Forms of pancreatitis
Acute – characterized by acute girdling pain in the upper abdomen. Pain often appears after eating fatty foods or alcohol. Unpleasant sensations can be either barely noticeable or unbearable, radiating to the scapula or sternum. Nausea, vomiting, and stool disturbances are observed. Due to the obstructed flow of bile, the skin takes on a yellowish color.
Chronic - the main localization of pain is on the upper part of the abdominal wall with irradiation to the back, chest (left side), lower abdomen. Unpleasant sensations occur after eating heavy fatty foods, alcoholic drinks, and constant stress.
The development of chronic pancreatitis is characterized by nausea, loss of appetite, bloating, bowel dysfunction, and sometimes vomiting.
The chronic form of the pathology differs from the acute form by periods of remission and exacerbation. As the disease progresses, periods of exacerbation become more frequent; intestinal disorders, disturbances in normal digestion, and weight loss are possible.
Chronic pancreatitis often causes complications (stomach bleeding, cancer, cysts and abscesses, liver damage, diabetes mellitus, enterocolitis). That is why you need to take the disease seriously and, at the slightest suspicion of the development of inflammation, consult a doctor.
Pathogenesis of the disease
Inflammatory phenomena in the pancreas gradually lead to degenerative changes in its structure, tissue sclerosis and obliteration of the ductal system. This process usually occurs in waves. The exacerbation is replaced by remission, instead of the glandular tissue that produces enzymes, connective tissue appears. Gradually, enzymes become insufficient; first of all, the exocrine function of the pancreas (production of digestive enzymes) decreases, and then the endocrine function (decreased insulin production).
Symptoms of pancreatic enzymatic insufficiency appear when normal pancreatic tissue is damaged by 90%.
Triad of symptoms of chronic pancreatitis
- pancreatic calcification;
- diabetes;
- steatorrhea is characteristic of an advanced stage of the disease. Steatorrhea occurs when lipase production by the pancreas falls below 16% of its normal level.
Impaired processing and absorption of nutrients in chronic pancreatitis leads to poor absorption of proteins, fats and vitamins. As a result, exhaustion, asthenia, and metabolic disorders of bone tissue and the blood coagulation system may develop.
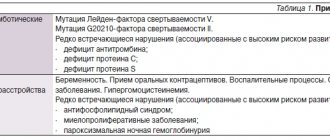
Reasons for the development of pancreatitis
The disease develops due to damage to pancreatic tissue. This happens for the following reasons:
- alcohol and tobacco abuse
- abdominal trauma, surgery
- uncontrolled and long-term use of medications: antibiotics, hormonal drugs, corticosteroids, some diuretics
- intoxication with food products, chemicals
- genetic predisposition
- improper diet with a predominance of spicy and fatty foods and long breaks between meals
14.06.2018
Author of the article: Gerlakh Alexander Alexandrovich, gastroenterologist of the highest category.
Chronic pancreatitis is characterized by a progressive irreversible decrease in the exocrine and endocrine function of the pancreas. There are many different classifications of chronic pancreatitis.
In the practical work of a general practitioner and gastroenterologist, the most acceptable and used is the clinical and morphological classification according to V.T. Ivashkin.
- I. According to morphological characteristics: interstitial edematous, parenchymatous, fibrinous sclerotic (indurative), hyperplastic (pseudotumorous), cystic.
- II. According to clinical manifestations: pain variant, hyposecretory, astheno-neuratic, latent, combined.
- III. According to the nature of the clinical course: rarely recurrent, often recurrent.
- IV.According to etiology: biliary-dependent, alcoholic, dysmetabolic (diabetes mellitus, hyperparathyroidism), infectious, drug-induced, idiopathic.
Based on this classification. Let us dwell on biliary-dependent pancreatitis. Recently, the number of patients with cholelithiasis has increased. As a result, there are more patients with biliary-dependent pancreatitis.
