How to decipher test results?
A general idea of the number, size and shape of the constituent elements of blood (erythrocytes, platelets, lymphocytes, leukocytes) is given by a clinical blood test. Decoding its results can tell a doctor a lot about the condition of his patient’s body. For each indicator there is a range of reference (normal) values. These norms depend on gender and age. Thus, blood test standards in adults and children can differ significantly. As a rule, modern laboratories indicate reference values in the results form that the client receives. However, deviations from the norm of certain indicators do not yet indicate the presence of pathological conditions. The results of blood tests can be influenced by severe physical activity on the eve of blood sampling, and in women, also by the phase of the menstrual cycle. It is known, for example, that the day before the start of menstruation, the level of leukocytes can rise almost 2 times, so the normal values will differ from the standard ones. Therefore, it is better to contact a specialist for interpretation.
But what to do when it is important to get at least a general idea of the state of your body before going to the doctor? In this case, you can use the “online analysis interpretation” service, where you can enter the indicators of your analysis online and receive a preliminary conclusion. It is important to do this on the website of the exact laboratory where the tests were taken, because different units of measurement for blood parameters may be used. If the tests were taken in a laboratory whose website does not have such a service, then at your service is a calculator for converting units of measurement and a table for deciphering the main indicators of a general blood test. It contains blood test indicators that are considered reference values for middle-aged men and women. The interpretation of blood tests in children varies depending on age. The younger the child, the more his normal blood counts will differ from those of an adult. Thus, the number of leukocytes in the first days of a child’s life can be 2-3 times higher than the concentration of these cells in the blood of an adult. And this will not be a deviation from the norm.
Complexes with this research
Advanced female anti-aging diagnostics Advanced monitoring of basic blood parameters in women aged 40+ 19,540 R Composition
Anti-aging diagnostics in postmenopause Monitoring of age-related changes during the postmenopausal period 7,440 R Composition
Male check-up No. 1 39 studies for annual preventive examination RUR 10,930 Composition
IN OTHER COMPLEXES
- Preventative check-up 6,530 RUR
- Biochemistry of blood. 19 indicators 3,420 RUR
- Advanced male anti-aging diagnostics RUR 22,840
- Women's check-up No. 1 11,530 RUR
- Advanced anti-aging diagnostics in postmenopause RUR 19,860
General blood analysis. Table of reference values
| Index | Patient gender | Norm |
| Hemoglobin | Men Women | 130-170 g/l 120-150 g/l |
| Red blood cells | Men Women | 4.0-5.0 1012/l 3.5-4.7 1012/l |
| Leukocytes | — | 4.0-9.0×109/l |
| Hematocrit (the ratio of the volume of plasma and cellular elements of blood) | Men Women | 42-50% 38-47% |
| Average red blood cell volume | — | 86-98 µm3 |
| Leukocyte formula | — | Neutrophils:
Monocytes: 3-11% Eosinophils: 0.5-5% Basophils: 0-1% |
| Platelet count | — | 180-320·109/l |
| Erythrocyte sedimentation rate (ESR) | Men Women | 3 - 10 mm/h 5 - 15 mm/h |
When do you need to take a potassium (K+), sodium (Na+), chloride test?
- Diseases of the kidneys and cardiovascular system, including arterial hypertension and arrhythmia.
- Profuse vomiting, nausea, diarrhea, constipation.
- Pharmacotherapy with diuretics.
- Abuse of laxatives and adsorbents.
- Increased consumption of salt (sodium chloride).
- Cushing's syndrome.
- High doses, long-term use of glucocorticosteroids.
- Inadequate diet, increased consumption of coffee, alcohol, sugar.
- Muscle weakness, rhabdomyolysis and paralysis.
- Chemotherapy.
- Diabetes.
- Adrenal dysfunction.
- Formation of kidney stones.
- Osteoporosis.
Decoding the biochemical blood test
A biochemical blood test in adults shows whether the most important internal organs are functioning correctly: liver, pancreas, kidneys, cardiovascular system, muscles. So creatinine speaks about the work of the kidneys, as well as the state of the muscular system, albumin and bilirubin - about the work of the liver, the level of glucose, cholesterol and triglycerides in the blood - about metabolism. In addition, a biochemical blood test can reveal a lack of essential microelements in the body: you will receive their reference values along with the test results. The normal results of blood tests indicate the coordinated functioning of the main organs; deviation from the norms is a reason for further diagnosis and consultation with a doctor.
