Sick sinus syndrome
(SSSU) is a group of cardiac rhythm and conduction disorders characterized by a decrease in the frequency of electrical signals emanating from the sinus node.
The sinus (sinoatrial) node is a source of electrical excitation and the first-order pacemaker of the heart. It is localized in the wall of the right atrium and produces impulses with a frequency of 60-80 per minute. The SA node is subject to the influence of the ANS (autonomic nervous system) and hormonal systems, this is manifested by changes in rhythm adequate to the needs of the body during physical, psycho-emotional activity, sleep or wakefulness.
With sick sinus syndrome, the SA node loses its leading position in generating the heart rhythm.
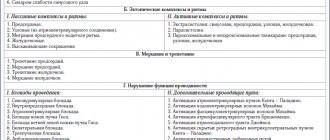
SSSU classification
- According to the etiology,
SG dysfunction is divided into primary and secondary, arising against the background of another pathology. - According to the course:
acute, accompanied by hemodynamic disturbances and severe symptoms; paroxysmal (attack-like) and chronic form. Among the chronic ones, a latent form is distinguished, in which there are no symptoms or ECG signs, and the diagnosis is established only after EPI (electrophysiological study); compensated brady- and tachybrady-form with variants of decompensation; permanent brady-form of atrial fibrillation against the background of sick sinus syndrome. - Based on the presence of clinical manifestations,
SU dysfunction can be asymptomatic or symptomatic. Manifestations of the latter may include AHF (acute heart failure), hypotension, angina pectoris, syncope (fainting), transient ischemic attack as a consequence of impaired cerebral blood supply.
Forms of the disease SSSU
- Sinus bradycardia
- rhythm with a frequency of up to 60 contractions per minute. It is considered the norm for physically trained individuals, athletes, as well as young people with a predominance of vagal influences on the heart. In addition, during sleep there is a physiological decrease in heart rate by 30%. In other cases, bradycardia accompanies various diseases.Moderate bradycardia may not impair blood circulation, but a rhythm with a frequency of less than 40 beats per minute leads to insufficient blood supply and ischemia (oxygen deficiency) of organs and tissues, thereby disrupting their function.
Regardless of the cause, the basis of bradycardia is a violation of the sinus node’s ability to generate electrical impulses with a minute frequency of more than 60 or their incorrect propagation through the conduction system.
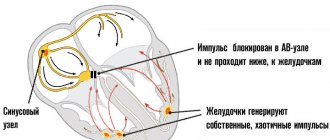
- Sinoatrial block.
With this type of sinus dysfunction, inhibition occurs until the transmission of the electrical wave from the pacemaker to the atria completely stops. In this case, there is an increase in the pause between atrial contractions, their temporary asystole and, as a consequence, the absence of timely contraction of the ventricles, which affects hemodynamics.
The mechanism for the development of blockade can be associated both with blocking the movement of the impulse from the source and with the lack of formation of excitation in the node itself.
- SU stop.
Sinus arrest threatens sudden cardiac arrest. However, more often the role of a source of impulses is taken on by a second order pacemaker (AV node), generating signals with a frequency of 40-60 per minute or a third order (His bundle, Purkinje fibers) with AV block, frequency = 15-40 per minute.
Location and structure
The sinoatrial node consists of a group of specialized cells located in the wall of the right atrium, just transverse to the opening of the vena cavae at the junction where the superior vena cava enters the right atrium. The SA node is located in the myocardium. This deep formation abuts the cardiac myocytes belonging to the right atrium, and its superficial part is covered with adipose tissue.
This elongated structure, which extends 1 to 2 cm to the right of the margin of the appendage, represents the crest of the right atrial appendage, and extends vertically into the superior portion of the terminal groove. SA node fibers are specialized cardiomyocytes that vaguely resemble normal, contractile cardiac myocytes. They have some contractile filaments, but they do not compress as tightly. In addition, the fibers of the SA node are noticeably thinner, more tortuous, and stain less intensely than cardiac myocytes.
Symptoms of SSSU
Clinically significant dysfunction of the sinus node occurs when less than 1/10 of the working pacemaker cells remain.
The clinical picture of SSSU is formed by 2 main groups of symptoms: cardiac
(heart) and
cerebral
(brain).