Etiology and pathogenesis . The cause-and-effect relationship between cholelithiasis (GSD) and pancreatitis is well known. Stones from the common bile duct, entering the ampulla of the papilla of Vater, can cause the development of acute pancreatitis. If the stone passes into the duodenum, the inflammatory phenomena in the pancreas subside quickly enough. When a calculus is strangulated in the ampulla of the major duodenal papilla, the signs of exacerbation of pancreatitis increase. In recent years, biliary sludge has been given an increasingly important role in the development of chronic pancreatitis [1]. As a result of destabilization of the physicochemical state of bile, precipitation of its main components occurs and the formation of biliary sludge (BS) in the gallbladder. An important factor contributing to the persistence of BS is dysfunction of the gallbladder and sphincter apparatus of the biliary tract. The constant passage of BS through the biliary tract leads to damage to the mucous membrane, mainly in the area of the sphincter of Oddi. Traumatization of the mucous membrane occurs by microlites, which make up the main part of the BS. As a result of this, secondary dysfunction of the sphincter of Oddi first develops, and subsequently stenotic papillitis forms. Functional and organic changes in the area of the major duodenal papilla disrupt bile outflow and contribute to the development of biliopancreatic reflux. It is bile refluxate that is the main pathogenetic factor in the occurrence of acute or exacerbation of chronic pancreatitis. In this regard, such pancreatitis is usually referred to as biliary pancreatitis (BP). Considering the close connection between BS and the development of acute pancreatitis, it is currently generally accepted that the diagnosis of idiopathic pancreatitis can be made only after excluding microlithiasis in the patient.
Clinic. The leading symptom in the clinical picture of PD is abdominal pain. They are usually localized in the epigastrium and radiate to the back. Pain is usually associated with overeating, eating spicy, fatty, fried foods, or occurs spontaneously at night. The cause of the development of pain syndrome is mixed. On the one hand, they are caused by the presence of biliary pathology and arise, as a rule, as a result of dysfunction of the sphincter apparatus of the biliary tract. On the other hand, they are associated with exocrine pancreatic insufficiency.
The main causes of abdominal pain in PD may be the following:
1. Inflammatory process in the pancreatic parenchyma (stretching of the capsule, compression of nerve endings).
2. Complications of chronic pancreatitis
intrapancreatic: duct obstruction; pseudocysts; pancreatic neuritis (scar changes in the area of intrapancreatic nerve endings).
extrapancreatic: stenosis of the intrapancreatic portion of the common bile duct with the development of biliary hypertension; stenosing papillitis; stenosis of the descending duodenum.
3. Exocrine insufficiency syndrome (flatulence with increased intraintestinal pressure, impaired motor function of the small and large intestine, excessive bacterial growth in the intestine).
4. Concomitant diseases of the digestive system (chronic gastritis, duodenitis, erosive and ulcerative lesions of the gastroduodenal region).
The causes of abdominal pain vary depending on the stage of the disease. In the acute period, the leading cause is the inflammatory process in the pancreatic parenchyma. Subsequently, as acute phenomena subside, various complications and exocrine pancreatic insufficiency take first place as the causes of pain. The mechanism of pain formation in chronic PD is due to the peculiarities of duodenal digestion. The nutrients supplied from the stomach to the duodenum are a mixture of long-chain polypeptides that stimulate pancreatic secretion to a greater extent than their monomers. It should be noted that the intestinal (duodenal) phase of pancreatic secretion is the main one, since it accounts for 70–80% of the volume of postprandial secretion. This phase of intestinal secretion is regulated by reflex and humoral mechanisms.
The most important is hormonal regulation through cholecystokinin-producing cells. Nutrients release cholecystokinin-pancreozymin from I-cells, the most important stimulator of pancreatic secretion of enzymes in its intestinal phase [3].
Various strictures and deformations of the ductal system, both from the pancreas and the terminal sections of the bile ducts, make it difficult for an adequate outflow of pancreatic juice at the height of digestion. In this regard, hypertension in the ductal system increases, which leads to the occurrence or intensification of pain. The main clinical symptoms of exocrine pancreatic insufficiency are: a feeling of heaviness in the epigastrium that occurs immediately after eating, belching, bloating, stool disorders (usually diarrhea, an increase in the mass of stool and a change in its color, a foul odor and a greasy appearance), weight loss. However, such a clear clinical picture is observed only in a small number of patients with severe disorders of pancreatic function (with exocrine deficiency of more than 90%) [4].
During the attack, moderate fever is possible. A pronounced clinical picture of acute PD develops when a calculus is strangulated in the ampulla of the major duodenal papilla with disruption of the outflow of bile and pancreatic secretions. In this situation, the clinical picture of obstructive jaundice with partial or complete disruption of bile outflow and pancreatic juice is added.