Different results in different laboratories. Where is the truth?
Why is the IgG antibody value of 2 considered positive in one laboratory, and negative in another? How do you understand that immunity has been formed? And who to believe?
Today we talk about all the nuances of laboratory diagnostics of the immune response to coronavirus.
What are reference intervals?
The results of some studies are given to patients in the format of “yes” and “no”; such studies are called qualitative. There are quantitative and semi-quantitative tests. Together with them, the laboratory issues reference interval values.
The reference interval is the range of indicator values that is average for a healthy person in the population.
Why do they differ from one laboratory to another?
Manufacturers of equipment and test systems set their reference values. And in different laboratories the same analysis can be carried out using different test systems.
For example: IgG values for the test system are considered negative:
- Mindray (China) <10;
- Abbott (USA)<1;
that is, you will be considered not to have been in contact with the infection if the results show 5 units for the Chinese test system and 0 for the American one.
That is why the doctor who interprets the result should always rely on the reference interval.
Why else might antibody tests show incorrect results?
Antibody tests are based on the principle of antigen-antibody reaction. Where the antibody is an immunoglobulin and the antigen is the protein on the surface of the virus.
And different test systems detect different antigen proteins.
For example, the Abbot test system detects IgG antibodies to the nucleocapsid (N) protein. And the Mindray and Vector-Best test system detects IgG to the spike (S) protein.
In total, there are 4 types of proteins that test systems can identify:
- S1 (spike protein domain)
- S2 (spike protein domain)
- RBD (a fragment of the S1 protein; neutralizing antibodies are synthesized against it)
- N (nucleocapsid)
First of all, you need to understand the purpose for which the IgG test is taken, and based on this, choose the test:
- To find out whether post-vaccination immunity has formed: you need to take an IgG test for the spike (S) protein. The Sputnik V vaccine contains a section of the virus genome that encodes the S protein. And if you take an IgG test for the nucleocapsid (N) protein, it will show that immunity has not been formed. But in fact, the body will be familiar with the infection, simply antibodies will be synthesized to another of its proteins.
- Has there been contact with infection and has immunity been formed? In this case, it is better to get tested for antibodies to two proteins, N and S, in order to be more likely to “catch” antibodies to both viral proteins.
For personal advice on selecting the right test, you can contact the hotline. Doctors at the Doctor Q service help you select tests, interpret their results, and choose the right strategy for further diagnosis for free.
LABquest - Your correct diagnostic path!
Primary diagnosis of anemia
A comprehensive study taking into account the quantitative and qualitative composition of cells, as well as biochemical blood parameters, which allows us to identify signs of iron deficiency anemia.
The research results are provided with a free doctor’s commentary.
English synonyms
Iron deficiency anemia screening.
Research method
Colorimetric photometric method, flow cytometry, SLS (sodium lauryl sulfate) method, conductometric method, immunoturbidimetry.
Units
μmol/l (micromoles per liter), *10^9/l (10 in st. 9/l), *10^12/l (10 in st. 12/l), g/l (grams per liter), % (percent), fl (femtoliter), pg (picogram).
What biomaterial can be used for research?
Venous blood.
How to properly prepare for research?
- Eliminate alcohol from your diet 24 hours before the test.
- Do not eat for 12 hours before the test.
- Do not take medications for 24 hours before the test (as agreed with your doctor).
- Avoid physical and emotional stress 30 minutes before the test.
- Do not smoke for 30 minutes before the test.
General information about the study
Anemia is a pathological condition characterized by a decrease in the number of red blood cells and/or hemoglobin in the blood. The causes of anemia are varied and can be closely related to chronic somatic diseases (kidney and liver pathologies, autoimmune, infectious and inflammatory diseases, diabetes, tumors), acute and chronic blood loss, hereditary diseases and malnutrition, lack of vitamins and microelements. They occur when there is insufficient production of red blood cells in the bone marrow (for example, with deficiency of iron, vitamins B12 and B6, bone marrow depletion) or premature and excessive destruction of red blood cells in the bloodstream (for example, with hemolysis).
The most common form of anemia, iron deficiency, is detected in 80-90% of patients who have a reduced number of red blood cells and/or hemoglobin in the blood.
Iron deficiency develops gradually. Initially, a negative iron balance is created, in which the body's needs for it and its losses exceed the amount it receives from food. This may be due to blood loss, pregnancy, breastfeeding, growth spurts during puberty, malabsorption of micronutrients in the gastrointestinal tract, or insufficient intake of foods containing iron, as with vegetarianism.
