Causes of fatty hepatosis
There are three main reasons for the development of hepatic steatosis:
- Obesity. If the body mass index exceeds 30, the likelihood of dystrophy is about 40%.
- Drinking alcoholic beverages. Moreover, hepatosis can occur even in people who drink a little, but every day. There is a direct relationship between the duration of alcohol consumption and the severity of liver dystrophy and, as a consequence, the risk of developing cirrhosis.
- Long-term use of medications with hepatotoxic effects.
Less commonly, hepatosis develops against the background of diseases that occur with metabolic disorders; this category includes hyperlipidemia, hypercholesterolemia, diabetes mellitus, thyrotoxicosis, myxedema, Itsenko-Cushing syndrome, malignant neoplasms, chronic diseases of the gastrointestinal tract, in which the absorption process is disrupted, etc. .
Liver dystrophy can be caused not only by obesity, but also by poor nutrition - overeating, abuse of fatty foods and foods containing hydrogenated fats and simple carbohydrates.
The disease is sometimes diagnosed in people who have a deficiency of enzymes involved in lipid metabolism (hereditary disease).
Most often, more than one factor leads to the development of steatosis. In most cases, there is a multifactorial factor, for example, the consumption of alcohol by a person who is eating poorly or taking toxic medications.
Fatty degeneration
Diabetes
2835 10 September
IMPORTANT!
The information in this section cannot be used for self-diagnosis and self-treatment.
In case of pain or other exacerbation of the disease, diagnostic tests should be prescribed only by the attending physician. To make a diagnosis and properly prescribe treatment, you should contact your doctor. Fatty degeneration: causes, symptoms, diagnosis and treatment methods.
Definition
Fatty degeneration, or lipodystrophy, is a group of rare disorders that are characterized by complete or partial loss of subcutaneous fat, as well as its abnormal distribution, in the absence of a previous fasting or catabolic state. These diseases are accompanied by various metabolic disorders: insulin resistance, specific diabetes mellitus (lipoatrophic diabetes), fatty hepatosis, steatohepatitis, lipid metabolism disorders, arterial hypertension.
Fatty degenerations are quite rare conditions; according to various sources, their incidence ranges from 1 to 60 cases per 1 million population.
Causes of fatty degeneration
Fatty degenerations are divided into congenital and acquired. Congenital lipodystrophies are always hereditary and associated with genetic mutations that lead to metabolic disorders in adipose tissue, resulting in its atrophy.
The mechanism of development of acquired generalized lipodystrophy is unknown; the disease is assumed to be related to genetic mutations and autoimmune processes.
Genetic mutations are also suspected in the occurrence of acquired partial lipodystrophies. Today, the most common type of lipodystrophy is a special variant of acquired partial dystrophy - lipodystrophy, which develops as a result of highly active antiretroviral therapy in HIV-infected patients. In addition, there are local lipodystrophies, which are usually associated with injections of drugs, for example, insulin.
Classification of the disease
Fatty degenerations are divided according to the degree of fat loss into generalized, when subcutaneous fatty tissue is absent over most of the body, and partial, or segmental, when adipose tissue atrophies in certain areas of the body.
Hereditary and acquired lipodystrophies are divided into 4 types:
- congenital generalized lipodystrophy (CHL, Berardinelli-Seyp syndrome) with 4 types depending on the gene in which the mutation occurred;
- acquired generalized lipodystrophies (PGL, Lawrence syndrome);
- familial partial lipodystrophy (FPL, Dunnigan-Cobberling syndrome) with 3 types;
- acquired partial lipodystrophy (PPL, Barraquer-Simons syndrome).
Separately, there are fatty degenerations that develop as a result of other genetic syndromes and those associated with drug injections.
Symptoms of fatty degeneration
With congenital generalized lipodystrophy, immediately after birth or in the first year of life, the child develops a complete absence of subcutaneous fat. Lipoatrophy can occur on the trunk, limbs, and face. In severe cases of the disease, there is a significant risk of intrauterine growth retardation. Due to the lack of fatty tissue, the patient experiences pseudohypertrophy of skeletal muscles, as a result of which the patient has an “athletic” appearance (usually observed in children over 10 years of age). Patients with generalized lipodystrophy are tall (ahead of bone age), they may have an enlarged lower jaw, hands and feet, there is an enlargement of the clitoris in women and external genitalia in men, children have a very high appetite - they are “insatiable.” Due to the difficulty in digesting fats, the level of lipids (triglycerides, cholesterol) in the blood increases and the load on the organs involved in their metabolism increases. There is an abnormal accumulation of fat in the liver, kidneys, myocardium, and skeletal muscles, which disrupts their functions.
