Learn more about diseases starting with the letter “A”: Abdominal migraine, Absence, Brain abscess, Abuse headache, Agnosia, Pituitary adenoma, Adrenoleukodystrophy, Acalculia, Akathisia, Alternating syndromes, Amaurotic idiocy, Werdnig-Hoffmann amyotrophy, Kugelberg-Welander amyotrophy, Amnesia, Angioneurosis, Cerebral aneurysms, Anomalies of brain development, Chiari anomaly, Kimerli anomaly, Apallic syndrome.
Kimerli's anomaly is a pathology that can be either acquired or congenital. This disease occurs in 12-30% of people on Earth. The disease consists of the presence of an additional bone arch in the structure of the first cervical vertebra. The free movement of the vertebral artery with the help of this arch is limited, and artery compression syndrome also appears.
The anomaly manifests itself in the form of tinnitus, uneven gait, dizziness, muscle weakness and lack of coordination. In the presence of pathology, ischemic stroke and TIA may occur. To detect this pathology, duplex scanning of the vessels of the head and neck is used, magnetic resonance angiography and radiographic examination of the craniovertebral junction are performed. Vascular disorders must be treated conservatively and comprehensively.
Kimerli's pathology is a craniovertebral malformation, that is, congenital disorders in the structure of the articulation of the skull and the first cervical vertebrae. The anomaly causes both compression of the vertebral artery and chronic ischemia in the posterior regions of the brain. This ailment in itself does not belong to a number of diseases and its presence in the body does not indicate that this is the cause of all disorders in the area of the vertebral artery.
When examining patients with this anomaly, only one out of 4 people shows a relationship between the anomaly itself and the development of the syndrome.
Pathogenesis of vascular disorders in Kimerli anomaly
To understand why Kimerli's anomaly is a serious pathology, it is necessary to first consider the structure of the spine. It is worth knowing that the left and right vertebral arteries arise from the subclavian arteries and then pass along the cervical spine. In this case, these arteries are located in a canal, which is formed by the openings of the vertebral processes. The vertebral artery then enters the foramen magnum and enters the skull.
The vertebral arteries, together with their branches, form the vertebrobasilar system, which supplies the cerebellum, brain stem and spinal cord. These arteries also bend around the cervical vertebra, after which they pass through a wide bony groove. If a patient has a Kimerli anomaly, a bone arch is formed above the bone groove, which limits the movement of the vertebral artery in this place.
Kimerli's anomaly is almost always a congenital pathology. But it does not always provoke serious health problems for the patient. Typically, clinical manifestations of pathology that worsen the patient’s quality of life occur against the background of the following diseases:
- vasculitis;
- arterial hypertension;
- atherosclerosis;
- cervical spondyloarthrosis;
- cervical osteochondrosis;
- presence of craniovertebral malformations;
- traumatic brain injury;
- scarring process;
- spinal injury.
Kimmerli anomaly (syn. Kimmerli, Kimerli, Kimmerle)
- an abnormal bone ring (complete/incomplete) around the vertebral artery (one/both) in the area of the posterior arch of the first cervical vertebra. It leads to limited mobility of both the artery and the entire craniovertebral joint. The frequency is 10%. The thickness of the bridge that forms a ring around the vertebral artery varies. It can be continuous, ossified, discontinuous, unilateral or bilateral. To date, this is not an indication for surgical treatment. Bone bridge of the atlas, described in 1923 by H. Hayek. It is located between the posterior edge of the articular process of the atlas and the posterior border of its arch and forms an opening through which the vertebral artery (VA) and the occipital nerve pass. This pathology was described in more detail in 1930 by the Hungarian doctor A. Kimmerle, who drew attention to the fact that this change can lead to cerebral circulatory disorders, and subsequently received his name - Kimmerle anomaly (AK). The development of this bone pathology is based on a discrepancy between the nervous elements of the spinal cord and vertebral tissues. These include occipitalization of the atlas or remnants of the protoatlas with progressive growth, gradual calcification of the atlanto-occipital membrane with microdamages or microhemorrhages received during CVO injuries. As a result of these changes, the PA passes not in the groove of the arch of the atlas, but in the hole formed on one side by the groove, and on the other by the ossified atlantooccipital ligament, which forms a kind of bone bridge. It limits the free movement of the PA and occipital nerve when moving the head, especially when turning it.
