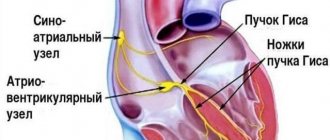
In order to synchronize the contractions of the parts of the heart, conductive pathways pass through them. They are represented by a special type of pacemaker cells that differ from other cardiomyocytes. Their function is to form and transmit nerve impulses through the myocardium to effect heart contraction. If a malfunction occurs in any part, then a person experiences various rhythm disturbances.
The mechanism of human existence
Man as a working multifunctional mechanism. He can perform many actions: eat, drink, walk, sit, look out the window - this list can be endless. The body's vital activity systems are responsible for all of the above. Each organ performs a specific function; it is impossible to replace it with another. Everything is very simple: our eyes are responsible for visual perception, our ears are responsible for auditory perception, our stomach is responsible for digestion, our lungs are responsible for breathing, our brain is responsible for mental and other operations, the spleen and liver are responsible for digestion processes and transport of food in the body, etc. d.
All organs are important and interconnected. Even without one, our body will not be able to function fully, and we, accordingly, will be susceptible to diseases. In the modern world, you can easily determine whether a person is healthy or not. A person’s illness is indicated by the color of his skin, the condition of his teeth, fatigue, exhaustion, etc. Therefore, each of us must take care of our health, namely the proper functioning of our internal organs.
The heart is a vital organ
The heart is a circulatory organ that transports blood through the vessels. It is capable of pumping 4-5 liters of blood per minute. But this is not the final figure; it can reach 30 liters. Based on research data, the weight of the heart is approximately 300 g, width - 7-10 cm, length - 12-13 cm. There is an opinion that if you clench a fist, its circumference will correspond to the size of the heart. But all this is relative and depends on the individual characteristics of the body and the rhythm of life.
The heart is an organ that is involved in transporting nutrients through the blood vessels to the brain and other organs. And as long as it works without deviations, our body does not experience difficulties in its functioning.
But do not forget that this organ does not last forever and can fail and require urgent restoration. Heart problems can appear due to heredity, the influence of the internal environment, alcohol and smoking abuse, frequent stress and lack of sleep, as well as other negative factors. The best prevention is exercise and a proper diet.
FIBER NETWORK PURKINJE
The terminal branches of the right and left bundle branches are connected by anastomoses with an extensive network of Purkinje cells located subendocardially in both ventricles. Purkinje cells are modified myocardial cells that directly communicate with the contractile myocardium of the ventricles. The electrical impulse arriving along the intraventricular pathways reaches the cells of the Purkinje network and from here passes directly to the contractile cells of the ventricles, causing myocardial contraction.
The nerve fibers of the vagus nerve do not reach the network of Purkinje fibers in the ventricles. The cells of the Purkinje fiber network are fed with blood from the capillary network of the arteries of the corresponding region of the myocardium.
Heart structure
The heart consists of four chambers separated by special partitions. The two chambers are the left and right atrium. The sinoatrial node is located in the right atrium. The other two chambers are the left and right ventricles. The right side of the heart, where the right atrium and ventricle enter, is responsible for venous blood, and the left, where the left atrium and ventricle are located, is responsible for arterial blood.
Between the atria and ventricles there is a valve that prevents blood from flowing in the opposite direction. The heart also has vena cavae, which enter the right atrium, and pulmonary veins, which enter the left atrium.
Diseases associated with the atrioventricular node
Atrioventricular node block
The most common atrioventricular disorder is AV block . This is a cardiac arrhythmia that develops due to delayed or interrupted transmission of signals through the atrioventricular node. Often the block goes undetected and in such cases it is usually determined to be a first degree block. However, severe AV block causes the heart to beat very slowly. This phenomenon causes so-called bradycardia, which sometimes turns into temporary cardiac arrest with all the ensuing consequences. To treat such conditions, a pacemaker is usually used, which stabilizes the impaired transmission of impulses. With such a serious disruption of the AV node, they speak of third-degree AV block.
AV node block can be diagnosed using an ECG, where it is expressed as a prolonged PQ interval, depending on the severity. Congenital AV block is extremely rare, but may occur as part of another congenital heart disease. Most AV blocks are acquired. They usually result from degenerative changes in the heart. For example, inflammation or infection of the heart muscle may contribute to the formation of a blockage. Patients with this disease are first treated with medication to eliminate the arrhythmia. If the condition worsens, patients with 2nd and 3rd degree AV node block usually have a pacemaker implanted, since drug therapy is considered unreliable for severe symptoms.