Patients complain of a feeling of a slow, irregular pulse, a sinking heart, in the case of severe bradycardia, pain in the projection of the heart, a pressing, squeezing nature behind the sternum due to a decrease in blood flow through the coronary arteries. Arrhythmia may occur (paroxysmal tachycardia, supraventricular and ventricular extrasystole, fibrillation, atrial flutter - this is felt by interruptions in the heart, palpitations, “tumbling” of the heart. In an unfavorable course, ventricular fibrillation develops, which is often the cause of sudden cardiac death.
Brain (cerebral) symptoms
in the initial stages of SSSS is presented by nonspecific symptoms: general weakness, fatigue, irritability, emotional instability, decreased memory and attention.
As sick sinus syndrome develops, drowsiness, presyncope, and short-term loss of consciousness (Morgagni-Adams-Stokes attacks) appear, associated with a sharp deterioration in blood supply to the brain. As a rule, such fainting passes on its own.
Dizziness, tinnitus, weakness also progress, the emotional sphere suffers, performance and memory are significantly reduced, and sleep is disturbed.
Naturally, with SSSS, the blood supply not only to the heart and brain deteriorates - other organs also suffer. Kidney function is impaired, the patient notices a decrease in the amount of urine; digestive function is impaired; the tone and strength of skeletal muscles decreases.
Prevention of the syndrome
Based on the above, it is much easier to prevent a disease than to treat it.
The best prevention of the development of SSSS will be strengthening the heart muscle, as well as limiting those substances that affect the functioning of the heart:
- quitting tobacco and alcohol;
- limiting strong tea and coffee;
- a balanced diet that includes foods that have a beneficial effect on heart activity - honey, zucchini, nuts;
- regular exercise and physical activity. This includes walks in the fresh air, exercise and swimming;
- avoiding stressful situations or taking sedatives - infusion of valerian, motherwort;
- refusal to take uncontrolled medications. As mentioned above, they can affect heart rate;
- compliance with safety regulations. For example, ticks can carry Lyme disease, which also affects the sinus node. So, you need to be very careful when you are in the forests and parks in the summer.
For all its frivolity, SSSS is a very serious disease. You should not neglect your well-being and it is better to consult a doctor if the symptoms described above appear more than once or twice a year.
Reasons for SSSU
Primary dysfunction:
- Replacement of cells with connective tissue - cardiosclerosis (post-infarction, post-myocardial, cardiomyopathic).
- Congenital underdevelopment of the sinus node.
- Senile amyloidosis.
- Idiopathic damage, including Lenegra's disease.
Secondary dysfunction:
- Increased vagal tone (vagus nerve): carotid sinus syndrome, sleep apnea, vasovagal syncope, increased intracranial pressure, myocardial infarction of the lower topic, subarachnoid hemorrhage, Bezold-Jarisch reflex, diseases of the larynx and esophagus, cardioversion.
- Effects of drugs: beta-blockers, non-dihydropyridine calcium channel blockers, cardiac glycosides, antiarrhythmics, cholinomimetics, morphine, sodium thiopental, lithium preparations.
- Inflammation of the heart muscle (myocarditis).
- Ischemia of the sinus node.
- Acute injury to the sinus due to right atrium infarction
- Traumatic damage to the cells of the sinus node and conduction system (surgery, injury).
- Electrolyte disturbances.
- Blood gas disturbances (hypoxemia, hypercapnia).
- Dysfunction of hormonal systems (most often hypothyroidism).
Diagnosis of SSSU
- An ECG
showing bradycardia of sinus origin with a frequency of up to 40 beats per minute during the day and less than 30 beats per minute at night may indicate sinus dysfunction. SA blockade, pauses of more than 3 seconds, tachy-bradycardia syndrome, migration of the pacemaker through the atria allow us to suspect a weakening of the pacemaker. - A more informative diagnostic method is Holter ECG monitoring
. It allows you to analyze the heart rhythm for a whole day or more, track the connection of disturbances with exercise, taking medications, and identify provoking factors. - In difficult situations, when dysfunction of the SU is not permanent, EFI
. An electrode is inserted into the patient's esophagus, with which the atria are stimulated to a frequency of 140-150 beats per minute, thereby suppressing the activity of the natural pacemaker and observing the time it takes to restore the function of the sinus node after cessation of stimulation.
EchoCG is used to detect organic myocardial pathology
(ultrasound of the heart), less often cardiac tomography.