A.A.
Lutsik (1988) attaches paramount importance to cicatricial degeneration of the arterial wall and periarterial tissue due to prolonged trauma to the VA in the area of the arterial valve, which leads to the development of intimal damage, early formation of atherosclerotic plaques, narrowing the lumen of the vessel, and/or dissections. As a result, sudden movements of the head can provoke a process of destabilization of the hemodynamics of the affected artery and turn into a source of disturbances in the blood supply to the distal parts of the vertebrobasilar system (VBS) according to the Bow Hunter Stroke mechanism. Thus, the pathogenesis of hemodynamic disorders in the VBS with AK is etiologically determined by the development of a complex compression-stenotic irritative effect, as a result of which there is a decrease in volumetric blood flow in the VA and the development of circulatory failure to varying degrees in the VBS. Anatomical studies reveal various variants of AK in approximately 30% of the population. In patients with clinical vertebrobasilar dysfunction (cochleo-vestibular disorders, ataxia, visual disturbances, etc.) or with myofascial pain of the Tonzik syndrome type, AK is detected in 7.6% of cases. The bridge can be incomplete, one- or two-sided, so there are different degrees of this anomaly. It should be noted that the thickness of the bridge and the size of the hole also vary significantly.
The clinical picture of the initial manifestations of AK is characterized by a variety of symptoms (dizziness, autonomic dysfunction, headaches, transient changes in vision, neck pain), which creates difficulties in determining the prevalence of the initial manifestations of AK, which are due to the fact that periodic headaches occur in the initial stages of the pathology patients, and often doctors, do not consider it a serious disease. Thus, they are observed for a long time with various diagnoses, such as “migraine”, “cephalgia”, “tension headache”, “VSD”, etc. from different specialists, they receive heterogeneous examination and treatment, which, as a result, does not allow the formation of the necessary statistical base.
In the advanced stage, which develops in 20% of all cases of AK, the clinical picture of the disease is dominated by symptoms of ischemia of the structures fed by the VBS, such as initial manifestations of cerebral circulatory failure (CIF) and/or paroxysmal cerebrovascular accidents (CVA). NPNMC manifest themselves in the form of dizziness, hearing impairment, noise, ringing in the ears, headache in the back of the head, sensations of “dots or sand” in front of the eyes, and sometimes color photopsia. During the interictal period, patients complain of blurred vision, pressure in the external auditory canal, noise, hyperacusis, fatigue, and sleep disturbance. There are no focal neurological symptoms. The dependence of each symptom on the movement of the body in space is clearly visible. PNMK are characterized by more pronounced symptoms: paroxysmal non-systemic dizziness, often with nausea, vomiting (when straightening and turning the head); hearing impairment (noise, ringing in the ears); headaches (mainly in the occipital region); visual disturbances (blurred vision, photopsia, visual field defects); pathological pyramidal signs; sensitivity disorders; cerebellar and bulbar symptoms; mono-, para- or tetraparesis; sudden falls without loss of consciousness (drop-attacks); sudden falls with loss of consciousness (Unterharnscheidt's syndrome). All symptoms of PNMK should persist for no more than 24 hours.
The most pronounced complication of circulatory disorders in the VBS is ischemic stroke in the VBS system, in which small foci of softening are formed in the cerebellum and medulla oblongata, which is clinically manifested by persistent neurological failure in the form of general cerebral and focal neurological symptoms, damage to the mid-stem and cerebellar structures, which persist in patients for more than 24 hours.