Video: AV block and its degree on the ECG (atriventricular block)
Accelerated conduction between the atria and ventricles
The opposite of AV block is accelerated conduction between the atria and ventricles. This phenomenon is often determined against the background of Wolff-Parkinson-White syndrome. With this cardiac arrhythmia, one or more additional conduction pathways are usually identified, connecting the ventricles and atria to bypass the AV node. Accelerated transmission is usually manifested by a significant increase in pulse, and tachycardia, that is, rapid heartbeat, can also be detected.
In most cases, tachycardia can be regulated by the patient himself. For example, the heartbeat and rhythm stop slightly when you hold in air while exhaling. In addition, the doctor usually prescribes appropriate drugs like ajmaline to patients with tachycardia. In contrast to the slow transmission of excitation of the sinus node, surgical implantation of a pacemaker with accelerated conduction and tachycardia is not performed in most cases.
Atrioventricular nodal re-entry tachycardia
It may occur suddenly and be accompanied by an increase in normal heart contractions between pathological ones. Symptoms can last from a few minutes to several days, and some patients report no symptoms at all.
Reentry tachycardia becomes a problem when it occurs frequently and continues for a long time, especially in the presence of other cardiac damage.
The main signs of the disease are:
- Fluttering in the chest
- Rapid heartbeat
- Irregular breathing
- Dizziness
- Sweating
- Heaviness in the neck
- Fainting or pre-fainting
The most common types of re-entry tachycardia:
- Atrioventricular nodal reentry tachycardia (AVNRT). It occurs in men and women of any age, although it is more common in young women.
- Atrioventricular reciprocating tachycardia (AVRT) . It is the second most common type of re-entry tachycardia. Most often diagnosed in young people.
In the treatment of clinically significant pathology, conservative treatment is initially used. It is very important to take any antiarrhythmic medications exactly as prescribed by your doctor to minimize complications. If medications do not help, catheter ablation is used. During this procedure, the doctor guides one or more catheters through the blood vessels to the heart. Electrodes at the tips of the catheter can apply heat, extremely cold temperatures, or radiofrequency energy to tissue. This allows you to damage a small area of the myocardium and create an electrical block along the path that was causing the arrhythmia.
Sometimes treatment for reentrant tachycardia involves the use of a small implanted device called a pacemaker, which generates electrical impulses that stimulate the heart to beat at a normal rhythm. The pacemaker is placed under the skin near the collarbone during minor surgery. An insulated wire is guided from the device to the heart, where it is permanently attached.
Cystic tumor of the atrioventricular node
Primary cardiac tumors are rare diseases, defined with an incidence of 0.0017% to 0.03% of the total.
Cystic tumor of the atrioventricular (AV) node, also known as AV node mesothelioma, is a benign congenital tumor that is located in the triangle of Koch in the AV nodal region of the interatrial septum of the heart.
The AV nodal region is formed during embryonic fusion, when disrupted, the tissue transforms into a similar tumor. Studies have shown that 10% of people with AV node cystic tumor also have defects in midline development along the central axis of the vertical body (1,9), suggesting a genetic defect associated with migration of embryological tissues and unfavorable heredity. It has been suggested that, unlike a true neoplasm, it is most likely the result of dilatation of cystic spaces rather than cellular replication. In addition, there are no mitoses in this tumor
Because pacemaker implantation does not prevent sudden death in patients with this tumor, surgery is most often performed. There are various options for excision of the lesion, however, due to the rarity of AV node cystic tumors coupled with the difficulty of diagnosing the lesion, surgical resection techniques and therapeutic concepts are not fully standardized. For example, it remains controversial whether the lesion should be completely or partially removed from the base of the interatrial septum.
The prognosis for a cystic tumor of the AV node is favorable with early diagnosis followed by prompt and complete surgical removal of the pathological formation. Cases of sudden cardiac death have shown that this tumor is associated with fatal cardiac dysrhythmia and partial/complete heart block. Thus, despite the fact that the tumor is benign, most patients receive a definitive diagnosis after autopsy. Additionally, it is worth pointing out that tumor size does not appear to be associated with symptoms of lethal arrhythmia or sudden death.
Where is
Today we will look in more detail at one of its components - the sinoatrial node. It's just a scary name.
It is also called the sinoatrial, sinus, and Keyes-Fleck nodes. The sinoatrial node is located in the right atrium, into which the superior vena cava drains. This explains why we previously looked at the structure of the organ.
The sinoatrial node of the heart is a node that is a collection of muscle tissue. The length of such a knot is usually from 1 to 20 mm, and the width is from 3 to 5 mm. The structure of the sinoatrial node includes two types of cells: those that excite electrical impulses for the heart to work, and those that are responsible for conducting the resulting stimuli from the node to the atria.