Normally, iron is absorbed in the small intestine, but in some chronic diseases of the stomach and intestines, malabsorption syndrome occurs with impaired absorption of nutrients and microelements from food. In the blood, iron is transported by the protein transferrin to sites of use or accumulation. With iron deficiency, the amount of free transferrin in the blood increases, and the level of serum iron decreases. Hemoglobin synthesis in the bone marrow occurs less actively, and iron deficiency anemia develops with clinical manifestations of anemia. In a general blood test, small pale colored red blood cells are detected, MHC (average hemoglobin content in an erythrocyte), MCV (average erythrocyte volume), MCHC (average hemoglobin concentration in an erythrocyte), and hemoglobin level and hematocrit decrease. Without treatment, the amount of hemoglobin decreases more and more, the shape of red blood cells changes, and the intensity of cell division in the bone marrow decreases. Due to a decrease in the amount of hemoglobin and red blood cells, the transport of oxygen and carbon dioxide in the tissues is disrupted, symptoms of anemia appear: pale skin, headache, memory impairment, drowsiness, spots before the eyes, dizziness, fainting, rapid heartbeat, decreased blood pressure, pain in the area heart, muscle weakness.
In addition to well-being, negative changes occur in appearance: dry skin (as a result, early wrinkles), brittle nails, hair loss.
Children susceptible to anemia are more likely than healthy peers to suffer from colds.
In addition, with iron deficiency, the patient may experience a disturbance of taste and smell: there is a desire to eat chalk, clay, raw cereals and inhale the smells of acetone, gasoline, and turpentine.
Often people do not pay attention to the main signs of anemia - constant fatigue, paleness, dry skin - considering them an insufficient reason to see a doctor. Of course, such symptoms do not always indicate a disease; it cannot be diagnosed only by their presence. Moreover, you should not start taking iron-containing medications on your own - this can lead to serious complications.
It is important to know what exactly causes anemia. For example, in older people it often results from internal bleeding due to a tumor in the gastrointestinal tract. There is a type of anemia associated with poor absorption of vitamin B12. But in order to identify it, you first need to make sure that there is enough iron in the body and that the red blood cells are saturated with it.
At the same time, simply donating blood for hemoglobin is not enough to fully diagnose anemia. For example, in smokers, the level of hemoglobin and red blood cells is often normal: carbon monoxide contained in cigarettes, combining with hemoglobin, forms the substance carboxyhemoglobin, this form of hemoglobin does not have the ability to carry oxygen, and to compensate for oxygen starvation, the level of hemoglobin increases. It turns out that a comprehensive analysis is needed, reflecting the true reserves of this microelement in the body: determination of the levels of serum iron, transferrin, reticulocytes, general blood test, leukocyte formula.
In addition, it is important that timely diagnosis of anemia makes it possible to identify diseases of which it is the first symptom: some malignant tumors, chronic inflammatory processes, helminthic infestations, etc.
What is the research used for?
- For the diagnosis of iron deficiency anemia.
- For differential diagnosis of anemia.
- For the evaluation of patients at high risk of developing anemia.
- To evaluate the effectiveness of treatment for iron deficiency anemia.
When is the study scheduled?
- For symptoms of iron deficiency in the body (pallor and/or yellowness of the skin, general weakness, fatigue, drowsiness, dizziness, tinnitus, flashing spots before the eyes, fainting, atrophy of the tongue mucosa, changes in the structure of the nails, abnormal taste preferences).
- When the number of red blood cells and/or hemoglobin decreases according to a clinical blood test.
- In the presence of risk factors for the development of anemia (pregnancy, breastfeeding, menstrual irregularities, malnutrition, vegetarianism, diseases of the stomach and intestines with impaired absorption of nutrients, chronic stress).
- When examining children during periods of intensive growth.
- When examining patients with asthenia of unknown origin and severe fatigue.
- When monitoring the effectiveness of the use of drugs containing iron.
What do the results mean?
