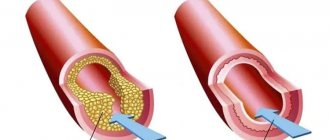
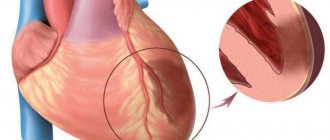
The first to describe the picture of myocardial infarction in 1892 was V. M. Kerning. Due to impaired coronary circulation, myocardial necrosis occurs, accompanied by thrombosis of the coronary artery and impaired blood supply to the heart muscle, which are called “infarction”. The disease takes the lives of both young and old people. There is also an increase in the incidence of heart attacks in people under 30 years of age. Statistics also show that heart attacks affect men and women differently. Most often, women suffer from it during menopause, when the amount of female hormone in the body decreases and the atherosclerotic plaque is destroyed, replaced by a blood clot that clogs the vessel. If this process occurs quickly, then an acute heart attack occurs, requiring immediate hospitalization. Representatives of the stronger sex are traditionally less likely to have a heart attack, but after 40 years of age, men get a heart attack approximately 4 times more than women, and starting from the age of 55, the number of cases in both sexes is comparable. A heart attack leads to irreparable consequences in 35% of cases.
What kind of heart attack happens?
The types of infarction are distinguished by where exactly the necrosis occurred, the depth and area of myocardial damage. In accordance with these criteria, in medical practice it is customary to distinguish the following classes of heart attack:
- Large-focal or extensive - with this form of the disease, the thrombus is significant in size;
- Small-focal occurs as a result of minor muscle damage and is usually asymptomatic;
- Lower - localized in the lower wall of the artery of the left ventricle;
- Anterior infarction is observed on the anterior wall of the left ventricle of the heart;
- Posterior – affects, respectively, the posterior wall of the left ventricle;
- Transmural is the most dangerous form of infarction, affecting the entire wall of the ventricle. Most often leads to death;
- Intramural – manifests itself throughout the entire thickness of the myocardium;
- Abdominal - localized on the posterior wall of the left ventricle, occurs as a result of other heart ailments;
- Recurrent occurs from time to time.
There are also various atypical forms of a heart attack, in which there are no pronounced symptoms. Approximately 10% of the disease occurs in this form.
Where is the lesion located?
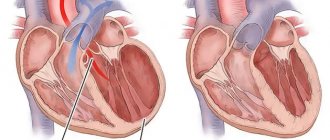
The “target” of lower myocardial infarction is the left ventricle - the main and most massive component of the muscle “pump”. Its size is 2-3 times larger than other parts of the heart. Thickness ranges from 11 to 14 cm, myocardial mass index is 109-124 g/m² for women and men, respectively. Blood supply is carried out through two important vessels - the right coronary and circumflex arteries. The most important arterial vessel, the aorta, emerges from this part of the heart.
Thus, I can conclude that the left ventricle needs abundant blood circulation and much more oxygen than other areas of the myocardium. In this regard, it is he who is affected as a result of a cardiovascular accident in almost 100% of cases. And the posterior wall, divided into the diaphragmatic and basal regions, is affected only in 10 - 15%. But I want to note that when it is involved in the pathological process, great difficulties arise in diagnosis. Standard 12 electrocardiographic leads do not record damage to a given anatomical segment (“silent” zone).
Inferior myocardial infarction in most cases is accompanied by damage to adjacent areas - posteroseptal, posteroinferior and posterolateral.
This combination saves the lives of many patients, as changes are clearly recorded on the ECG curve.
Symptoms of a heart attack
It should be remembered that cardiologists consider the pre-infarction state and, in fact, the myocardial infarction itself. Sudden onset of the disease was recorded in 43% of patients. About a month before an exacerbation, a person begins to feel unwell. Moreover, in women the symptoms are less pronounced and are similar to the flu or a cold. In men, the symptoms are classic. Many people note the presence of the following symptoms long before the attack occurs:
- Fatigue that does not go away even after sleep;
- Constant weakness;
- Sleep disorders;
- Dyspnea;
- Numbness or tingling of the extremities;
- Visual impairment;
- Anxiety;
- Pale skin;
- Increased sweating.
