Causes of pathology
Fibrillation and ventricular flutter occur due to the pathology of impulse transmission through the myocardium.
These rhythm disturbances are successive stages of the development of one process. In ICD-10 (International Classification of Diseases, 10th revision) they are classified under one heading. Dysfunction of the cardiac pathways can occur as a result of:
- large scar (consequence of myocardial infarction);
- focal post-infarction cardiosclerosis;
- coronary heart disease;
- acute myocardial infarction;
- cardiomyopathy with severe hypertrophy of cardiomyocytes;
- dilatation (stretching of the walls) of the heart chambers;
- arrhythmogenic cardiomyopathy;
- myocarditis (inflammation of the heart muscle);
- valve defects;
- severe intoxication (including alcoholism).
Symptoms and signs of ventricular fibrillation
VF is a life-threatening condition. It develops suddenly, and the victim very quickly develops a picture of clinical death. However, if it is preceded by ventricular flutter (contraction of muscle fibers with a frequency of more than 200 times per minute), the patient may have time to complain about:
- chest pain;
- sensation of accelerated heartbeat (2-3 times per second or more);
- dizziness, loss of orientation in space;
- nausea, which may progress to vomiting;
- increased sweating;
- disturbed rhythm and difficulty breathing;
- general weakness.
These symptoms may last no more than 15-20 seconds. When VF develops, the patient loses the ability to speak coherently. During inspection, you need to pay attention to:
- unconscious state;
- pallor of the skin with acrocyanosis (bluish color of the earlobes, tip of the nose);
- convulsive muscle contractions (occur 35-45 seconds after the onset of the attack, may be accompanied by involuntary urination or defecation);
- a state of clinical death that will occur 2 minutes after the onset of VF if help is not provided: dilation of the pupils (normally they narrow if a person raises their eyelids in a bright room, but here opening the eyes does not cause a physiological reaction);
- it will be impossible to feel the pulse (both on the radial artery (peripheral, runs at the wrist) and on the main ones (large: carotid, femoral);
- breathing movements will stop.
However, to confirm the diagnosis, it is necessary to conduct an instrumental study - electrocardiography.
Anticoagulants can only be taken as prescribed by a doctor.
Standard dosage: Xarelto 20 mg / once a day Eliquis 5 mg / 2 times a day Pradaxa 150 mg / 2 times a day
Studies show that patients are more comfortable taking Xarelto - taking it once a day is easier to remember, especially for older people.
"Wafarin": take one tablet in the evening, take the INR test after 3-4 days. If the INR does not reach 2.0, then the doctor should increase the dosage. The INR should be taken every 3-4 days until the desired level is reached. Then you need to take an INR test every 3 weeks.
Important: all medications and their dosage are prescribed strictly during an in-person consultation with a doctor! This information is for informational purposes only and cannot be a guide to action. Self-medication for arrhythmia is unacceptable and can have serious health consequences.
| Reducing the dosage of anticoagulants mainly depends on only three parameters: — Creatinine clearance is less than 50. — The patient’s weight is less than 65 kg. — The patient’s age is over 85 years. In other cases, reducing the dosage risks a stroke. |
How does the disease manifest itself on an electrocardiogram?
Ventricular fibrillation on an ECG (electrocardiogram) has several stages of development:
- Ventricular flutter. Lasts several seconds, myocardial contractions are still coordinated. On the ECG it appears in the form of high-amplitude (with a large distance between the upper and lower bending points) rhythmic waves (there can be 250-300 such complexes per minute).
- Convulsive stage. The high-amplitude waves remain, but now their frequency is on the order of six hundred per minute. This is a manifestation of chaotic uncoordinated contraction of individual sections of the myocardium lasting 55-65 seconds.
- Ventricular fibrillation. Deterioration of contractility leads to dissociated contraction of individual groups of cardiomyocytes. The ECG records small (low-amplitude) waves with a frequency exceeding 100 per minute.
- Atonic stage. The energy reserve of the myocardium is almost completely exhausted. There are damped contractions of individual sections of the heart muscle. The waves become even lower and smaller, now their frequency does not exceed 400 per minute.
Photos and examples of film with VF
Let's look at examples of electrocardiographic films and descriptions of them.
- Ventricular flutter
- Stages: convulsive;
- ventricular fibrillation;
- atonic.
Treatment and algorithm for helping with VF
Since VF is a condition that poses an immediate threat to the patient’s life, there is a documented protocol for action when such a paroxysm occurs. Since the patient is often treated after the transition to a state of clinical death, it all begins with resuscitation.
If a person is found during a convulsive period of VF, then all that needs to be done is to gently restrain the head from hitting the underlying surface. You can add folded clothing to mitigate their effects. It is forbidden to open the victim’s mouth, take out his tongue or hold his limbs.
Urgent actions
Algorithm of actions in order of priority:
- Check the patient’s consciousness: call by voice; if he does not respond, lightly shake his shoulders (so that the head does not come off the surface on which it lies and does not fidget on it; the direction of movement is from top to bottom).
- Assess for the presence of a pulse. To do this, it is recommended to clasp the central part of the neck (trachea) in the upper half with the fingers of one hand.
- If there is no pulse, call an ambulance (or have someone do it).
- Check for breathing. You need to lean your cheek towards the victim’s mouth and nose, observing the amplitude of movements of the chest and at the same time feeling the air movement (if present) with the skin. If necessary, clear the airway.
- Perform indirect cardiac massage (in this situation this is the most important) and artificial respiration.