Diagnostics. Laboratory signs include moderate leukocytosis, changes in liver function tests (increased activity of aminotransferases, alkaline phosphatase, GGTP), as well as increased levels of serum amylase and lipase. It should be noted that changes in liver function tests in PD are more pronounced than in pancreatitis of alcoholic or other etiology. To diagnose exacerbation of biliary pancreatitis, it is important to study the levels of serum amylase and lipase. It should be taken into account that the level of amylase increase depends on the time of taking the material for research. Thus, the level of amylase increases already in the first hours of exacerbation of pancreatitis, reaches a maximum by the end of the first day, remaining at elevated levels for another 2–3 days, and by the 4th day it decreases to normal levels. At the same time, the dynamics of changes in the level of lipase differs from amylase. The level of lipase increases from the end of the 4th day, reaches a maximum on the 5th–6th day and remains at elevated levels for up to 12 days. Naturally, with complicated pancreatitis, the dynamics of amylase and lipase levels may differ significantly.
Methods by which pancreatic enzyme deficiency is detected can be divided into 2 groups.
1. Direct methods - based on determining the activity of pancreatic enzymes in various biological media - pancreatic juice, blood plasma, duodenal contents, feces, urine.
2. Indirect methods - based on assessing the digestive ability of its enzymes (scatological study with determination of the amount of neutral fat or the presence of slightly changed muscle fibers).
In practice, fecal diagnostic tests are most often used to detect exocrine pancreatic insufficiency:
- quantitative study of neutral fat in the volume of feces excreted within 72 hours. An increase in fat content of more than 6 g/day is a pathology;
- determination of pancreatic elastase-1 in feces. A level of less than 200 mcg of elastase in 1 g of feces indicates pancreatic insufficiency.
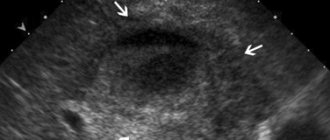
The main instrumental diagnostic method is ultrasound examination (US). Stones or various forms of biliary sludge are detected in the gallbladder and/or common bile duct (Fig. 2, 3, 4). If it is difficult to visualize the common bile or pancreatic duct using transabdominal ultrasonography, endoscopic ultrasound is used (Fig. 5). The common bile duct can be of normal size; its expansion occurs when a stone is pinched in the terminal section or ampulla of the major duodenal papilla. The Wirsung duct is of normal size or moderately dilated. It should be noted that the normal size of the common bile duct according to ultrasound is not a convincing sign of the absence of pathology in it. According to our data (Fig. 6), with a common bile duct width of up to 6 mm, accepted by most researchers as the norm, the frequency of detection of stones in the common bile duct with cholecystolithiasis is 20.6%, and with the gallbladder removed for cholelithiasis - 43.4%. Changes in the pancreatic parenchyma depend on the stage of the process. In the early stages, changes in the pancreas cannot be detected. Subsequently, the heterogeneity of the structure and the unevenness of its contours are revealed. During exacerbation of PD, ultrasound signs of edema of pancreatic tissue are detected. Dynamic cholescintigraphy (DCSG) is indicated to determine the patency of the bile ducts. The ability to trace the entire process of bile redistribution with analysis of its accumulation and evacuation into the duodenum is a valuable advantage of DHSG [6], especially in PD, when ERCP is associated with a high risk of exacerbation of the pathological process in the pancreas. At the same time, ERCP is the most common method for diagnosing pathology of both the biliary system and the pancreas. If necessary, papillotomy or papillosphincterotomy is simultaneously performed during the examination. Violation of the functional state of the pancreas, as mentioned above, is not always accompanied by changes in its parenchyma, therefore methods such as computed tomography, nuclear magnetic resonance and transabdominal ultrasound may be uninformative. An alternative method for diagnosing PD in these cases is EUS. Recently, in clinical practice, magnetic resonance cholangiopancreaticography has been increasingly used to diagnose PD, which allows simultaneous assessment of the condition of the bile and pancreatic ducts. Various criteria have been proposed for predicting the severity of pancreatitis. The most widely used system is based on the Renson criteria [5], which can also be applied to PD.