A typical heart attack has the following symptoms:
- Pain of extreme intensity of varying nature, localized in the chest and radiating to the arm, neck, left shoulder, ear, area between the shoulder blades. A proportion has been noticed: the more intense the pain, the larger the area of the heart muscle affected by necrosis;
- Wave-like pain attacks;
- Tachycardia;
- Arrhythmia;
- Blood pressure rises, then falls;
- Increased body temperature;
- Symptoms of heart failure.
Treatment
In the most acute stage of a heart attack, first of all, doctors relieve pain. For this purpose, various analgesics and narcotics (morphine) can be used intravenously. For a faster effect, painkillers are administered intravenously.
After the electrocardiogram is taken, thrombolytics are administered to restore coronary blood flow. To eliminate a pain attack, neuroleptanalgesia is performed.
Next, the patient is prescribed a set of drugs to reduce the myocardial oxygen demand, beta blockers to reduce the load on the heart, medications to thin the blood and reduce the level of blood clotting. If necessary, inhibitors, sedatives and hypnotics are prescribed. The combination of drugs depends on the presence of concomitant diseases in the patient and the severity of the heart attack.
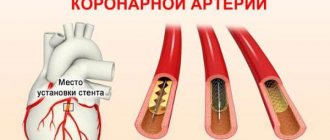
To treat a heart attack, surgical methods of restoring blood flow are used (coronary artery bypass grafting, balloon angioplasty).
During the first days of treatment, the patient is prescribed bed rest, and starting from days 3-4, the patient can sit on a chair for about an hour twice a day. With an uncomplicated heart attack, the patient is allowed to walk 5-7 days after the heart attack. In case of an uncomplicated form of myocardial infarction, the patient is discharged from the hospital on days 10-12; in case of complications, hospitalization can last up to 4 weeks.
Clinical guidelines
Clinical recommendations “Acute myocardial infarction with ST segment elevation of the electrocardiogram” were developed by the Russian Society of Cardiology with the participation of the Association of Cardiovascular Surgeons of Russia, approved by the Scientific and Practical Council of the Ministry of Health of the Russian Federation and approved by the Ministry of Health in 2021. The document contains information about the disease, forms of its diagnosis, symptoms, treatment methods, possible complications, care and rehabilitation.
Appendix B of the document contains recommendations for patients who have had a heart attack related to secondary prevention of the disease. The recommendations say that patients should stop smoking, ensure regular physical activity, follow a diet designed for such cases, lose excess weight, follow the doctor's recommendations, maintain low blood cholesterol levels with the help of medications, ensure stable normalization of blood pressure (if present). arterial hypertension), maintain normal blood sugar levels (in the presence of diabetes mellitus). In addition, with extensive damage to the heart muscle and/or complications of myocardial infarction, additional treatment is required, which is prescribed by a doctor. Stopping essential medications early is known to significantly increase the risk of another heart attack, death, and heart failure, which can significantly limit your daily activities. You should not stop taking medications without consulting your doctor. To reduce the risk of recurrent events (myocardial infarction, its complications), it is highly advisable for you to participate in a special rehabilitation program, including regular dosed physical activity, psychological support, and monitoring of risk factors.
Stages of myocardial infarction
If a person does not notice the manifestations of a pre-infarction condition, the heart attack itself develops. The medical community has created the following list of stages of the disease, which successively replace each other:
- The sharpest. Lasts about 6 hours. Often the patient does not have time to be transported for treatment;
- Spicy. Considered the most dangerous. Lasts about two weeks, which allows a scar to form on the heart muscle;
- Subacute – characterized by the gradual disappearance of necrosis;
- Post-infarction – begins from the second month from the onset of the disease. Its duration is directly related to the lesion;
- The scarring stage ends the course of the disease, but does not mean that the person is completely and irrevocably cured.
Rehabilitation and recovery after a heart attack
The main tasks of rehabilitation after a heart attack are the restoration of the circulatory system, ability to work and a normal lifestyle. Rehabilitation includes a set of measures, consistently and continuously carried out under the supervision of doctors.
Rehabilitation measures are individual and depend on the patient’s condition, the severity of the heart attack, and chronic diseases. At the same time, the stages of rehabilitation are associated with being in a hospital, in a sanatorium and at home.
In the hospital, the disease is diagnosed, treatment is carried out after restoration of the patency of the coronary vessels, risks are assessed and a prognosis for the recovery period and relapse is formed.