Reference values
- Serum iron
| Floor | Age | Reference values |
| Female | Less than 24 days | 17.9 - 44.8 µmol/l |
| 24 days – 1 year | 7.2 - 17.9 µmol/l | |
| 1-14 years | 9 - 21.5 µmol/l | |
| More than 14 years | 10.7 - 32.2 µmol/l | |
| Male | Less than 24 days | 17.9 - 44.8 µmol/l |
| 24 days – 1 year | 7.2 - 17.9 µmol/l | |
| 1-14 years | 9 - 21.5 µmol/l | |
| More than 14 years | 12.5 - 32.2 µmol/l |
- Leukocyte formula
- Leukocytes
| Age | Reference values |
| Less than 1 year | 6 - 17.5 *10^9/l |
| 1-2 years | 6 - 17 *10^9/l |
| 2-4 years | 5.5 - 15.5 *10^9/l |
| 4-6 years | 5 - 14.5 *10^9/l |
| 6-10 years | 4.5 - 13.5 *10^9/l |
| 10-16 years | 4.5 - 13 *10^9/l |
| More than 16 years | 4 - 10 *10^9/l |
- Neutrophils
| Age | Reference values |
| Less than 1 year | 1.5 - 8.5 *10^9/l |
| 1-2 years | 1.5 - 8.5 *10^9/l |
| 2-4 years | 1.5 - 8.5 *10^9/l |
| 4-6 years | 1.5 - 8 *10^9/l |
| 6-8 years | 1.5 - 8 *10^9/l |
| 8-10 years | 1.8 - 8 *10^9/l |
| 10-16 years | 1.8 - 8 *10^9/l |
| More than 16 years | 1.8 - 7.7 *10^9/l |
- Neutrophils, %
| Age | Reference values |
| Less than 1 year | 16 — 45 % |
| 1-2 years | 28 — 48 % |
| 2-4 years | 32 — 55 % |
| 4-6 years | 32 — 58 % |
| 6-8 years | 38 — 60 % |
| 8-10 years | 41 — 60 % |
| 10-16 years | 43 — 60 % |
| More than 16 years | 47 — 72 % |
- Complete blood count (without leukocyte formula and ESR)
- Leukocytes
| Age | Reference values |
| Less than 1 year | 6 - 17.5 *10^9/l |
| 1-2 years | 6.6 - 11.2 *10^9/l |
| 2-4 years | 5.5 - 15.5 *10^9/l |
| 4-6 years | 5 - 14.5 *10^9/l |
| 6-10 years | 4.5 - 13.5 *10^9/l |
| 10-16 years | 4.5 - 13 *10^9/l |
| More than 16 years | 4 - 10 *10^9/l |
- Red blood cells
| Floor | Age | Reference values |
| Less than 1 year | 4.1 - 5.3 *10^12/l | |
| 1-5 years | 4 - 4.4 *10^12/l | |
| 5-6 years | 4.1 - 4.5 *10^12/l | |
| 6-7 years | 4 - 4.4 *10^12/l | |
| 7-8 years | 4.2 - 4.6 *10^12/l | |
| 8-9 years | 4.1 - 4.5 *10^12/l | |
| 9-14 years | 4.2 - 4.6 *10^12/l | |
| 14-15 years old | 4.4 - 4.8 *10^12/l | |
| Female | 15-19 years old | 3.5 - 5 *10^12/l |
| More than 19 years | 3.5 - 5.2 *10^12/l | |
| Male | 15-19 years old | 3.9 - 5.6 *10^12/l |
| More than 19 years | 4.2 - 5.3 *10^12/l |
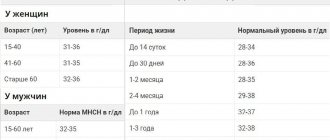
- Hemoglobin
| Age | Reference values |
| Less than 2 weeks | 134 - 198 g/l |
| 2 weeks – 2 months | 124 - 166 g/l |
| 2-12 months | 110 - 131 g/l |
| 1-2 years | 110 - 132 g/l |
| 2-3 years | 111 – 133 g/l |
| 3-4 years | 112 – 134 g/l |
| 4-5 years | 114 - 134 g/l |
| 5-6 years | 113 - 135 g/l |
| 6-7 years | 115 - 135 g/l |
| 7-8 years | 116 - 138 g/l |
| 8-9 years | 115 - 137 g/l |
| 9-10 years | 118 - 138 g/l |
| 10-11 years | 114 - 140 g/l |
| 11-12 years old | 118 - 142 g/l |
| 12-13 years old | 117 - 143 g/l |
| 13-14 years old | 121 - 145 g/l |
| 14-15 years old | 120 – 144 g/l |
| 15-16 years old | 130 – 168 g/l |
| 16-17 years old | 130 – 168 g/l |
| 17-18 years old | 120 – 148 g/l |
| Over 18 years old | 120 – 156 g/l |
- Hematocrit
| Floor | Age | Reference values |
| Less than 1 year | 33 — 41 % | |
| 1-3 years | 32 — 40 % | |
| 3-6 years | 32 — 42 % | |
| 6-9 years | 33 — 41 % | |