This type of lipodystrophy is characterized by severe fatty hepatosis, leading to liver enlargement, steatohepatitis, liver cirrhosis and liver failure.
Since metabolism is a balanced system, when lipid metabolism is disturbed, both protein and carbohydrate metabolism suffer. Disorders of carbohydrate metabolism lead to insulin resistance from the first years of life and to the development of type 2 diabetes mellitus by the age of 15-20 years. Such patients experience hyperpigmentation of the groin area, neck, armpits, weight loss, increased thirst, and excessive urination. Some forms of congenital generalized lipodystrophy are accompanied by damage not only to adipocytes (adipose tissue cells), but also to skeletal muscle cells and myocardium (heart muscle), which can lead to hypertrophic cardiomyopathy, heart failure and subsequently to an unfavorable outcome.
In addition, with this type of lipodystrophy, psychomotor retardation, intellectual impairment, hirsutism (excessive hair growth in women according to the male pattern - in the armpits, on the pubis, above the upper lip) or hypertrichosis (excessive hair growth in all areas of the body and head, not associated with the secretion of sex hormones). Due to the lack of subcutaneous fat, the veins of the upper and lower extremities bulge - this is called phlebomegaly. The characteristic appearance of the patient is a thin face against the backdrop of a developed figure, noticeable saphenous veins, increased size of the feet and hands, areas of hyperpigmentation (acanthosis nigricans) in the area of skin folds.
With acquired generalized lipodystrophy, a child is born with a normal amount of subcutaneous fatty tissue, and its degradation begins in childhood or adolescence and occurs gradually. Large areas of the body are affected, especially the face and extremities, including the palms and soles. In approximately a quarter of cases, patients with PGL are first diagnosed with panniculitis (inflammation of subcutaneous fat tissue), which manifests itself as local lipodystrophies. There are also PGL associated with autoimmune diseases (~25%) and idiopathic (~50%).
Familial partial lipodystrophies appear in childhood or adolescence. A progressive loss of adipose tissue begins in the chest, anterior abdominal wall and limbs with its redistribution to other areas - the face, neck and inside the abdominal cavity. This redistribution of subcutaneous fat may resemble Cushing's syndrome or create a false impression of an “athletic” physique in women. In men, the redistribution of adipose tissue and the expression of skeletal muscles are often perceived as a normal physique. Metabolic disorders develop after puberty and are more severe in women.
SPF is characterized by insulin resistance, a significant increase in the concentration of free fatty acids and triglycerides in the blood, accumulation of fat in skeletal muscle cells and hepatocytes, and impaired leptin secretion.
Patients have a high risk of developing diabetes mellitus and insulin resistance, dyslipidemia, mainly due to increased triglyceride levels, pancreatitis, liver steatosis, hyperpigmentation in skin folds (this symptom is less pronounced than with VHL), arterial hypertension. In rare cases, myopathies and cardiomyopathies may develop, as well as hirsutism, menstrual irregularities and polycystic ovary syndrome, however, in most patients, reproductive function remains intact.
Acquired partial lipodystrophy is characterized by a progressive loss of subcutaneous fat in the upper body - in the face, neck, chest, upper extremities, and epigastric region.
This process can begin at any age, lasts from several months to several years and moves from top to bottom from the head to the feet, but, as a rule, does not affect the lower limbs. On the contrary, some patients may develop excess accumulation of fatty tissue in the lower abdomen, buttocks and thighs. Metabolic disorders are less common than in other types of fatty degeneration, but PPL is associated with the development of chronic kidney disease.
Diagnosis of fatty degeneration
When collecting complaints and anamnesis, the doctor pays attention to the patient’s appearance, and also studies the family history of the disease to identify the nature of its inheritance.
From laboratory examinations the patient is given:
- general blood analysis;
Classification
Based on etiology, hepatosis is divided into non-alcoholic fatty liver disease and alcoholic steatosis. The first type of disease is diagnosed in only 7–10% of cases.
Hepatosis occurs:
- primary - caused by metabolic disorders, for example, obesity or hyperlipidemia;
- secondary – due to the impact on the body of external negative factors, which subsequently lead to metabolic disorders, for example, fasting, long-term use of corticosteroids, intestinal resection.
Doctors also take into account the characteristics of fat deposition, according to which hepatosis is divided into:
- diffuse;
- zonal;
- focal disseminated;
- pronounced disseminated.
Symptoms of fatty liver disease
There are no specific signs of fatty liver hepatosis, even when there are already significant morphological changes. This is the insidiousness of the disease and lies a serious danger.