The inpatient rehabilitation period is the time of the acute period of a heart attack, which the patient spends in a specialized rehabilitation department of the hospital and then in a cardiological sanatorium.
An outpatient rehabilitation period is provided for home conditions under the supervision of a cardiologist and exercise therapy doctor.
Rehabilitation is medicinal and non-medicinal methods of recovery. These include:
- gymnastics to prevent the formation of repeated blood clots and increase blood supply and oxygen supply,
- physiotherapy,
- psychological help.
At the same time, an individual set of measures includes a gradual increase in physical activity. Typically, two weeks after a heart attack, patients are allowed to walk up to 2 km per day, assessing the ability of the heart to work using echocardiography (ultrasound examination of the heart), and performing exercise tests.
The exercise therapy complex gradually includes swimming, walking at a pace, and training on exercise machines. Depending on the functional class of ischemia, classes are held in a training or gentle mode.
During rehabilitation, measures of psychological recovery are important. Returning to normal life and overcoming fear, including before physical activity, is an important stage of recovery after a heart attack. The formation of depressive and anxiety states can delay the results of rehabilitation for a long time and worsen its quality.
Non-drug methods, in addition to physical rehabilitation, include lifestyle correction:
- quitting smoking and alcohol,
- diet,
- full sleep.
Medicines are used for:
- preventing angina attacks,
- blood pressure control,
- blood clotting,
- lipid metabolism,
- treatment of arrhythmia and chronic heart failure.
A comprehensive rehabilitation program helps patients recover in a shorter time and prevent recurrent heart attacks and other complications.
How does an atypical heart attack occur?
In addition to the usual course of the disease, which occurs in most cases, medicine also knows atypical variants of pathogenesis. For example, such as:
- Asthmatic. Typical for older people, the pain syndrome is mild, but the heartbeat is rapid, shortness of breath is observed, and the pulse is increased;
- Gastralgic. With this option, there is pain in the upper abdomen, belching, hiccups, vomiting are observed, and the abdomen is swollen. ;
- Arrhythmic. The heartbeat is abnormal, but the pain is minor. The percentage of patients with arrhythmic infarction is up to 5%;
- Cerebrovascular is characterized by a person’s disorientation in space, loss of consciousness and vomiting occur;
- Asymptomatic - practically does not make itself felt. As a rule, it is discovered when a patient is prescribed an ECG for preventive purposes.
However, doctors warn that only the first, most acute period is atypical. Then the disease takes its toll and the picture will be the same as with the normal course of a heart attack.
HELP OF THE SAMAZDRAV RESPIRATORY SIMULATOR IN REHABILITATION
To quickly return to a normal lifestyle, you can use the Samozdrav breathing simulator. Regular exercises on this device will improve blood supply to the heart. It can be especially useful for that group of patients who undergo rehabilitation at home.
You can start training on the simulator within 3 months after a heart attack. The Samozdrav simulator is useful both for the rehabilitation of the patient and for the prevention of a recurrent heart attack. After all, with the help of a hypercapnic mixture, vascular spasm is relieved and the functioning of the entire cardiovascular system is improved.
Due to constant training, a system of collaterals is formed - small blood vessels around the heart. They provide alternative blood supply and more complete nutrition of the heart muscle.
By exercising on the Samozdrav simulator, the patient will recover faster after a heart attack, because blood flow is normalized and the load is removed from the coronary vessels. Classes on the Samozdrav simulator will give tangible results within 3-4 months, and for such a serious illness as a heart attack this period is quite short.
Disability after a heart attack
A heart attack requires a long period of treatment and rehabilitation. At the same time, a person’s full working capacity is not always restored. For these reasons, permanent or temporary disability is given to patients with a heart attack quite often.
All patients who have suffered a major heart attack have the right to four months of paid rehabilitation based on the compulsory medical insurance policy. Usually this period of rehabilitation is enough to understand whether a person needs a disability or whether he is able to fully begin his usual work. If there is reason to think about partial loss of ability to work, the patient, on the recommendation of the attending physician, can undergo an examination by a medical and social expert commission.
To assess the level of disability, the commission will assess:
- patient self-care options,
- his education,
- possibility of returning to normal work,
- general health.