The outer shell of these cells (membrane) is characterized by high permeability to sodium ions. The presence of sodium ions leads to the occurrence of certain actions in cells that are nearby, this is the so-called excitation wave. Shocks of excitation pass through the heart muscles and provoke their contraction.
The main function of the sinus node is the excitation of electrical impulses. The impulses generated in the node lead to excitation and contraction of the heart. During normal operation this is 60-80 pulses/min.
In many respects, the sinoatrial node is often called the pacemaker of the heart, since a wave of excitation originates in it, which, in turn, provokes the next one.
The contraction propagates along the walls of the atrium at a speed of 1 m/s. This information makes it possible to understand how the node works and where its location is.
RIGHT AND LEFT BAND BAND
The bundle of His in the lower part, called the bifurcation, is divided into two legs - right and left, which run subendocardially or intracardially along the corresponding side of the interventricular septum. The right crus is a long, thin, well-segmented fascicle consisting of many fibers with little or no proximal branching. In the distal part, the right bundle branch leaves the interventricular septum and reaches the anterior papillary muscle of the right ventricle, where it branches and anastomoses with the fibers of the Purkinje network.
Despite intensified morphological studies carried out in recent years, the structure of the left bundle branch remains unclear. There are two main schemes for the structure of the left bundle branch. According to the first scheme (Rosenbaum et al.), the left leg is, from the very beginning, divided into two branches - anterior and posterior. The anterior branch, which is relatively longer and thinner, reaches the base of the anterior papillary muscle and branches in the anterosuperior part of the left ventricle. The posterior branch is relatively short and thick and reaches the base of the posterior papillary muscle of the left ventricle. Thus, the intraventricular conduction system is represented by three pathways, named by Rosenbaum et al. fascicles - the right leg, the anterior branch and the posterior branch of the left bundle branch. Many electrophysiological studies support the idea of a three-bundle (trifascicular) intraventricular conduction system.
According to the second scheme (James et al.), it is believed that, unlike the right leg, the left one does not represent a separate bundle. The left leg at the very beginning, moving away from the His bundle, is divided into many fibers varying in number and thickness, which fan-shapedly branch subendocardially along the left side of the interventricular septum. Two of the many branches form more separate bundles - one located anteriorly in the direction of the anterior muscle, and the other posteriorly in the direction of the posterior papillary muscle.
Both the left and right bundle branches, like the internodal tracts of the atria, are composed of two types of cells - Purkinje cells and cells very similar to the cells of the contractile myocardium. Most of the right and anterior two-thirds of the left leg are supplied by the septal branches of the left anterior descending artery. The posterior third of the left leg is fed by the septal branches of the posterior descending artery. There are many transseptal anastomoses between the septal branches of the anterior descending coronary artery and the branches of the posterior descending coronary artery (James). The fibers of the vagus nerve reach both branches of the His bundle, but there are no ganglia of this nerve in the ventricular pathways.
Conduction system of the heart
The sinoatrial node (in Latin, nódus sinuatriális) is of great importance in the life of the body. Is it really as important as we say it is? The answer is simple, because the heart is a pump for our body, which pumps blood through the veins and arteries. This pump works only due to contractions in the organ. This is possible thanks to the conduction system of the heart.
Integral and very important components of this system are two components: the Kisa-Fleck node and the Aschoff-Tavara node.
Description of the atrioventricular node
The definition of “atrioventricular node” comes from the Latin: atrium - entrance, ventriculus - small belly. Synonyms: AV node (AV node), Aschoff-Tawar node, atrioventricular node.
In 1906, Sunao Tawara (1873-1952), a young Japanese anatomist working under Ludwig Aschoff in Marburg, Germany, published “A System of Impulse Transmission in the Mammalian Heart,” which described his three-year histological search. Tawara discovered a “complex nodal” (atrioventricular (AV) node) site at the proximal end of the divergence of the conducting fibers. He concluded that this was the beginning of an electrical conduction system that extended from the AV node through the His bundle, divided into right and left branches and ending in Purkinje fibers. Tawara was the first to realize that Purkinje fibers contain tissue that rapidly delivers impulses to the apex of the ventricle so that their compression extends from the apex of the heart to its base.
The atrioventricular node, or AV node, is a secondary center of the cardiac conduction system (second-order node) involved in the complex regulation of heart rate.