| 9-12 years | 34 — 43 % | |
| Female | 12-15 years | 34 — 44 % |
| 15-18 years old | 34 — 44 % | |
| 18-45 years old | 35 — 45 % | |
| 45-65 years | 35 — 47 % | |
| More than 65 years | 35 — 47 % | |
| Male | 12-15 years | 35 — 45 % |
| 15-18 years old | 37 — 48 % | |
| 18-45 years old | 39 — 49 % | |
| 45-65 years | 39 — 50 % | |
| More than 65 years | 39 — 50 % |
- Mean erythrocyte volume (MCV)
| Floor | Age | Reference values |
| Less than 1 year | 71 – 112 fl | |
| 1-5 years | 73 – 85 fl | |
| 5-10 years | 75 – 87 fl | |
| 10-12 years | 76 – 94 fl | |
| Female | 12-15 years | 73 – 95 fl |
| 15-18 years old | 78 – 98 fl | |
| 18-45 years old | 81 – 100 fl | |
| 45-65 years | 81 – 101 fl | |
| More than 65 years | 81 – 102 fl | |
| Male | 12-15 years | 77 – 94 fl |
| 15-18 years old | 79 – 95 fl | |
| 18-45 years old | 80 – 99 fl | |
| 45-65 years | 81 – 101 fl | |
| More than 65 years | 81 – 102 fl |
- Average hemoglobin content in erythrocytes (MCH)
| Age | Reference values |
| Less than 1 year | 31 - 37 pg |
| 1-3 years | 24 - 33 pg |
| 3-12 years | 25 - 33 pg |
| 13-19 years old | 26 - 32 pg |
| More than 19 years | 27 - 31 pg |
- Mean erythrocyte hemoglobin concentration (MCHC)
| Age | Reference values |
| Less than 1 year | 290 – 370 g/l |
| 1-3 years | 280 – 380 g/l |
| 3-12 years | 280 – 360 g/l |
| 13-19 years old | 330 - 340 g/l |
| More than 19 years | 300 – 380 g/l |
- Platelets
| Floor | Age | Reference values |
| Less than 1 year | 214 - 362 *10^9/l | |
| 1-2 years | 208 - 352 *10^9/l | |
| 2-3 years | 209 - 351 *10^9/l | |
| 3-4 years | 196 - 344 *10^9/l | |
| 4-5 years | 208 - 332 *10^9/l | |
| 5-6 years | 220 - 360 *10^9/l | |
| 6-7 years | 205 - 355 *10^9/l | |
| 7-8 years | 205 - 375 *10^9/l | |
| 9-10 years | 177 - 343 *10^9/l | |
| 10-11 years | 211 - 349 *10^9/l | |
| 11-12 years old | 198 - 342 *10^9/l | |
| 12-13 years old | 202 - 338 *10^9/l | |
| 13-14 years old | 192 - 328 *10^9/l | |
| 14-15 years old | 198 - 342 *10^9/l | |
| 15-18 years old | 165 - 396 *10^9/l | |
| 18-45 years old | 159 - 376 *10^9/l | |
| Male | 45-65 years | 156 - 300 *10^9/l |
| Female | 45-65 years | 156 - 351 *10^9/l |
| More than 65 years | 139 - 363 *10^9/l |
- Mean platelet volume (MPV)
| Age | Reference values |
| Less than 10 years | 8.3 - 10.9 fl |
| 10 – 18 years | 8.6 - 12.1 fl |
| 18 – 45 years old | 8.5 - 12.8 fl |
| 45 – 65 years | 8.6 - 12 fl |
| 45 – 65 years | 9 - 12.9 fl |
| More than 65 years | 8.8 - 12.4 fl |
- Reticulocytes
- Reticulocytes, % (RET%)
| Floor | Age | Reference values |
| Female | Less than 2 weeks | 0,15 — 1,5 % |
| 2 weeks – 1 month | 0,45 — 1,4 % | |
| 1-2 months | 0,45 — 2,1 % | |
| 2-6 months | 0,25 — 0,9 % | |
| 6 months – 2 years | 0,2 — 1 % | |
| 2-6 years | 0,2 — 0,7 % | |
| 6-12 years | 0,2 — 1,3 % | |
| 12-18 years old | 0,12 — 2,05 % | |
| Over 18 years old | 0,59 — 2,07 % | |
| Male | Less than 2 weeks | 0,15 — 1,5 % |
| 2 weeks – 1 month | 0,45 — 1,4 % | |
| 1-2 months | 0,45 — 2,1 % | |
| 2-6 months | 0,25 — 0,9 % | |
| 6 months – 2 years | 0,2 — 1 % | |
| 2-6 years | 0,2 — 0,7 % | |
| 6-12 years | 0,2 — 1,3 % | |
| 12-18 years old | 0,24 — 1,7 % | |