As a result, disability may be assigned to those whose work involves frequent stress, increased attention, and physical activity; pensioners and patients who have undergone vascular surgery; people with heart failure or unstable angina, as well as those who have lost their ability to work by 50 percent or more.
The commission evaluates each case individually and makes a decision based on a combination of factors both on the fact of establishing disability and on its group.
Diet
In the first week after myocardial infarction, a low-calorie diet with limited fluid, salt, fat, excessive fiber and cholesterol is recommended. The diet should include foods rich in potassium and vitamin C.
In the first week, food is served pureed, in small portions 6-7 times a day. It can be:
- semolina,
- oatmeal,
- buckwheat,
- rice porridge,
- lean veal,
- chicken,
- fish,
- steamed white omelette,
- cottage cheese and kefir,
- carrot and apple salad,
- beets and cabbage,
- fruit purees,
- honey.
You can't eat:
- baked goods and sweets,
- smoked,
- fried,
- fatty,
- spicy,
- salted and pickled dishes;
- pasta,
- beans,
- coffee,
- boiled and fried eggs.
After the acute period, whole foods are introduced into the diet, but dietary restrictions should become the norm for a person.
The basis of the diet should be:
- vegetables,
- fruits,
- nuts,
- lean meats and fish,
- cereals
Smoked, canned, fried and salted foods are not recommended for consumption. It is convenient to control your weight using your body mass index (the result of dividing your weight in kg and height in meters squared).
It should be within 25-27 kg/m. In addition, the waist circumference is assessed: for men this figure should not exceed 94 cm, for women – 80 cm.
Diet for weight loss
First breakfast.
One hundred grams of low-fat cottage cheese, a cup of coffee with milk and without sugar.
Lunch.
Fresh cabbage salad (170 g) with sour cream without salt.
Dinner.
Vegetarian cabbage soup (200 ml), 90 g lean boiled meat, 50 g green peas, 100 g apples.
Afternoon snack.
One hundred grams of cottage cheese and 180 ml of rosehip decoction.
Dinner.
Boiled fish (100 g) and vegetable stew (125 g).
Before going to bed, at night.
Kefir (180 ml) and 150 g of rye bread.
Let us repeat, this is an approximate diet for one day. This diet contains 1800 kcal.
For patients without excess weight problems, the diet is significantly expanded.
They are prescribed a diet with a calorie content of 2500 - 3000 kcal
. The consumption of animal fats and carbohydrates is limited. Also 4-5 meals a day. It is useful to spend fasting days on apples (1.5 kg) or fresh cucumbers (2 kg). For “avid meat eaters”, 600 g of lean meat plus a side dish of vegetables (fresh cabbage, green peas) are even allowed.
Strongly not recommended
Doctors do not allow such patients to drink
alcohol
, even of the highest quality. It causes tachycardia and an undesirable increase in appetite. The consumption of smoked meats, fried foods, fatty sausages and sweets is absolutely unacceptable.
Breathing exercises after a heart attack
A heart attack is an acute condition associated with extreme strain on blood vessels and extreme circulatory impairment. Lack of oxygen in the heart muscle leads to its death. Unfortunately, necrosis of the heart muscle is irreversible, but nevertheless, it is necessary to create conditions for sufficient oxygen in the body for both primary and secondary prevention of the disease.
Acute pain during angina attacks, which are precursors to a heart attack, signals the myocardium about problems with oxygen.
The surest way to provide the heart muscle with enough oxygen is to reduce risk factors and breathe properly. We receive oxygen through the respiratory organs, and they must be trained and tuned to support a full respiratory cycle.
The Samozdrav breathing simulator can become a confident and powerful support in the prevention of heart attack. One of the basic positive effects of breathing training on the body is sufficient oxygen supply to the body and maintenance of normal CO2 levels. Thanks to training with Samozdrav, you can constantly maintain oxygen levels at a level that eliminates oxygen deficiency. This means a high probability of myocardial preservation and significantly reduces the risk of heart attack.
In addition to the “direct supply” of oxygen to the body, breathing training strengthens the functioning of the nervous system and corrects reactions to stress, providing peace and a smooth emotional background even under high loads.
Training with Samozdrav corrects metabolism and is effective in treating obesity. They activate metabolism by normalizing the level of oxygen in cells and tissues, normalize the excretion of metabolic products, and allow for better absorption of nutrients.