Treatment. Drug treatment of PD does not differ from the treatment of other forms of pancreatitis, however, it has its own characteristics associated with the pathogenesis of the disease and should primarily be aimed at eliminating the cause that caused the development of biliary pancreatitis. Fasting for 3-5 days is recommended. The volume of fluid taken should meet the body's needs (1.5–2.0 l). To suppress pancreatic secretion and create its maximum functional rest, ranitidine 150 mg 2 times, famotidine 20-40 mg 1-2 times a day, omeprazole 40 mg 1-2 times a day, sandostatin 0.1-0, 2 mg - 1-2 times/day s.c. Antacids are indicated - Maalox, Remagel, phosphalugel - 10-15 ml every 2-3 hours. According to indications - polyglucin (dextran) 400 ml/day, hemodez (pavidon) 300 ml/day, 10% albumin solution 100 ml/day, 5-10% glucose solution 500 ml/day - intravenously. For pain relief - baralgin 5 ml , papaverine 2 ml of a 2% solution 1–2 times a day, platiphylline 1–2 ml of a 0.2% solution 1–2 times a day, drotaverine 2–4 ml of a 2% solution 1–2 times a day and others. For severe and resistant pain - non-narcotic analgesics (tramadol 1 capsule (0.05 g) 2-3 times a day or 1-2 ampoules (0.05-0.1 g) slowly intravenously or intramuscularly). It should be noted that that myotropic antispasmodics used to relieve abdominal pain have a number of side effects that limit their use. Thus, the antispasmodic effect can simultaneously be accompanied by a decrease in motility of the stomach, duodenum, intestines and the secretion of saliva, gastric and intestinal juice (atropine, metacin, belladonna), a bronchodilator effect (papaverine, aminophylline), impaired atrioventricular conduction (papaverine), hypotension ( drotaverine, aminophylline), dizziness, sleep disturbance (halidor) and other disorders. These drugs are contraindicated for glaucoma, prostate adenoma (atropine, metacin, platifillin), organic diseases of the liver, kidneys (platifillin), hypotension (halidor, nitroglycerin, no-spa, aminophylline, platifillin). In this regard, to relieve abdominal pain in PD, the use of Duspatalin (mebeverine) 200 mg 2 times a day is indicated. Clinical experience of using the drug abroad is quite convincing and amounts to about 40 years. Duspatalin appeared on the Russian pharmaceutical market relatively recently and is used mainly for irritable bowel syndrome. Recent studies have shown that the antispasmodic effect of duspatalin is accompanied by relief of pain and dyspeptic disorders in cholelithiasis (Table 1).
Dynamics of clinical symptoms during 7–14 days of therapy with Duspatalin for cholelithiasis
| Symptoms | N | Treatment effectiveness, % | |
| in 7 days | in 14 days | ||
| Pain in the right hypochondrium | 20 | 70 | 85 |
| Bitterness in the mouth | 13 | 30 | 45 |
| Belching | 9 | 20,5 | 32 |
| Nausea | 15 | 14,6 | 20,5 |
As can be seen from table. 1 after 7 days of treatment with Duspatalin, pain in the right hypochondrium decreased in 14 of 20 patients with cholelithiasis (70%), and after 14 days completely disappeared in 17 (85%) patients and significantly decreased in duration and intensity in 3 patients ( 15%) [7].
Similar data were obtained with the use of Duspatalin in patients with postcholecystectomy syndrome [8]. This fact served as the basis for its use in PD. It should be noted that the antispasmodic effect of Duspatalin is higher compared to other known drugs and, for example, is 30 times higher than that of platyphylline. The drug is practically not absorbed into the general bloodstream and, therefore, has no side effects, which allows it to be used for a long time (one month or more).
Pancreatic enzyme inhibitors are used - contrical, gordox. When expanding the diet, enzyme preparations are prescribed - Creon, pancitrate, mezim, festal, pancreatin and others.
It should be noted that digestion is a normally quite stressful process. In healthy people, about 300–600 thousand IU of lipase are released during the digestion phase (within 6 hours), which corresponds to 87–171 Mezim tablets, 50–100 Festal tablets or 30–60 Creon 10,000 capsules).
This places serious demands on enzyme replacement therapy for exocrine pancreatic insufficiency, which can be formulated as follows:
- the active principle (pancreatin) must reach the site of application (duodenum) without being destroyed in the stomach and be active only in the intestine;
- the effect of the drug should develop with the beginning of food entering the duodenum.