| Over 18 years old | 0,67 — 1,92 % |
- Reticulocytes (absolute count, RET#)
| Floor | Reference values |
| Female | 17 - 63.8 *109/l |
| Male | 23 - 70 *109/l |
- Immature reticulocyte fraction (IRF)
| Floor | Reference values |
| Female | 3 — 15,9 % |
| Male | 2,3 — 13,4 % |
- Transferrin
| Age | Reference values |
| Less than 11 years old | 2.03 - 3 g/l |
| More than 11 years | 2 - 3.6 g/l |
Serum iron
Reasons for the increase:
- anemia (aplastic, hemolytic, pernicious), thalassemia;
- polycythemia;
- acute hepatitis, liver damage;
- hemochromatosis;
- hemosiderosis;
- nephritis;
- lead poisoning;
- excessive intake of iron supplements.
Reasons for the decline:
- chronic inflammation;
- Iron-deficiency anemia;
- blood loss;
- burns;
- malignant neoplasms;
- rheumatoid arthritis;
- myocardial infarction;
- nephrosis;
- malabsorption;
- pregnancy;
- uremia.
General blood analysis
1) Red blood cell count
Reasons for the increase:
- erythremia;
- chronic heart and pulmonary failure;
- stress, physical activity, staying at high altitudes;
- Itsenko-Cushing syndrome.
Reasons for the decline:
- anemia of various origins;
- acute and chronic leukemia;
- lymphomas;
- myelodysplastic syndrome;
- radiation sickness;
- renal failure;
- hypothyroidism;
- taking cytostatics.
2) Hemoglobin
Reasons for the increase:
- erythrocytosis;
- polycythemia;
- dehydration;
- burns;
- Cushing's syndrome;
- kidney cysts;
- liver cancer;
- heart failure;
- chronic lung diseases with respiratory failure.
Reasons for the decline:
- anemia of various origins;
- blood loss;
- myelodysplastic syndrome;
- Addison's disease;
- overhydration;
- acute and chronic leukemia, lymphoma;
- multiple myeloma;
- cirrhosis;
- chronic infection;
- hypothyroidism;
- kidney disease;
- pregnancy;
- autoimmune diseases;
- deficiency of vitamins B6, B12.
3) Mean erythrocyte volume (MCV)
Causes of increased (macrocytosis):
- megaloblastic anemia;
- myelodysplastic syndrome;
- liver diseases;
- pregnancy;
- hypothyroidism;
- alcoholism;
- treatment with estrogens, barbiturates.
Reasons for decrease (microcytosis):
- anemia (microspherocetary, iron deficiency, sideroblastic, thalassemia);
- anemia in chronic diseases;
- hypohydration;
- aluminum intoxication.
4) Dispersion of red blood cell distribution by volume (RDW)
Reasons for the increase (anisocytosis):
- anemia (hemolytic, iron deficiency, megaloblastic);
- osteomyelofibrosis.
5) Average hemoglobin content in erythrocytes (MCH)
Causes of increase (hyperchromia):
- megaloblastic anemia;
- cirrhosis of the liver;
- neonatal period.
Reasons for decrease (hypochromia):
- Iron-deficiency anemia;
- thalassemia;
- sideroblastic anemia.
6) Mean erythrocyte hemoglobin concentration (MCHC)
Reasons for the increase:
- megaloblastic anemia;
- microspherocytosis;
- prolonged hypohydration;
- neonatal period.
Reasons for the decrease (absolute hypochromia):
- Iron-deficiency anemia;
- thalassemia;
- sideroblastic anemia;
- hydremia.
7) Hematocrit usually decreases with anemia of various etiologies.
 The number of platelets can be increased in iron deficiency anemia and hemolytic crisis, decreased in aplastic or megaloblastic anemia.