Gulyaev S.A., Kulagin V.N., Archipenko I.V., Gulyaeva S.E. (2013) conducted a study to analyze the incidence of AK in the structure of a neurological hospital, develop criteria for its diagnosis and rational methods of therapy. The study used the results of a screening examination of patients hospitalized at the neurological clinic of the State Educational Institution of Higher Professional Education of VSMU over a period of 6 years (total 8,436 people). The exclusion criterion was the presence of verified traumatic brain injuries and injuries of the cervical spine, vascular anomalies, and tumors of this area. In addition to clinical and neurological examinations, the complex of examinations included radiography of the spine and skull, CT, MRI of the brain and spinal cord, ultrasound examination of the vessels of the neck and brain (USDG, DS), EEG. All examinations were carried out over a three-year follow-up period with a frequency of 2 to 6 times a year. The study identified 68 patients with AK aged from 18 to 67 years, among them 42 (61.8%) women and 26 (38.2%) men. In most cases (74.6%), the clinical manifestations of the neurological defect became stable by 20–25 years. However, anamnesis studies showed that 43.8% of those examined had previously had specific complaints indicating the presence of CVO pathology, which were regarded by specialists as spastic torticollis, cervicobrachialgia, syncope, hemocerebrospinal fluid dynamics disorders, etc.
Research results
The clinical picture identified in patients with AK was characterized by a variety of symptoms, but, taking into account the leading clinical sign, 3 main neurological syndromes were identified:
1. Pain syndrome, characterized by a half-type headache localized predominantly in the occipital region (91.6% of cases) with irradiation to the eye or ear canal, accompanied in 43.9% of cases by photopsia, loss of visual fields (34.6%) or metamorphopsia (21.5%)
2. Vascular insufficiency syndrome, manifested in 42.6% of cases in the form of dizziness (79.4%), unsteadiness when walking, unstable disturbances in coordination tests (61.7%), accompanied in 54.4% of cases by nausea and vomiting. Less often, patients noted the appearance of noise illusions in the form of buzzing, rustling, squeaking, whistling, localized either in the ear or in the head (45.8%). A characteristic feature of this syndrome was its connection with head turns, manifested in its increase during movement, which forced patients to take a certain position (the so-called head positioning)
3. Vegetative syndrome (panic attack syndrome) was recorded in 41.1% of those examined, characterized by a sudden development with the appearance of a feeling of “hot flash” to the head or neck, accompanied by unmotivated fear, anxiety, a feeling of suffocation with pronounced dysfunctions of the autonomic nervous system (chill-like trembling , numbness of the hands, instability of blood pressure, etc.). At the end of the attack, patients experienced polyuria and panasthenia. Their duration ranged from tens of minutes to several hours
Observation of patients over time allowed us to identify three degrees of severity of the disease:
I mild – characterized only by the presence of pain in combination with hemo-cerebrospinal fluid-dynamic disorders; II medium – manifestations of the first degree were accompanied by autonomic dysfunctions of a permanent and paroxysmal nature with a frequency of paroxysms 3–4 times a year; III severe - with it the frequency of the main syndromes ranged from monthly to weekly. Follow-up analysis showed a direct dependence of the severity of the course on the duration of the disease and the possibility of a gradual and progressive transformation of clinical forms of the disease from mild through moderate (68.7±0.3%, p<0.05) to severe (31.3±0.2% , p<0.05).
Classification of Kimerli anomaly
The correctly selected method of treating a disease is largely determined by its type. In neurology, it is customary to distinguish two main types of Kimerli anomaly. The first is characterized by the formation of a bone arch that connects the process of the atlas with the posterior arch. The second type of anomaly involves the presence of a bone arch located between the transverse and articular processes of the atlas.
There are also complete and incomplete types of pathology. With a complete anomaly, the shape of the bone arch resembles a semi-ring, and with an incomplete anomaly, it resembles an arched outgrowth. Kimerli's anomaly can be localized both on both sides of the vertebra and on one side. It is also common to distinguish between acquired and congenital forms of the disease.
As for the acquired pathology of Kimerli, it is usually formed against the background of various chronic pathologies of the spine - for example, with osteochondrosis. In patients with an acquired anomaly, there is usually such a deformation of the groove in which it is closed from above by a ligament.
Kimerli's congenital anomaly is a consequence of developmental defects and does not pose a serious danger to the patient, therefore it does not require special treatment. On the contrary, the acquired form of the disease requires complex treatment, since it is characterized by severe symptoms that threaten the health and life of the patient. The most severe cases of the disease are accompanied by neurological disorders due to poor blood supply and compression of the spinal artery.