- In this regard, the ideal enzyme preparation must meet the following requirements:
- have an optimal composition of enzymes in physiological proportions;
- be acid-resistant against gastric juice;
- mix evenly and quickly with food;
- simultaneously with food enter through the pylorus into the duodenum;
- have an optimal effect in the pH range 4–7;
- quickly and completely release enzymes in the duodenum;
- have no side effects.
Experimental studies have established that particles with a diameter of 1–1.5 mm are better mixed with food in the stomach and at the same time leave it. Thus, the effectiveness of an enzyme preparation is determined not so much by the content of enzymes in one tablet or capsule, but by its dosage form. When using tablet forms of enzyme preparations, only about 10% of the administered dose reaches the site of action in the duodenum, the remaining 90% of the drug is destroyed in the stomach. In this regard, to obtain the maximum effect, it is necessary to take a dose of the drug 10–20 times larger, since a significant part of the enzyme acts as ballast. If we analyze in accordance with the stated requirements the entire range of enzyme preparations used in practice for replacement therapy for exocrine insufficiency pancreas, it can be noted that only two of them - Creon and pancitrate - meet these conditions. However, they differ significantly in the number of particles (minimicrospheres, microtablets) in the capsule (Fig. 7). The largest number of them is contained in the capsule of Creon 10000 and Creon 25000. It is also important that the minimicrospheres are enclosed in a capsule, which is a container that quickly breaks down in an acidic gastric environment. A large number of microspheres are easily mixed in the stomach and simultaneously enter the duodenum with food. Thus, Creon, thanks to its special dosage form, creates the most optimal conditions for cavity digestion.
Number of particles per capsule in various enzyme preparations
| A drug | Lipase content | Number of particles per capsule | |
| Creon | 8 000 | 130–150 | |
| Creon | 10 000 | 10 000 | 285–303 |
| Creon | 25 000 | 25 000 | 488–501 |
| Pancitrate | 25 000 | 25 000 | 59–63 |
Comparative characteristics of enzyme preparations depending on the dosage form and the content of enzymes in them are shown in table. 2. As can be seen from the table, the dosage form of Creon is presented in the most optimal physiological ratio of enzymes, which makes it the drug of choice for the correction of exocrine pancreatic insufficiency.
Comparative characteristics of enzyme preparations
| A drug | Components | |||
| lipase | amylase | protease | other | |
| Mezim (tablets) | 3.5 thousand ed ph eur | 4.2 thousand ed ph eur | 250 edph eur | |
| Panzinorm (dragée) | 6.0 ed fip | 7.5 ed fip | 450 ed fip | chemotrypsin 1500 ed fip cholic acid 13.5 mg |
| Creon 10000 microspheres in gelatin. capsule | 10.0 thousand ed ph eur | 8.0 thousand ed ph eur | 600 edph eur | |
| Creon 25000 microspheres in gelatin. capsule | 25.0 thousand ed ph eur | 18.0 thousand ed ph eur | 1.0 thousand ed ph eur | |
| Pancitrate capsules containing microtablets | 10.0 thousand 25.0 thousand ed ph eur | 9.0 thousand 22.5 thousand ed ph eur | 500 ed ph eur 1250 ed ph eur | |
| Festal (dragée) | 6.0 thousand ed ph eur | 4.5 thousand ed ph eur | ox bile extract | |
Clinical experience suggests that, depending on the degree of exocrine pancreatic insufficiency and the composition of the diet, the effective daily dose of Creon 10,000 for PD can range from 4 to 15 capsules. In this case, the dose of the drug should not be determined by clinical criteria, but based on data from objective tests.
To prevent cholangitis and pancreatic abscesses, broad-spectrum antibiotics are used, with preference given to those that are excreted primarily in the bile, for example, Klacid (clarithromycin) 500 mg 2 times a day.
In the presence of biliary sludge, litholytic therapy with ursodeoxycholic acid (ursosan, ursofalk) or in combination with chenodeoxycholic acid is indicated. The dose of UDCA is selected depending on the patient’s weight (on average 10–15 mg/kg); the course of treatment usually does not exceed 3 months, but can be longer if necessary. For dysfunction of the sphincter of Oddi, other drugs are also used - hepabene 1-2 capsules 3 times a day for 2-4 weeks, Odeston 200-400 mg (1-2 tablets) 3 times a day for 2-3 weeks.
