometimes it is necessary to seek the help of a psychotherapist.
Frequency
The frequency of ventricular extrasystoles is determined per minute or another unit of time. Extrasystoles can be either isolated (isolated episodes of premature depolarization) or frequent.
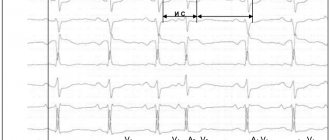
There are various combinations of ventricular extrasystoles. Two extrasystoles in a row (see Fig. 16-4) - a pair, or couplet . Three or more extrasystoles in a row - VT (see Fig. 16-5). Sometimes isolated extrasystoles occur so frequently (see Fig. 16-6) that each normal sinus complex is followed by a ventricular extrasystole. Such repeating groups are called ventricular bigeminy.
The sequence of two normal sinus complexes and a ventricular extrasystole is ventricular trigeminy .
The "R to T" phenomenon
The "R on T" phenomenon describes ventricular extrasystoles coinciding with the apex of the T wave (ventricular extrasystoles can also occur at the lowest point of the negative I wave) of the previous normal complex (Fig. 16-10, see Fig. 16-16).
Rice. 16-10. Ventricular extrasystole (X), close to the apex of the T wave of the previous complex, predisposes to the development of VT and VF. This "R on T" phenomenon is especially dangerous in acute ischemia or myocardial infarction, as well as prolongation of the QT(U) interval (1 - rhythm recording in lead).
Such extrasystoles can contribute to the development of VT or VF, especially in the acute stage of infarction or myocardial ischemia, as well as with prolongation of the QT interval. In the section on electrical cardioversion it is said that the apex of the G wave corresponds to the period when VF is especially likely to occur under the influence of an external stimulus (see Chapter 15). VT and VF, however, are often not associated with the R to T complex. Most of these complexes do not cause persistent ventricular tachyarrhythmia.
Monomorphic and polymorphic ventricular extrasystoles
The terms “monomorphic” and “polymorphic” describe ventricular extrasystoles in any lead. Monomorphic ventricular extrasystoles have the same morphology in one lead and originate from the same anatomical site (focus) (see Fig. 16-6). Of course, the shape of extrasystoles in different leads varies, as with normal complexes. On the contrary, polymorphic ventricular extrasystoles have different shapes in the same lead (see Fig. 16-9).
Rice. 16-9. Polymorphic ventricular extrasystoles differ in shape in one lead (compare with Fig. 16-6, A).
Polymorphic extrasystoles often, but not always, occur in different areas. Monomorphic ventricular extrasystoles are always monotopic, but polymorphic extrasystoles are not necessarily polytopic. Monomorphic ventricular extrasystoles can occur both in healthy individuals and in organic heart diseases. Frequent polymorphic ventricular extrasystoles are often a manifestation of organic heart damage.