Types of pathology and their symptoms
Neurologists distinguish two main types of damage:
- A complete anomaly
. It suggests the presence of an atlanto-occipital ligament, in which, over time, hardening and closure of the ring in the posterior section is observed. This process is characterized by noticeable compression of the artery and serious disturbances. - Incomplete
. There is no closure, only one bone arch is observed. In some cases, it is not detected due to the absence of certain symptoms. When diagnosing, it requires observation by the attending physician.
By type of formation there are:
- Congenital form
. The pathology begins in the womb, so it is impossible to prevent its occurrence. The lesion is not genetically transmitted and manifests itself in children of school age, especially during active physical activity. Requires constant medical supervision, physiotherapeutic procedures and maintenance medications. - Acquired
. It becomes a complication of diseases of the spine, cartilage and bone tissue. Often occurs with the progression of osteochondrosis. Therapy requires an integrated approach, since damage can cause other neurological disorders.
By localization:
- One-sided
. It involves damage to only one artery and progresses only on one side of the spine. - Double-sided
. Accordingly, it affects both vertebrae and compresses both arteries.
In all varieties, the symptoms are similar, so anamnesis is not the main diagnostic measure in determining the defect.
Before starting treatment, it is necessary to determine the causes and location.
The lesion is not inherited, so the pathology can be diagnosed in a child with absolutely healthy parents.
Most often, radiculitis becomes a consequence of spinal injuries or the active progression of osteochondrosis. Usually the lesion is diagnosed in old age, but in recent years more and more cases of the disease have been reported in people over 30-35 years of age. Read more in the article: “how to treat lumbar radiculitis at home.”
Symptoms of Kimerli anomaly
Various manifestations of the disease, which cause severe discomfort to the patient, are usually triggered by a decrease in blood flow to the posterior parts of the brain. As a result of this pathological process, the patient experiences noise in one ear or both. The nature of this noise can be different - hum, whistle, ringing, hissing. For the same reason, there is flickering or flickering before the eyes, as well as sudden darkening in the eyes.
Kimerli's anomaly is characterized by impaired blood supply to the cerebellum, which leads to such clinical manifestations of the disease as frequent dizziness, lack of coordination and unsteadiness of gait. Usually, all these conditions only intensify when turning the head. Constant muscle strain and uncomfortable head position lead to the patient often losing consciousness. Another unpleasant symptom of the disease is the appearance of sudden muscle weakness, which leads to the patient falling without a previous loss of consciousness.
Severe cases of the disease are characterized by more complex and unpleasant symptoms. In patients with severe forms of Kimerli's anomaly, clinical signs of the disease are observed, such as tremor of the arms and legs, headache, nystagmus, hypoesthesia of the face or trunk, coordination disorders, and motor disorders of the extremities. The most life-threatening complication is ischemic stroke.
Risk factors and causes
The acquired form of the disease can occur against the background:
Pay attention to the most common causes of the anomaly of Kimmerliarterial hypertension;- osteochondrosis of the cervical spine;
- neck vascular diseases;
- instability of the cervical vertebrae;
- direct head injuries;
- spinal injuries;
- spondyloarthrosis or spondylosis of the cervical spine;
- shoulder injuries on the side where the anomaly is located;
- craniovertebral diseases, for example, Arnold-Chiari malformation;
- scars and other craniovertebral malformations (congenital pathologies in the area of connection of the cervical vertebra and skull).
The most common congenital anomaly , which develops due to bad habits and infectious diseases of the pregnant woman, and unfavorable living conditions of the expectant mother. The congenital form of the disease is present in 10% of newborns.
Consequences
Kimmerly's anomaly can lead to the development of neurological disorders . The most severe complication of the disease is ischemic stroke with patient disability or death. The disease is also accompanied by frequent loss of consciousness, which can lead to falls and all kinds of injuries (including to the head).