In the presence of biliary hypertension, choledocholithiasis, stenotic papillitis, depending on the indications, balloon dilatation or papillosphincterotomy with removal of stones from the common bile duct is used
Symptoms of pancreatitis
Manifestations of pathology vary depending on the form - acute or chronic pancreatitis. In acute pancreatitis the following are observed:
- The pain is intense, constant, the nature of the pain is described by patients as cutting, dull.
- High body temperature, high or low blood pressure - the patient’s well-being quickly deteriorates due to the rapid development of the inflammatory process.
- Pale or yellowish complexion.
- Nausea and vomiting - dry mouth and a white coating appear, attacks of vomiting do not bring relief. The most correct step at this moment is to fast; any food intake can only worsen the situation.
- Diarrhea or constipation - stool in acute pancreatitis is most often foamy, often with a foul odor, with particles of undigested food. On the contrary, there are constipation, bloating, and hardening of the abdominal muscles, which may be the very first signal of an acute attack of pancreatitis.
- Bloating – the stomach and intestines do not contract during an attack.
- Shortness of breath - appears due to loss of electrolytes during vomiting.
Chronic pancreatitis is characterized by the following symptoms:
- Abdominal pain - may be girdling or have a clear localization radiating to the back. Appears after eating.
- Intoxication of the body - general weakness, loss of appetite, tachycardia, increased body temperature, and decreased blood pressure appear.
- Endocrine disorders - ketoacidosis, diabetes mellitus, tendency to hypoglycemia. Bright red spots may also appear in the abdomen, back, and chest, which do not disappear with pressure.
With a long course of the disease, the patient gradually develops anemia, weight loss, dry skin, brittle hair and nails, symptoms of vitamin deficiency, and increased fatigue.
Lack of secretion
Exocrine insufficiency is a decrease in the production of pancreatic juice. It is manifested by digestive disorders with “fatty” stools - steatorrhea. The stool volume is larger than the standard 200 grams, mushy or watery, almost like diarrhea. The surface of the feces is shiny, such stool is called “greasy.” There is not enough pancreatic juice for the normal processing of dietary fats, they are not absorbed, and this causes a person to lose weight, although the appetite does not suffer from insufficiency. All this may be accompanied by nausea, flatulence, and a feeling of rapid satiety with a small portion of food.
A quarter of patients in the late stages of CP develop endocrine insufficiency—a decrease in insulin production. A normal amount of insulin may be produced, but the gland's production of the hormone glucagon is greatly reduced, which causes hyperglycemia, when blood sugar levels rise sharply with tremors, profuse sweats, and even loss of consciousness. Another variant of insulin inadequacy may develop - pancreatic diabetes. This type of diabetes progresses aggressively, like type 1 diabetes in children.
In a third of patients, during an exacerbation of CP, the level of bilirubin increases, since the enlarged head of the pancreas compresses the bile duct, blocking bile in the liver, and there may even be obstructive jaundice.
First aid for an attack of pancreatitis
To reduce pain, you can use a heating pad filled with cold water. It needs to be applied to the abdominal area, namely to the epigastric region (the area under the xiphoid process, corresponding to the projection of the stomach onto the anterior abdominal wall). This allows you to reduce the intensity of pain, slightly reduce swelling and inflammation.
The patient must comply with the hospital regime. This will reduce blood flow to the organ, and therefore reduce inflammation.
Eating is prohibited. The digestion process can cause more severe pain, nausea and vomiting. And the diet will reduce the production of enzymes that increase the inflammatory response and pain. You need to fast for 3 days. You can drink clean water without gases.
It is imperative to call a doctor for an examination, even if the patient is not exactly sure that this is an attack of acute pancreatitis. As we already know, this pathology can subside and then rapidly recur. At this time, you can take a painkiller to reduce discomfort.
Diagnosis of the disease at the private medical clinic “Medunion”
Diagnosing this disease is not difficult, since the first signs speak for themselves. However, in order to prescribe adequate treatment, it is necessary to determine the form of the disease. To do this, the doctor performs laparoscopy - a method that allows you to examine the abdominal cavity from the inside using a special instrument.