Samozdrav is indispensable for patients with hypertension. It was the treatment of this disease that became the primary goal of the creators of the breathing simulator, and today its effectiveness in treating hypertension without medications has been fully proven by research and many years of practice of use by millions of people.
Breathing training can cope with any modified risk factor for heart attack. Regular exercise will give the myocardium sufficient oxygen levels and keep the heart healthy.
Diagnosis of heart attack
To make an appropriate diagnosis, it is necessary to question the patient and, if he complains of pain in the chest area, be sure to send him for an ECG. In case of a heart attack, the cardiogram will show a T- or Q-wave, QRS pathology. Only a specialized specialist can understand this. You will also need to take a blood test. In case of a heart attack it is very indicative. 6 hours after the attack, increased myoglobin will be detected, after 10 - creatine phosphokinase, after a day or two - an increased level of lactate dehydrogenase. ESR, AlAt, leukocyte count, and AsAt will also increase. One of the innovations in the diagnosis of heart attack is the troponin test. This express method helps detect a heart attack within an hour. A healthy person does not have troponins in the blood, but in case of a heart attack they will be present. By the way, this is one of the “folk” ways to distinguish angina from a heart attack. Most likely, it will not be possible to do without coronography, which will show how the ventricles contract, whether there are blood clots, and determine the possibility and need for bypass surgery.
Acute myocardial injury due to coronavirus disease 2021 (COVID-19) (case study)
- Babaev Maxim Alexandrovich
- Petrushin M.A.
- Dubrovin I.A.
- Kostritsa N.S.
- Eremenko Alexander Anatolievich
Summary
COronaVIrus Disease 2021 in 20% of cases is characterized by a severe and very severe course, which is accompanied by pneumonia, acute respiratory distress syndrome, and multiple organ dysfunctions. Complications from the cardiovascular system occur in 20-25% of cases and, alone or together with respiratory failure, cause deaths in 40% of patients with an unfavorable course of the disease. Acute myocardial damage (5-38%), which is most often caused by a combination of factors: infarction against the background of acute viral myocarditis and “cytokine storm”; thrombosis of coronary vessels due to covid-associated coagulopathy; vasoconstriction due to blocking of SARS-COV-2 receptors of angiotensin-converting enzyme II (ACE II) and an increase in the concentration of angiotensin II; hypoxia due to respiratory failure, manifested by heart failure, cardiac arrhythmias (~20%) and/or cases of sudden death (5-7%).
This clinical case demonstrates how a patient at particular risk (hypertension), despite positive dynamics, after therapy with human monoclonal antibodies to the interleukin-6 receptor (sarilumab), on the 8th day of her stay in the intensive care unit sudden death occurred with circulatory arrest, the cause of which was acute myocardial injury.
Key words: coronavirus, COVID-19, acute myocardial injury, multiple organ dysfunctions
Financing
.
The study had no sponsorship. Conflict of interest
.
The authors declare no conflict of interest. For citation
: Babaev M.A., Petrushin M.A., Dubrovin I.A., Kostritsa N.S., Eremenko A.A. Acute myocardial injury during coronavirus disease 2021 (COVID-19) (clinical case analysis) // Clinical and experimental surgery. Journal named after academician B.V. Petrovsky. 2021. T. 8, No. 3. P. 87-94. DOI: https://doi.org/10.33029/2308-1198-2020-8-3-87-94
COVID 19 (COronaVIrus Disease 2019) is a viral infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) with a mortality rate of 3-7% [1]. The disease has a 7-14-day incubation period and is more common in males with reduced body reserves (age, comorbidity). The disease has a heterogeneous clinical course, depending on the severity of the systemic process, the endotype and/or combination of endotypes of the generalized response to the introduction of the virus (hyperinflammation, coagulation disorders, immunosuppression) and the amount of damage to the vascular endothelium and epithelial tissues [2, 3]. With an adaptive response, the appearance of individual symptoms or generally asymptomatic carriage is possible. In 20% of cases, a severe and very severe course is observed, which is accompanied by pneumonia, acute respiratory distress syndrome (ARDS), multiple organ dysfunctions, the addition of a bacterial infection and ends with multiple organ failure [2].