At the initial stage, the following nonspecific symptoms of fatty hepatosis may occur:
- general fatigue, asthenia, decreased ability to work;
- heaviness in the abdomen, stool instability, discomfort in the right hypochondrium, nausea, flatulence, sometimes vomiting;
- weight gain;
- causeless increase in body temperature for a long period of time;
- slight enlargement of the liver;
- skin itching.
As the disease progresses, icteric staining of the mucous membranes and skin is possible. Blood pressure often decreases and fainting occurs. There is a tendency to hemorrhages (increased bleeding).
There are 3 degrees of fatty hepatosis depending on the lesion:
- up to 33% – I degree;
- 33–66% – II degree;
- more than 66% – III degree.
Diabetes
Diabetes mellitus leads in mortality from diseases of the circulatory system among other endocrine diseases.
With diabetes mellitus, various lesions of the cardiovascular system develop:
- changes in the blood vessels of the heart - diabetic macroangiopathy;
- arterial hypertension (due to diabetic kidney damage, metabolic syndrome - depending on the type of diabetes);
- diabetic cardiomyopathy with rhythm disturbances and circulatory failure;
- IHD, sometimes with painless angina;
- increased levels of cholesterol and triglycerides in the blood;
- increased risk of ventricular fibrillation, myocardial infarction, and cerebrovascular accidents.
Treatment:
- compensation of carbohydrate metabolism (insulin therapy, hypoglycemic drugs);
- antihypertensive drugs, antiplatelet agents;
- lipid-lowering drugs (statins).
Diagnostics
Diagnosis of the disease is difficult. Firstly, steatosis has no specific symptoms. Secondly, biochemical tests do not show significant changes. Sometimes the activity of serum transaminases increases, but this indicator does not change in all patients with steatosis. In this regard, differential diagnosis with hepatitis, biliary tract obstruction, primary hemochromatosis, and hepatocerebral dystrophy is of primary importance.
The doctor makes the final diagnosis based on a comprehensive examination and a series of tests, including ultrasound and biopsy.
To find out the cause of fatty hepatosis, the level of insulin in the blood, serum glucose concentration, hormonal status, antibodies to cytomegalovirus and hepatitis viruses, markers of autoimmune hepatitis, etc. are determined.
Treatment of fatty hepatosis
Treatment of fatty hepatosis is usually complex, including diet therapy, drug therapy and physical therapy.
Diet plays an important and sometimes paramount role in the treatment of steatosis. Sometimes, to cure the first stage, it is enough to follow a diet. Thanks to a significant limitation of fat consumption, healthy cells, and there are more than 66% of them, independently remove the fat present in the liver. But even in the later stages, nutritional correction is a prerequisite. It is recommended to steam food, eat more greens, vegetables and low-fat dairy products, eggs, cereals, and vegetarian dishes.
The cause of its occurrence directly affects how fatty hepatosis is treated.
Weight loss is a necessary condition for obese patients. As a rule, this helps to get rid of insulin resistance, which leads to normalization of carbohydrate and lipid metabolism. But there is one important nuance here - you should not lose weight too quickly (up to 600 g per week is allowed), otherwise there is a risk of progression of fatty hepatosis.
For alcoholic fatty degeneration, successful treatment is only possible with complete abstinence from alcohol. Patients are recommended to consult a narcologist.
Lipotropic drugs for fatty hepatosis are prescribed to accelerate the removal of fat from the liver. This category includes drugs that normalize cholesterol and lipid metabolism, promote fat oxidation and its mobilization from the liver: lipoic acid, essential phospholipids, folic acid, B vitamins.
To prevent the destruction of cell membranes and stimulate the regeneration of hepatocytes, hepatoprotective drugs are prescribed for fatty liver hepatosis: betaine, taurine, ursodeoxycholic acid, glutargin, phosphatidylcholine,
Tablets containing ursodeoxycholic acid often prescribed for fatty hepatosis: Livodexa, Grinterol, Urdoxa, Ursodez, Ursoliv, Ursofalk, Exchol, Ekurochol.
Thiazolidinediones and biguanides are used to eliminate insulin resistance.
The utilization of fatty acids is improved by physical exercise, so it is recommended for all patients with this disease.
Thyrotoxicosis
Thyroid hormones (triiodothyronine, thyroxine) stimulate metabolism; their excess leads to an increase in the need for oxygen and energy. The heart muscle is especially sensitive to this and begins to suffer first: myocardial dystrophy develops, as a result - specific cardiomyopathy (“thyrotoxic heart”). Thyroid hormones also have a “stimulating” effect on the heart: they increase heart rate and cardiac output.