The number of platelets can be increased in iron deficiency anemia and hemolytic crisis, decreased in aplastic or megaloblastic anemia.
9) The number of leukocytes decreases with megaloblastic or aplastic anemia, severe forms of iron deficiency anemia.
Reticulocytes
Reasons for increase (hyperregeneration):
- anemia (hemolytic, acute post-hemorrhagic);
- effective treatment of anemia caused by deficiency of iron, folic acid, vitamins B12 and B6 (on the 6-10th day);
- recovery from the state of bone marrow hypoplasia after cytostatic therapy;
- splenectomy;
- malaria.
Reasons for decrease (hyporegeneration):
- anemia (hypo- or aplastic, megaloblastic);
- anemia of chronic disease;
- myelodysplastic syndrome;
- acute leukemia;
- radiation sickness;
- regeneration crisis in hemolytic anemia;
- kidney pathology;
- taking cytostatics.
Transferrin
Reasons for the increase:
- Iron-deficiency anemia;
- pregnancy;
- taking estrogen.
Reasons for the decline:
- acute inflammation;
- anemia in chronic diseases;
- hypoproteinemia (with chronic infections, chronic kidney diseases, liver diseases, neoplasms, burns and malnutrition);
- genetic defects;
- hemochromatosis;
- oversaturation of the body with iron.
What can influence the result?
- Transfusion of blood and its components.
- Use of intravenous radiopaque agents shortly before the examination.
- Hemodialysis.
- Alcoholic liver disease, acute and chronic inflammatory diseases, neoplasms.
- Taking medications containing iron.
- The use of certain hormonal drugs, as well as other drugs that affect certain test indicators.
Important Notes
- Iron deficiency anemia is often a complication of other diseases, so it is important to find out the primary cause of iron loss. Diagnosis must be comprehensive, taking into account clinical data and the results of additional instrumental methods.
- Incorrect diagnosis of the type of anemia leads to inadequate treatment and progression of the disease. In difficult diagnostic cases, bone marrow puncture and myelogram are recommended. Only a doctor can evaluate the results of the study and select therapy.
Also recommended
- Laboratory diagnosis of iron deficiency anemia
- Laboratory diagnosis of anemia
- Bilirubin and its fractions (total, direct and indirect)
- Laboratory examination of the kidneys
- General urine analysis with sediment microscopy
- Fecal occult blood test
- Erythrocyte sedimentation rate (ESR)
- C-reactive protein, quantitative (highly sensitive method)
- Total protein in whey
- Serum albumin
- Ferritin
- Iron binding capacity of serum
- Latent iron binding capacity of serum
- Vitamin B9 (folic acid)
- Vitamin B12 (cyanocobalamin)
- Erythropoietin
Who orders the study?
Therapist, pediatrician, general practitioner, obstetrician-gynecologist, hematologist.
Literature
- Harrison's Principles of Internal Medicine. 16th ed. NY: McGraw-Hill; 2005: 2607 p.
- Fischbach FT, Dunning MB A Manual of Laboratory and Diagnostic Tests, 8th Ed. Lippincott Williams & Wilkins, 2008: 1344 p.
- Wilson D. McGraw-Hill Manual of Laboratory and Diagnostic Tests 1st Ed. Normal, Illinois, 2007: 666 p.
- Internal medicine: Textbook in 3 volumes. T1/Ed. prof. E. N. Amosova. – K.: Medicine, 2008 – P. 907-938.
General definition
A blood test for hormones can reveal whether hormonal balance is disturbed. Today there is an increase in endocrine diseases caused by dysfunction of the endocrine glands. To prevent negative consequences by starting therapy in a timely manner, it is recommended to regularly check your hormonal levels. This can be done in our multidisciplinary medical. Highly qualified specialists who have the best diagnostic equipment at their disposal will help identify problems in the body’s functioning at the earliest stages.
Other factors influencing research results
Laboratories usually report your test results using reference values for your age and gender. Your doctor then interprets the results for you based on his personal knowledge of your health and the drug therapy you are using. It is necessary to take into account that the results of the study may be influenced by many additional factors: consumption of coffee, tobacco, alcohol, vitamins, natural and artificial dyes, etc.; features of your diet (for example, vegetarian or meat), stress or pregnancy. Even your posture when the biomaterial is taken from you can affect some of the results, as well as the physical activity preceding the test.
For example, albumin and calcium levels may increase when changing from a lying to an upright position.