Diagnosis of Kimerli anomaly
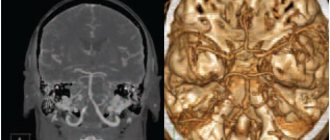
Kimerly's anomaly is a serious neurological disease, the effective treatment of which depends on timely and accurate diagnosis. Of great importance in diagnosing pathology is the collection of anamnesis and neurological examination of the patient. Typically, patients consult a doctor with symptoms of Kimerli's anomaly, which indicate a disruption of the circulatory process in the vertebrobasilar region. The doctor primarily prescribes diagnostic methods such as radiography of the skull and spine. These techniques are very effective, since Kimerli's anomaly is quite clearly visible on lateral radiographs of the craniovertebral zone.
If a patient complains of tinnitus, the doctor needs to exclude possible ENT diseases: cochlear neuritis, labyrinthitis, chronic otitis media. For this purpose, it is advisable to refer the patient for examination to an otolaryngologist. Differential diagnosis also involves conducting various hearing tests, such as experiments with tuning forks, speech, noise and tone audiometry. Additionally, studies of the vestibular apparatus may be prescribed: electronystagmography, vestibulometry, stabilography.
Kimerli's anomaly is not always provoked by vertebral artery syndrome, so the neurologist will need to exclude other causes of this pathological process during diagnosis. For example, using contrast angiography, it is possible to detect compression of a vessel by formations such as a cyst, tumor, brain abscess, arteriovenous malformation, thrombosis, and cerebral aneurysm.
Diagnosis of the disease also involves determining the degree of its influence on blood circulation in the vertebrobasilar region. This can be done with the help of additional studies such as transcranial Doppler sonography, ultrasound of extracranial vessels, MRI and duplex scanning of cerebral vessels. All these instrumental techniques make it possible to determine the location of compression of the vertebral artery and disruption of its functioning, depending on the position of the neck and head.
Therapeutic methods
There is no need to treat the classic type of mild to moderate Kimmerle anomaly. In such cases, the patient is indicated for supportive therapy and observation. Goals and objectives of treatment:
- elimination of painful symptoms and reduction of periods of exacerbation of pathology;
- normalization of blood supply to tissues;
- improvement of muscle condition and tone;
- reducing the likelihood of complications and consequences for other body systems;
- improving and maintaining the patient’s quality of life.
In severe situations, the patient may be indicated for surgery. The purpose of the intervention is to remove the bone growth that is pressing on the vessels and arteries. This treatment option allows you to get rid of the lesion without its further manifestation.
Drug effects
Medicines do not eliminate the causes of diseases and do not eliminate pathology. Medicines relieve pain and inflammation, improve nutrition and blood supply to tissues. For exacerbations use:
Advertising:
- Cerebrovascular stimulants
(Actovegin, Nitsergolin, Sermion, Cavinton, etc.). Prevents the occurrence of vascular insufficiency. - Means for stabilizing blood pressure
(Anaprilin, Furosemide, Captopril). - Vitamins and supplements
(Gingko Biloba, B vitamins, neuroprotectors). Prevents the development of hypoxia, normalizes metabolic processes in soft tissues. - Antispasmodics and muscle relaxants
(Ditilin, Esmeron). Relieves muscle tension and tension, helps reduce pain.
Medicines are selected and combined depending on individual characteristics. Additionally, painkillers and chondroprotectors may be prescribed. Osteochondrosis requires anti-inflammatory medications.
Physiotherapy
Physiotherapy is one of the key methods of intervention for pediatric and adult patients. In maintenance therapy the following are used:
- hirudotherapy;
- electrophoresis with analgesics;
- acupuncture.
In all cases, therapeutic physical training is also used (necessary to strengthen the muscle corset), massage of the cervical-collar area (to improve blood supply and restore muscle tone). It is not recommended to use the methods yourself at home, since incorrect implementation can aggravate the situation. Patients often sign up for manual therapy sessions with professional massage therapists.
Advertising:
Additional Methods
At home, it is allowed to use a Shants collar, a massage pillow, and treatment with bee venom. These methods of influence can be used with the permission of the attending physician in the absence of contraindications. With increased emotional excitability and irritability, sedative medications, tranquilizers, and sedatives are prescribed. The patient is also shown systematic rest and rest, proper distribution of loads on the spinal column.