When the emergency medical team arrives, they:
- continue to carry out resuscitation measures;
- connect a cardiac monitor and defibrillator (in modern models these two devices are combined);
- after recording an electrocardiogram and confirming the presence of VF, defibrillation is performed (discharges are delivered with increasing intensity every 2 minutes, against the background of chest compressions, until the rhythm normalizes);
In the absence of a defibrillator, it was previously recommended to perform a precordial blow (with a fist on the lower third of the sternum), but due to injuries and complex technique, it is now not recommended for use.
- if necessary, the following medications are administered: adrenaline;
- amiodarone;
- lidocaine.
What treatment should a patient with ventricular fibrillation receive?
Emergency care for ventricular fibrillation must include defibrillation. Waves of depolarization roll chaotically through the myocardium, and therefore performing chest compressions or using medications will most likely be ineffective.
When the patient is restored to sinus (normal) rhythm through the efforts of the ambulance team, there remains a risk of relapse. To reduce the risk of a recurrent attack, the following medications are prescribed:
| Group of drugs | Representatives | Destination purpose |
| Antiarrhythmic | Lidocaine Amiodarone | Prevention of recurrence of ventricular fibrillation immediately after an attack |
| Bisoprolol Nebivolol | Maintaining an adequate heart rate in the long term | |
| Oral anticoagulants | Warfarin Rivaroxaban | Preventing the formation of blood clots and embolism (blockage) of blood vessels |
| Infusion therapy | Stereofundin Ringer's Lactate Trisol Chlosol Sodium Bicarbonate | Restoring the body’s water-electrolyte balance (it ensures adequate processes of excitation and contraction in the heart cells) |
Are there surgical techniques?
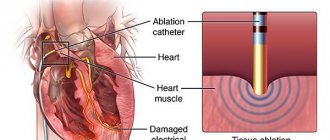
- Implantation of a cardioverter-defibrillator. This device is attached near the left collarbone, and electrodes from it are guided to the heart. It monitors the regularity of your heart rate. When VF paroxysm occurs, this device delivers a shock.
- Coronary angioplasty (stenting of coronary arteries). If VF occurs against the background of coronary heart disease, this surgical operation will remove the very cause of the paroxysm and prevent relapse.
- Coronary artery bypass grafting (bypass routes to restore blood flow in the basin of one of the coronary arteries). It makes sense if the onset of VF was preceded by an ischemic attack.
Anticoagulants thin the blood - is it dangerous?
Like any blood thinners, anticoagulants can cause bleeding. However, the risk of bleeding is 10 times lower than the risk of stroke. If a person has spontaneous bruises, nosebleeds, heavy menstruation, or blood in the urine, this is not an indication that the dosage needs to be reduced. Minor bleeding does not cause death, unlike a stroke. If you have the above symptoms of bleeding, you need to come for an examination to your attending physician - a gynecologist, urologist and, of course, a cardiologist.
| If a person takes anticoagulants, he must take a general blood test, creatinine, glomerular filtration rate (creatinine clearance), potassium, sodium, ALT, AST every 6 months. |
How does VF affect the duration of future life?
If defibrillation is successful (and it is more effective in large-wave forms of VF), the patient survives and the prognosis for future life is relatively favorable.
During ventricular fibrillation, the myocardium is more susceptible to damage (large infarction) as a result of lack of oxygen (hypoxia). This may increase the risk of sudden death, especially if:
- there is atherosclerotic damage to the coronary arteries;
- chronic physical inactivity is observed;
- the patient smokes;
- he drinks alcoholic beverages often and in large quantities;
- are overweight or obese;
- the person suffers from diabetes;
- arterial hypertension is present, and basic drug therapy is not used.
With properly selected antiarrhythmic therapy, the prognosis for life is favorable.
conclusions
Irregular contraction of individual muscle bundles in the ventricular myocardium causes their fibrillation. Without immediate cardioversion (restarting the rhythm), the likelihood of sudden cardiac death is very high.
The clinic is nonspecific: the patient is found unconscious, pale, often with no pulse, no breathing, and dilated pupils. The criterion for diagnosis is a characteristic electrocardiographic pattern (waves of different amplitudes).
Specific therapy is defibrillator discharge. In the future, drug and surgical (if necessary) treatment makes sense.
Why do you need to control your lifestyle?
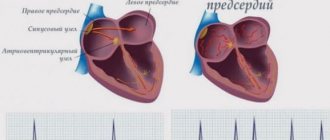
Because it affects the size of the left atrium. The more severe the obesity, the larger the size of the left atrium. If a person is overweight, the pressure in the heart increases, the volume of circulating blood increases, and the left atrium stretches. The larger the left atrium is from normal (400 mm), the higher the risk of developing atrial fibrillation.
Situations
With normal left atrium size, the effectiveness of radiofrequency ablation can reach 70%. The larger the size of the left atrium, the lower the effectiveness of RFA.
● If a patient is undergoing radiofrequency ablation, it is important to remember: the more abnormal the atrial function is, the higher the risk of recurrent atrial fibrillation. ● When a person’s heart rhythm is lost, during an ultrasound they pay attention to the size of the left atrium: if it is slightly dilated, it makes sense to try to restore this rhythm using medications or electrical pulse therapy. But if the left atrium is significantly dilated, there is no particular point in restoring the rhythm - sooner or later it will break down again.
What to do?
● Control your weight. ● Avoid alcohol - alcohol increases the risk of bleeding and aggravates the course of the arrhythmia or increases the frequency of breakdowns of this arrhythmia. ● Stop smoking. ● Stop taking dietary supplements - most of them can enhance the effect of anticoagulants. ● Increase physical activity. ● Monitor the condition of the thyroid gland by an endocrinologist.