The following symptoms may develop:
- feeling of palpitations, rapid pulse even at rest, severe fatigue;
- increased blood pressure, especially systolic (“upper” pressure), usually stable, without crises;
- there is often a significant spread between the values of systolic and diastolic pressure;
- when listening to heart sounds, the doctor can identify characteristic noises, and ultrasound examination of the heart often reveals prolapse (sagging, protrusion) of the mitral valve;
- most often there is a so-called sinus tachycardia;
- if the patient initially had a cardiac pathology, against the background of thyrotoxicosis it worsens: attacks of angina pectoris, atrial fibrillation, resistant to drug therapy (in the elderly this is sometimes the only symptom of thyrotoxicosis).
Over time, the walls of the heart thicken, its cavities expand, the heart muscle is partially replaced by connective tissue, fibrosis forms, and the contractility of the heart is impaired, which can lead to heart failure and atrial fibrillation.
Treatment:
- medicinal – thyreostatics, beta blockers, cardiac glycosides, diuretics, antiplatelet agents, etc.;
- radioiodine therapy;
- Surgical intervention is resorted to in severe cases, with low effectiveness of conservative treatment - the so-called subtotal resection of the thyroid gland is performed - i.e. removing most of it. Hypothyroidism
With decreased thyroid function, heart rate, cardiac output, and blood pressure, on the contrary, decrease. The lipid composition of the blood changes, there is an increased cholesterol content, widespread atherosclerosis, especially of the heart vessels. A specific cardiomyopathy is formed - “hypothyroid” or “myxedematous heart”.
The following symptoms may appear:
- rare weak pulse;
- pain in the heart area;
- systolic pressure is usually low, while diastolic pressure may remain normal;
- sometimes it is possible to develop concomitant hypertension;
- general swelling;
- weakness, lethargy, sleep apnea;
- X-ray examination reveals an increase in the size of the heart.
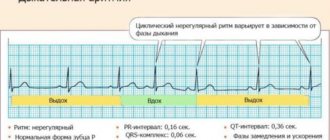
The most common type of arrhythmia in hypothyroidism is sinus bradycardia.
The contractile function of the heart suffers, and there is a risk of developing heart failure. Mucous fluid accumulates in the muscle wall and in the heart sac, mucinous edema develops, which also impedes the blood supply to the heart, all this can lead to the appearance of foci of ischemia and an increased risk of heart attack.
Treatment:
- The main treatment is thyroid hormone replacement therapy;
- With concomitant arterial hypertension - antihypertensive drugs, diuretics;
- There are also surgical innovative methods - for example, transplantation of donor thyroid cells.
Fatty hepatosis of pregnant women
Separately, there is hepatic steatosis, which occurs without a significant cause in women bearing a child. Acute fatty hepatosis of pregnancy is diagnosed in one out of 13,000 women. 20–25% of cases end in death, according to foreign authors, and up to 60%, according to domestic sources.
The disease progresses quickly, over 2–3 weeks. Occurs mainly in late pregnancy - 32–36 weeks. The exact cause of this pathology has not yet been established.
Symptoms that may indicate acute fatty hepatosis in pregnant women: excessive vomiting, severe nervous disorders, general weakness, drowsiness.
The only treatment method is emergency delivery. Within 5 weeks after birth, the disease regresses.
Prevention
Preventive measures include:
- proper nutrition, in particular limiting fatty, spicy, fried and smoked foods;
- moderation in the consumption of alcoholic beverages;
- taking medications correctly;
- regular physical activity.
Fat accumulation is often caused by excess weight due to a sedentary lifestyle. Scientists have proven that if you eat only fast food for 4 weeks, this disease will almost certainly occur. Student volunteers took part in the experiment. Moreover, the first signs appeared after 1 week of such nutrition. Therefore, nutrition and weight control are of great importance.
For prevention, hepatoprotectors should be used, especially during periods of increased load on the liver, for example, with prolonged alcohol consumption, antibiotic treatment, and following a diet aimed at weight loss.
Symptoms
Each form of muscular dystrophy has its own specific clinical picture, but there are also a number of common symptoms characteristic of this group of diseases:
- gradual decrease in muscle fiber tone;
- absence of pain syndrome;
- maintaining sensitivity of the affected areas;
- change in gait;
- frequent falls due to weakness of the leg muscles;
- change in muscle size;
- constant fatigue;
- gradual atrophy of skeletal muscles;
- loss of acquired physical skills in children.
Frequently asked questions about fatty liver disease
Which doctor should I contact?
A hepatologist specializes in liver diseases.
How to determine fatty hepatosis?
Unfortunately, the disease has no specific symptoms. A comprehensive examination allows you to identify deviations.
Can hepatic steatosis be cured?
With proper and timely therapy, changes in the liver are reversible. The main thing is to strictly follow all the doctor’s instructions, stick to your diet, and give up alcohol and “harmful” foods.