Kimmerle's anomaly is a conditionally pathological condition of the patient, and therefore does not require mandatory radical treatment. The active manifestation of the disease in the form of persistent pain, incoordination, and discomfort is suppressed with the help of medications, manual therapy, and physical therapy. This approach allows improving the quality of life of patients without surgical intervention.
Treatment of Kimerli anomaly
Treatment of Kimerli's anomaly is not necessary in all cases. Indications for treatment may include serious clinical symptoms of circulatory disorders caused by the disease. Patients in whom Kimerly's anomaly has caused vascular insufficiency are usually prescribed conservative treatment. In particular, to improve cerebral blood flow, vascular therapy is prescribed, which involves taking drugs such as Cavinton, Sermion, cinnarizine, Devincan.
To improve real blood parameters, trental and pentoxifylline are prescribed. Complex therapy for the disease also involves taking neuroprotectors, antioxidants, nootropics and metabolic medications (ginkgo biloba, piracetam, mildronate, picamilon).
Recovery prognosis
Treatment of a disease does not always bring the desired result. Conservative therapy can improve the patient’s condition and make blood flow more active, but a number of symptoms may still persist . For example, ringing or noise in the ears is difficult to correct, and many patients have to put up with it. As for the prognosis for life, it is usually favorable. In the absence of pronounced symptoms and timely treatment of minimal blood flow disorders, nothing threatens a person’s life.
Surgery
In most cases, treatment of Kimerli's anomaly is limited to conservative methods and does not require surgical intervention. The need for surgery may be due to a decompensated manifestation of vertebral artery syndrome, which provokes a serious circulatory disorder in the vertebrobasilar region. During surgery, the doctor performs mobilization of the vertebral artery and resection of the pathological arch. After the operation, the patient will need to undergo a rehabilitation period, during which he will have to wear a Shants collar for 2-4 weeks.
What it is?
Kimmerly's anomaly is understood as a pathological change in the atlas (1st cervical vertebra), accompanied by the appearance of an additional bone arch in the form of a semiring (arched outgrowth).
Kimmerly's anomaly is a pathological change in the first cervical vertebra
Classification/Grades
Kimmerly's anomaly may be:
- congenital (the disease is present from birth);
- acquired (the disease develops due to dystrophic diseases of the spine).
Depending on the severity, the anomaly may be:
- Full. A bone arch in the shape of a half ring is diagnosed, as well as the atlanto-occipital lateral ligament, which gradually ossifies due to the deposition of calcium salts. The result is severe compression of the vertebral artery and rapid progression of the disease.
- Incomplete. There is only an additional bone arch in the form of an arched outgrowth.
Depending on the location, there are:
- One-sided anomaly. The disease occurs on one side of the vertebra. In this case, only one vertebral artery is compressed.
- Bilateral anomaly. The disease develops on both sides of the vertebra. Two vertebral arteries are affected.
ICD 10 code
The disease code is in section Q10-Q18. This includes all congenital malformations .
Prevalence
It was previously thought that Kimmerly's anomaly occurs in 10% of people. The widespread use of MRI and radiography has made diagnostic results more accurate. Today it is known that about 30% of the planet's inhabitants suffer from the disease .
Additional measures
Patients diagnosed with a mild form of Kimerly's anomaly should definitely adhere to certain precautions that will help them avoid serious complications. Namely, they need to avoid in every possible way sharp turns of the head, excessive physical exertion, performing physical exercises while standing on their heads, as well as sports games and activities that involve hitting their heads. Such activities include football, gymnastics, basketball and others.
Before a session of manual therapy or massage, the patient must warn the attending physician about the presence of Kimerli's anomaly. He must remember that in the event of a sharp deterioration in his health, he needs to urgently consult a neurologist for advice so as not to miss the early stage of the disease and begin treatment on time.
Preventive measures
If you exercise, you should consult with a qualified physician about the safety of these activities. Together, choose the most suitable therapeutic exercises to improve blood flow. You can contact an experienced chiropractor who, with his “magic” hands, can improve blood circulation in the neck area where the disease is located.