- Anatomy
The AV node is a muscular structure in Koch's triangle located in the right atrium near the atrial septum. At the macroscopic level it is difficult to distinguish. Located at the junction with the ventricles and regulates the transmission of impulses through the non-conducting cardiac skeleton to the lower chambers of the heart. The node is located at the top of the His bundle. Probably controlled by the sympathetic and parasympathetic systems, which are involved in the complex regulation of heart rate. It is usually supplied with blood from the atrioventricular nodal branch, which arises from the right coronary artery.
Thus, the atrioventricular node is the only electrical connection between the atria and the underlying cardiac chambers.
- Histology
The atrioventricular node consists of specific cardiac cells (cardiomyocytes), which are partially associated with the connective tissue of the cardiac skeleton. Unlike the working muscles of the heart, nodal cells are partially devoid of myofibrils and mitochondria.
- Physiology
The AV node is a secondary stimulation center for the heart. Typically, it receives the depolarization propagated through the working muscles of the atria and redirects them into the ventricles after a second delay. The time period for this transition is called atrioventricular conduction time (AV time), corresponding to the PQ interval on the ECG. Delayed excitation in the AV node is necessary to ensure coordinated and orderly contraction of the atria and ventricles. Atrial systole occurs slightly earlier than ventricular systole, which is necessary for complete filling of the lower parts of the heart.
Additionally, the AV node acts as a frequency filter. Under physiological conditions, it does not conduct signals above a certain frequency due to the refractory period of depolarized cardiac muscle cells. As a result, even with atrial flutter, when the heart rate of the atria increases to 300 beats/min and above, much fewer signals reach the ventricles, so they contract within acceptable limits.
- Pathophysiology
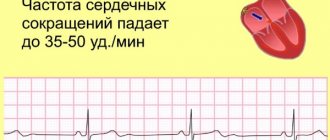
In the event of sinus node failure, the AV node can take over as the primary rhythm generator and control the heart rate from 40 to 60/min.
Excessive time lag of impulse conduction through the AV node or conduction failure can lead to AV block, which is divided into three stages of clinical severity. Sometimes accelerated transmission of electrical impulses is detected, then tachycardia and rapid pulse are noted, mainly present in the context of Wolff-Parkinson-White syndrome.
History of the origin of terms
The history of the origin of terms begins in the 19th century. The beginning of the 20th century is famous for its morphological studies of the heart, which have entered science and history. In 1806, S. Tavara discovered the atrioventricular node. He was named after the scientist. A. Kis and M. Fleck studied this issue; they accurately described the sinus node. They soon proved that this node is the main, one might say, irreplaceable generator of cardiac impulses.
It was also important that if the sinoatrial node loses its functions, the atrioventricular node automatically becomes the rhythm generator. Thus, these nodes complement each other in case of dysfunction of one of them.
INTERNODE PATHWAYS
Electrophysiological and anatomical studies in the last decade have proven the presence of three specialized pathways in the atria connecting the sinus node with the atrioventricular node: the anterior, middle and posterior internodal tracts (James, Takayasu, Merideth and Titus). These pathways are formed by Purkinje cells and cells very similar to the cells of the contractile atrial myocardium, nerve cells and ganglia of the vagus nerve (James).
The anterior internodal tract is divided into two branches - the first of them goes to the left atrium and is called the Bachmann bundle, and the second goes down and anteriorly along the interatrial septum and reaches the upper part of the atrioventricular node.
The middle internodal tract , known as Wenckebach's bundle, starts from the sinus node, passes behind the superior vena cava, descends down the posterior part of the interatrial septum and, anastomosing with the fibers of the anterior internodal tract, reaches the atrioventricular node.
The posterior internodal tract , called the bundle of Thorel, arises from the sinus node, passes downward and posteriorly, passes directly above the coronary sinus and reaches the posterior part of the atrioventricular node. Thorel's bundle is the longest of all three internodal paths.
All three internodal tracts anastomose with each other near the upper part of the atrioventricular node and communicate with it. In some cases, fibers depart from the anastomosis of the internodal tracts that bypass the atrioventricular node and immediately reach its lower part, or reach the place where it passes into the initial part of the His bundle.
Problems and pathologies
All organs of the body can be subject to the development of various pathologies. No one is immune from this. The heart is one of the organs that suffers most often. And of course, there are problems in the functioning of the nodes of the conduction system of the heart. You should be very careful about these disorders, as they can disrupt the functioning of the conduction system of the heart, which will lead to negative consequences. These problems lead to:
- Partial blockade. In this case, the impulse is carried out slowly.
- Complete blockade, when there is no impulse at all.