Intense exercise can affect the activity of the enzymes creatine phosphokinase (CPK), aspartate aminotransferase (AST), and lactate dehydrogenase (LDH). Therefore, going to the gym the night before a test may lead to an increase in CPK. Additionally, testosterone, luteinizing hormone (LH) and platelet levels may be increased in people who have been actively involved in sports such as long-distance running for several months or years or weightlifting.
All these factors emphasize the importance of following the rules of preparation for analysis. It is also important to follow your doctor's instructions when preparing for tests. Following these simple rules will give you even greater confidence in the correctness and accuracy of the results obtained.
Detailed description of the study
Water-electrolyte balance is ensured by various molecular structures of cells, which, through regulatory mechanisms, are transformed into a single system with physiological processes in the human body.
In clinical practice, sodium balance disturbances may occur in the form of its deficiency or excess. The renal mechanism of sodium regulation is the most important factor in maintaining plasma concentrations. The release of sodium salts depends on factors such as aldosterone secretion, acid-base status and potassium concentration in the blood plasma. Sodium plays an important role in the regulation of osmotic pressure and water metabolism, when disturbed, symptoms such as thirst, dry mucous membranes, swelling of the skin are noted, and also has a significant effect on protein metabolism. Sodium metabolism is under the control of the thyroid gland, with hypofunction of which it is retained in the tissues.
Potassium is the main cation in the intracellular space. Potassium deficiency is one of the most common electrolyte disturbances in clinical practice. Potassium deficiency plays a key role in the occurrence of functional disorders of the cardiovascular and central nervous systems. Potassium has an irritating effect on mucous membranes, increases the tone of smooth muscles (intestines, uterus), which is why its compounds are used as laxatives.
The main and important role of chlorine is played in maintaining blood plasma volume, blood and osmotic pressure, as well as in maintaining the acidity of gastric juice. The main organ of deposition is the skin, in the cells of which a large amount of incoming chlorine accumulates. It is excreted from the body through the urinary system (up to 90%), in small quantities it is excreted through the pores of the skin with sweat and through the gastrointestinal tract (gastrointestinal tract).
The modern system of indicators for laboratory diagnostics of water-electrolyte metabolism disorders makes it possible to understand the nature and extent of these disorders and carry out their rational therapy.
How to evaluate test results that are outside the reference range?
There are several reasons why test results may fall outside the established reference range, even if you are completely healthy:
- When values fall outside the range, it is associated with the physiological characteristics of the human body. If your doctor advises you to take the same test several times, there is a certain chance that the result will be outside the reference range. For biological reasons, your results may vary from day to day. That is why the doctor may ask you to take the test again to then compare the results. In most cases, diagnostic conclusions are made not on the basis of single measurements, but on the dynamics of changes in results over time.
- Individual characteristics of the body can also affect your results. Reference values are usually calculated by experimental clinical studies of a large number of people in certain categories, then the data are averaged, taking into account the average standard deviations. This is just statistical data, not biological law. Therefore, it happens that in healthy people certain indicators that are the “norm” for them are not ultimately the “norm” for the majority of the population and do not fall within the range of generally accepted reference values.
As a rule, such cases imply only a slight deviation from the reference values.
However, readings outside the reference range may signal problems in the body and indicate the need for further testing. Your doctor will evaluate the test results, taking into account your medical history, physical condition and other relevant factors to determine whether something signifies serious deviation of your test result from the generally accepted reference values. He may order a repeat test or order additional tests. It is also important for the doctor to compare the results of current and previous tests, if we are talking about a situation where you took the same test, to find out what is the “norm” for you.
If you are aware of any special circumstances that could affect the test results, tell your doctor about them. One should not think that the doctor could have guessed about them on his own.
References
1. Chaltsev, B. D., Vasiliev, V. I., Palshina S. G. [etc.]. Clinical guidelines for the diagnosis and treatment of Schörgen's disease with anticentromere antibodies. Scientific and practical rheumatology, 2019. 2. Rheumatoid arthritis. Clinical recommendations. approved Ministry of Health of Russia, 2021. - URL: https://legalacts.ru/doc/klinicheskie-rekomendatsii-revmatoidnyi-artrit-utv-minzdravom-rossii/ (access date: 02/11/2021). 3. Croia, C, Bursi, R, Sutera, D, One year in review 2021: pathogenesis of rheumatoid arthritis. Clinical Experience in Rheumatology, 2021.