In addition to all of the above, sometimes it’s enough to walk in the fresh air more often. Such walks stimulate the immune system and stabilize a person’s general condition, help improve blood pressure and limit the production of the stress hormone, which is found at almost every step of modern people.
Kimmerle anomaly in children
As a rule, this pathology is diagnosed at an early age by chance. Kimmerle anomaly is formed in a child at the stage of intrauterine development, but a specific cause for this process has not been identified. A child can live with this disorder for a long time and not suspect it. An aggravating factor may be:
- scoliosis;
- osteochondrosis;
- strong physical activity;
- prolonged sitting position (for example, at a computer).
Due to compression of the blood supply channel to the brain, children may study worse, and endurance may be reduced. The following symptoms actively manifest themselves as Kimmerle disease progresses:
- nausea;
- prostration;
- weakness;
- vegetative-vascular dystonia;
- dizziness;
- unstable emotional background.
Prevention of Kimmerly anomaly
Preventive measures for acquired Kimmerli anomaly include:
- adherence to the principles of proper nutrition;
- sufficient fluid intake (from 2 liters per day);
- regular exercise;
- taking massage courses;
- correct lifting of weights (do not hold heavy objects on outstretched arms, put stress on your legs);
- uniform load distribution when carrying heavy objects.
Sports with Kimberly anomaly are not contraindicated. Patients can ski, roller-skate, do water aerobics, swimming, and horse riding. But, before enrolling in a specific sports section, you need to consult a doctor. Lifting heavy objects (especially placing a barbell on your neck) is prohibited. It is also important to avoid forced loads and sharp turns.
Kimmerle anomaly - how to live with it
A person who acquires the disease after birth experiences a significantly reduced quality of life. When the first symptoms appear, the patient wants to know how to live with Kimmerle anomaly. Many people experience all of the symptoms described above, but do not associate them with the disease. Sometimes they make mistakes with the diagnosis and doctors, based only on the symptoms described by the patient, lead to the prescription of incorrect treatment.
Kimmerle can lead to impaired coordination, memory, loss of sensitivity, and decreased mental abilities. The worst scenario is an ischemic stroke, which leads to death. To prevent the disease, it is recommended to closely monitor your health; if you receive injuries or the first signs appear, consult a doctor. It is recommended to exercise moderately, spend more time in the fresh air, and monitor your body weight.
Physiotherapy
This is one of the treatment options that help cope with the manifestations of the disease. Exercises for Kimmerli anomaly are therapeutic in nature, aimed at stretching the suboccipital muscles, this is special gymnastics for the cervical spine. The full effect of therapy can be obtained if the condition of the entire ridge is normalized and posture is improved. This therapy will help normalize blood flow and relieve muscle pressure around the vertebral artery.
- What is fibrofatty involution of the mammary glands?
- Staphylococcus aureus in the nose
- Adhesive disease of the abdominal cavity - prevention and treatment. Symptoms of abdominal adhesive disease, diet
Massage
This is one of the options to relieve tension in the cervical spine and improve blood flow to the brain. Massage for Kimmerle anomaly must be performed by a qualified specialist. If you come to a massage therapist for the first time, you must warn him about the presence of an anomaly so that he takes this into account and selects the appropriate technique. The procedure will help relieve muscle spasms and improve overall well-being. Under the supervision of a doctor, you can use different massage applicators.
Why is the Kimmerle anomaly dangerous?
One of the first questions of patients who learned their diagnosis: will life expectancy decrease and what are the consequences of the anomaly? The pathology does not pose a mortal danger; only in some cases, when the course of the disease is advanced and no treatment is carried out, a stroke may occur. In other cases, the disease causes migraines and has a deforming effect on the structure of blood vessels, which leads to impaired blood circulation in the brain.
Chronic pain and other symptoms of Kimmerle disease sharply reduce a person’s standard of living, the patient cannot perform active activities, and with physical activity the symptoms worsen: problems with coordination, numbness, movement of the eyeballs. All this becomes a harbinger of a stroke in the craniovertebral region. It is necessary to take an x-ray for an accurate diagnosis, begin treatment for Kimmerle pathology and follow all the doctor’s instructions. All this will help avoid complications.