In addition to pulmonary complications, the most common complications are those of the cardiovascular system (CVS), which alone or together with respiratory failure cause deaths in 40% of patients with an unfavorable course of the disease. With COVID-19, patients with a history of cardiovascular disease (CVD) and hypertension are more likely to require intensive care [odds ratio (OR) 2.1; confidence interval (CI) 1.5-3.0; OK: 1.9, CI 1.5-2.5)] and have an increased risk of mortality (OR 4.7; CI 2.9-7.b) [4]. Complications from the cardiovascular system manifest themselves in the form of acute heart failure (AHF) and venous thromboembolism. Heart damage is detected in 20-25% of severe patients with COVID-19 [2]. Acute myocardial injury is a consequence of ischemic (acute coronary syndrome, ACS)/non-ischemic (myocarditis)/mixed causes (arrhythmias), manifested by increased levels of troponin and type B natriuretic peptides, and is associated with an increased risk of developing ARDS, malignant ventricular tachyarrhythmias, acute kidney injury and coagulopathy, the risk of death, and this risk is greater in patients with existing cardiovascular diseases [5, b].
This article presents an analysis of risk factors, causes of occurrence and course of COVID-19, complicated by acute myocardial injury.
Clinical case
Patient Z.,
Born in 1958, she was admitted on May 30, 2020 to the pulmonology department (for the treatment of patients with diagnosed COVID-19) of the Regional Clinical Hospital of Tver with a diagnosis of “bilateral community-acquired pneumonia (covid-pneumonia?).”
She considers herself sick since 05/23/2020, when general weakness appeared, after 2 days she turned to her local physician for help, after which she was prescribed levofloxacin, and from 05/26/2020 ceftriaxone was added to the treatment. On May 29, 2020, a multislice computed tomography (MSCT) of the chest was performed, which revealed bilateral moderate pneumonia with damage to 25-50% of the lung parenchyma, areas of compaction of the “ground glass” type (CT2 - classification according to the degree of detected changes). She did not seek inpatient care. On May 30, 2020, due to deterioration of her condition (hyperthermia up to 38.6 °C, refractory to therapy, weakness), she called an ambulance. History: stage II hypertension, stage II arterial hypertension, risk 2.
Upon admission, PCR analysis detected Covid-19 RNA; on the electrocardiogram (ECG) atrioventricular (AV) block of the first degree, corrected QT
— 413 ms; in a biochemical blood test: an increase in the level of aspartate aminotransferase (AST) - up to 111 units/l with the level of alanine aminotransferase (ALT) - 31 units/l, γ-glutamyl transpeptidase (GGT) - up to 988 units/l, serum creatinine - 134 µmol/l.
After additional studies, the patient was diagnosed with coronavirus infection caused by the COVID-19 virus, the virus was identified (U07.1); community-acquired bilateral polysegmental pneumonia (J18.8); multiple organ dysfunctions (moderate acute respiratory distress syndrome, ARDS); acute myocardial injury; acute kidney injury, AKI) and concomitant diseases in the form of stage II hypertension, stage II arterial hypertension, risk 2.
By the 3rd day of hospital stay (11th day from the onset of the disease), the patient’s condition worsened (Fig. 1):
• therapy-resistant hyperthermia up to 38.7 °C persisted; an increase in the level of C-reactive protein to 85 mg/l, ferritin was detected, the content of presepsin corresponded to a moderate risk of developing systemic inflammation (487 pg/ml); there was a high tendency to microthrombosis (D-dimer, lactate dehydrogenase, LDH);
• laboratory signs of myocardial damage (troponin I) and overload of the heart cavities (NT-proBNP) were recorded; according to echocardiography (EchoCG) diastolic dysfunction of the left ventricle (LV) of the first degree (slow relaxation), a tendency to dilatation of the left atrium, signs of pulmonary hypertension (average pressure in the pulmonary artery - 25 mm Hg);
• hypoperfusion with the appearance in the analysis of acid-base status (ABS) - metabolic (4 mmol/l) lactic acidosis (pH - 7.20, BE - 16 mmol/l);
• progression of respiratory failure - decrease in SatO2 level to 86% (by pulse oximeter) when breathing atmospheric air, the appearance of tachypoea up to 26/min, on control computed tomography (CT) diffuse thickening of the lung tissue like “ground glass”, consolidation in combination with reticular changes, significant distribution of the volume of lung damage 96% (CT4).