Opening
On a hot summer day in 1906, Martin Flack, a medical student, studied microscopic sections of a mole's heart while his mentor, Arthur Keith, and his wife cycled through the beautiful cherry orchards near their cottage in Kent, England. Upon his return, Flack excitedly showed Keith “the wonderful structure he had discovered in the mole’s right atrial appendage, exactly where the superior vena cava enters that chamber.” Keith quickly realized that this structure closely resembled the atrioventricular node described by Sunao Tawara earlier this year. Further anatomical studies confirmed the same structure in the hearts of other mammals, which they called the “sinusoidal node” (sino-auricular node). Finally, the long-awaited heart rate generator was discovered.
Beginning in 1909, using a two-string galvanometer, Thomas Lewis simultaneously recorded data from two sites on the surface of a dog's heart, making precise comparisons of the arrival of the excitation wave at different points. Lewis identified the sinusoidal node as the heart's pacemaker through two innovative approaches.
- First, he stimulated the superior vena cava (SVC), coronary sinus, and left appendage and showed that only the waveforms near the sinus node were identical to the normal rhythm.
- Secondly, it was known that the point at which contraction begins becomes electrically negative relative to inactive muscle points. As a result, the electrode near the SAU invariably had a primary negativity indicating: “The nodal area SA is the place where the excitation wave originates.”
Cooling and heating of the sinus node to study the heart rate response was carried out by G Ganter and others, who also indicated the location and primary function of the sinus node. When Einthoven was awarded the Nobel Prize in 1924, he generously mentioned Thomas Lewis, saying: “I doubt that without his valuable contributions I would have the privilege of standing before you today.” [2 - Silverman, ME; Hollman, A. (1 October 2007). "Discovery of the sinus node by Keith and Flack: on the centennial of their 1907 publication]
Treatment of SSSU
Treatment tactics for sick sinus syndrome depend on the degree of sinus node dysfunction, the cause of the disease, clinical manifestations, and the severity of hemodynamic disorders. The secondary nature of the pathology implies treatment of the underlying disease.
For mild and moderate forms of SSSS, medications are used. If medications do not have an effect, or a complex, combined with other rhythm disturbances, or acute, severe form of sinus node dysfunction develops, disrupting regional and systemic circulation, installation of a pacemaker is indicated.
Prices
Since the pathologies are very different, their treatment methods also differ significantly from each other. Vascular surgery in Israel carries out a variety of operations by type, level of complexity, etc. which effectively help eliminate the problem and save a person’s life.
In Israel, the following operations can be performed depending on the type of disease.
For atherosclerosis of the coronary arteries and coronary heart disease, coronary angioplasty combined with stenting, as well as coronary artery bypass grafting, are performed. In case of atherosclerosis of the carotid arteries, they are stenated.
Aortic aneurysm is treated using standard prosthetics, graft stenting, aortic root reconstruction, aneurysm clipping, etc.
Endovasal surgery (obturation with special coils) helps to cure aneurysms and malformations of the cerebral arteries.
For varicose veins, effective methods are laser coagulation, foam sclerotherapy, stripping, etc.
Hemangiomas are treated by excision, sclerotherapy, cryosurgery, or laser surgery.
Prices for vascular surgery procedures in Israel are not very high, which is why treatment in clinics in this country is so popular. The cost will vary significantly depending on the treatment method, equipment and drugs used, doctor, clinic and many other factors. You can send a request to find out data for your specific case. The high level of professionalism of doctors and the use of advanced technologies guarantee a quick recovery.
The main goal is the patient’s speedy recovery and restoration of his ability to work. Treatment conditions are created in such a way that the patient feels completely comfortable - this has a good effect on the treatment process.
Approximate prices for the Department of Cardiology and Cardiac Surgery
| Disease | Approximate price, $ |
| Prices for mitral valve replacement in Israel | 49 200 — 55 720 |
| Prices for treatment of atrial fibrillation | 22 720 — 36 310 |
| Prices for treatment of hypertrophic cardiomyopathy | 39 420 |
| Prices for treatment of thoracic aortic aneurysm | 101 279 — 112 279 |
| Prices for coronary artery bypass surgery | 48 610 |
| Prices for diagnosing hypertension | 5 630 |
| Prices for treatment of abdominal aortic aneurysm | 71 960 — 74 960 |
| Prices for treatment of coronary heart disease | 9 260 — 23 110 |