Such blockades can occur in different parts of the entire system. For example, it could be a sinus block - an area of disturbances and deviations in this particular node, an atrioventricular block - directly at the site of this node, etc. That is, the place where the blockage occurs is considered the name.
We already know that if the sinoatrial node does not work well, this entails dysfunction of the remaining components of the heart. Therefore, it is worth keeping all organs in order and protecting them as much as possible.
Even if a person leads a completely correct lifestyle, follows all recommendations, regulates work and rest time, and avoids stressful situations, he will not be able to avoid congenital blockages. They, as a rule, do not affect a person’s life and do not cause any discomfort.
Diagnosis of pathologies of the atrioventricular node
To diagnose AV node pathology, the doctor takes into account symptoms, medical history, and performs a physical examination. He may also ask about the presence of risk factors that often provoke the development of the disease. This could be another heart pathology or a problem with the thyroid gland. If necessary, tests are performed to examine the heart. Most often used:
- Electrocardiogram (ECG) . During an ECG, sensors (electrodes) that will detect the electrical activity of the heart are attached to the chest and sometimes to the limbs. An ECG measures the timing and duration of each electrical phase of the heartbeat.
- Holter monitoring . This is a portable ECG device that can be worn for a day or more to record heart activity during a person's daily activities.
- Event monitoring . For sporadic episodes of the disease, you need to keep a portable ECG device within reach so that if an attack occurs, you can attach it to your body and press the button on the recording device. This will allow your doctor to check your heart rhythm during an episode of arrhythmia.
- EchoCG . During this non-invasive test, a hand-held device (transducer) is placed on the chest. Through the use of sound waves, images are created from which the size, structure and movements of the heart are studied.
- Implantable recorder . The device detects abnormal heart rhythms, for which it is implanted under the skin in the chest area.
If the doctor does not detect signs of arrhythmia during these tests, other diagnostic methods may be used:
- Stress test . In some people, the abnormal rhythm is caused or worsened by stress or exercise. During the stress test, it is suggested that you exercise on a treadmill or stationary bicycle until your heart activity is normal. If doctors have assessed the risk of arrhythmia due to coronary artery disease, but the patient is having difficulty exercising, then a medication that stimulates the heart in a way that is similar to exercise may be used.
- Tilt table test. The doctor may recommend this test if the patient has had a history of fainting. Heart rate and blood pressure are measured while the person lies on a table. The table then tilts as if he were standing up. The doctor observes how the heart and nervous system react to changes in body position.
- Electrophysiological testing and mapping . In this test, the doctor threads thin tubes (catheters) through blood vessels to various places in the heart. Located in the heart chambers, electrodes can map the propagation of electrical impulses along the conduction system of the heart.
If necessary, the cardiologist can use electrodes to stimulate the heart to beat at a pace that causes or stops the arrhythmia. This allows you to determine the location of arrhythmic activity and what causes it.
Video: Cardiac conduction system (CCS)
4.75 avg. rating ( 93 % score) - 4 votes - ratings
Causes of diseases
The causes of heart disease can vary. Sometimes we may not even know that we are a carrier of any pathology. There are the following causes of pathology:
- acquired or congenital heart defects;
- surgical consequences, injuries;
- complications after illness;
- nervous system disorder;
- diseases of the respiratory system;
- thyroid diseases, diabetes mellitus, anemia;
- side effects from medications;
- alcohol and smoking;
- blockades that occur for no apparent reason.
People have the opportunity to solve such problems with medication and surgery.
Drug treatment involves taking vitamins and medications, following a diet (increasing the portion of fresh vegetables and fruits, avoiding too fatty and sweet foods). Surgery is used when drug treatment does not work. For example, a person often loses consciousness or the disease becomes malignant. In such cases, it is possible to install a pacemaker. After which such people should be under the constant supervision of specialists.
Disease Prevention
Nowadays, every person has some kind of health problem. These can be acquired diseases or congenital. Unfortunately, not every person will be able to afford regular treatment or wellness activities. But this does not mean that you need to resign yourself to health problems. Experts recommend following some rules that are effective and necessary in order to prevent disruption in the functioning of these organs. With their help, you can not only maintain your health level, reduce the risk of new ones, but also alleviate the form of existing diseases. These rules include:
- correct daily routine;
- balanced diet;
- rejection of bad habits;
- avoidance of stressful situations;
- timely contact with specialists.
It will not be difficult to follow such rules, but the result will not be long in coming. The most important thing is to follow the systematic implementation and learn to enjoy them.
This is how we learned where the sinoatrial node is located, what it is responsible for, and how to maintain stable heart function for many years. Take care of yourself, don't get sick! And most importantly, monitor your health.