If acute pancreatitis is suspected, laboratory tests are performed:
- General blood analysis
- Blood chemistry
- Analysis of urine
- Stool analysis
- Ultrasound, MRI or radiography of the abdominal organs
- Computed tomography according to indications
In the chronic form, the same studies are carried out, but it is better to take tests during the period of exacerbation of the disease.
Our services
The administration of CELT JSC regularly updates the price list posted on the clinic’s website. However, in order to avoid possible misunderstandings, we ask you to clarify the cost of services by phone: +7
| Service name | Price in rubles |
| Ultrasound of the abdominal organs (liver, gall bladder, pancreas, spleen) | 3 800 |
| Pancreatocholangiography | 4 500 |
| MSCT of the abdominal cavity and retroperitoneal space of the abdomen | 6 000 |
All services
Make an appointment through the application or by calling +7 +7 We work every day:
- Monday—Friday: 8.00—20.00
- Saturday: 8.00–18.00
- Sunday is a day off
The nearest metro and MCC stations to the clinic:
- Highway of Enthusiasts or Perovo
- Partisan
- Enthusiast Highway
Driving directions
Treatment of acute pancreatitis
If acute pancreatitis is detected, the patient should be hospitalized immediately. Treatment should take place in a hospital setting, as this condition is very dangerous.
To relieve pain, antispasmodics are taken; in difficult cases, the contents of the stomach are pumped out to relieve the load on the gland.
In case of exacerbation of pancreatitis, patients require hospitalization with daily monitoring of blood parameters, water balance, leukocyte count, and enzyme levels in the blood serum during the first week. In the first 1–3 days, fasting and taking alkaline solutions every 2 hours are recommended.
During an exacerbation of chronic pancreatitis, the patient is shown therapy similar to the acute process. The patient must follow a diet throughout his life and take drugs from the group of antispasmodics and drugs that normalize the secretory function of the organ.
The most important thing in the chronic form of the disease is to maintain a diet that involves excluding fatty and fried foods from the diet. At the slightest violation of the regimen, the patient may experience discomfort and nausea. For intense pain, the doctor prescribes antispasmodics. Antisecretory therapy can be used for a short course.
Diagnostics
It is a very difficult matter, but when stones are visible in the projection of the pancreas during an X-ray of the abdominal cavity, this is considered sufficient to make a diagnosis. But ultrasound is not used to detect chronic pancreatitis because it is not informative; the gland is not visible at all.
CT helps to make a diagnosis and monitor changes in the pancreas, but MRI is much worse in quality.
Endosonography is the same sensitivity as CT - a combination of endoscopy and ultrasound, plus you can immediately take a puncture from the gland. If the instrumental examination is uncertain, functional tests can be performed that indirectly assess the working capabilities of the organ in the later stages, when secretory insufficiency has flourished, but their information content leaves much to be desired.
Diet for pancreatitis
For any form of the disease, the patient is prescribed a strict diet “Table No. 5p”, according to which it is forbidden to eat spicy and fried foods. All dishes are steamed, boiled or baked. Alcohol and smoking are also prohibited.
It is also necessary to limit salt intake and eat small portions 6 times a day. Dishes should always be served warm. It is necessary to exclude all products with a high content of extractives or essential oils (fish, meat broths, cocoa, coffee, etc.), fresh berries, vegetables, herbs, fruits, sour juices, carbonated drinks, marinades.
Prevention
If symptoms appear, you must immediately seek medical help. Ignoring abdominal pain can lead to serious damage to the gastrointestinal tract. In order to prevent the disease, you need to accustom yourself to small meals at the same time and avoid snacking. This is how we teach our body to produce juices, liquids and enzymes only when food is ingested. If the body does not know when to expect food, it works constantly. The same gastric juice will eat away at the stomach if there is no food in it.
It is important not to overeat and eat food only when it is warm. Few people know that hot food is harmful to the intestines. A healthy habit will be to exclude fatty, fried and spicy foods from your diet, even in small quantities. You need to consume less dairy products, especially fatty ones. It is recommended to cook porridge in water. Patients must strictly monitor their diet: no processed foods, canned food, pickles or fast food products.
Under no circumstances should you drink alcohol. It is absolutely contraindicated in any quantity if there is a hereditary risk of developing pancreatitis or the diagnosis has already been established. Smoking is also prohibited. Although doctors agree that nicotine does not cause pancreatic disease, it can trigger an attack. And, of course, it is necessary to eliminate stressful situations from your life.