Rice. 1.
Clinical and laboratory characteristics of the course of the disease in patient Z.
SOFA - sepsis-associated organ dysfunction scale; TnI—troponin I; PEEP - positive end-inspiratory pressure; CPAP - continuous positive airway pressure; NT-proBNP - N-terminal propeptide of natriuretic hormone; CT - computed tomography; RR - respiratory rate; FIO2—fraction of oxygen in inspired air; prone position - prone position; AST—aspartate aminotransferase; ALT - alanine aminotransferase.
Fig. 1.
Clinical and laboratory characteristics of the course of the disease in patient Z.
SOFA—scale of organ dysfunction associated with sepsis; TnI—troponin I; PEEP is the positive pressure of the end of the dose; CPAP - continuous positive airway pressure; NT-proBNP - N-terminal propeptide of natriuretic hormone; CT - computed tomography; RR—respiratory rate; FIO2 - fraction of oxygen in the inhaled air; prone position - prone position; AST—aspartate aminotransferase; ALT - alanine aminotransferase.
The patient was transferred to the intensive care unit (ICU), where she was started on non-invasive pulmonary ventilation (NIV) in CPAP mode with PEEP 8 cm H2O. and fraction of inhaled oxygen (FiO2) 50% with periodic sessions of prone position for 6-10 hours, correction of CBS and water-electrolyte balance, a change in antibiotic therapy was carried out, targeted therapy for the “cytokine storm” was started with the IL-6 antagonist drug sarulumab.
By the 7th day of stay in the ICU (18th day from the onset of the disease), it was possible to stop the hyperthermia, the patient began to notice a subjective improvement in well-being, which was accompanied by a decrease in the volume of the lesion to 86% according to CT data, with stabilization of the SatO2 indicator at 96% during inhalation 40% oxygen.
However, blood tests showed progressive signs of inflammation (leukocytosis - 25.5x109/l, segmented neutrophils - 80.5%), thrombotic microangiopathy (LDH increase almost 2 times), acute hepatic-renal dysfunction (cholestasis, cytolysis, increase in creatinine) and myocardial damage (increased levels of high-sensitivity troponin I and NT-proBNP), which was accompanied by an increase in the corrected QT
up to 420 ms, diffuse hypokinesia of the LV myocardium without local contractility disorders; reduction in ejection fraction up to 46%; LV diastolic dysfunction of the first degree. Also, echocardiography visualized LV hypertrophy, signs of chronic pulmonary heart disease (dysfunction and overload of the right sections against the background of arterial pulmonary hypertension, right ventricular hypertrophy); secondary tricuspid insufficiency degree II; left atrium dilatation; atherosclerosis of the aorta, grade I-II calcification of the aortic valve leaflets, grade I aortic regurgitation.
On June 11, 2020, the patient’s condition worsened sharply. The patient lost consciousness, did not respond to painful stimuli (Glasgow Coma Scale - 6 points), asystole was recorded on the ECG. The patient was intubated, transferred to mechanical ventilation, and full resuscitation measures were carried out, which turned out to be ineffective.
Results of pathological examination
The macropreparation is shown in Fig. 2.
Rice. 2.
Macroscopic specimen of the heart of patient Z.
Heart weighing 340 g, size 11x9x7 cm. Left ventricular wall thickness 1.5 cm, right 0.3 cm, interventricular septum thickness 1.3 cm; coronary arteries are patent. Noticeable enlargement of the right side of the heart. The heart muscle on sections is pale red, under the endocardium of the anterior wall of the left ventricle and the interventricular septum there is a hemorrhage of 5x4 cm. The pulmonary arteries are passable freely, the intima is smooth, shiny
Fig. 2.
Macrodrug of the heart of a patient Z.
Heart weighing 340 grams, size 11x9x7 cm. LV wait thickness 1.5 cm, right 0.3 cm, interventricular septum thickness 1.3 cm; coronary arteries are passable. Marked expansion of the right heart. The muscle of the heart on the incisions is pale red, under the endocardium of the anterior wall of the left ventricle and interventricular septum there is a 5×4 cm hemorrhage. The pulmonary arteries are freely passable, the intima is smooth, shiny
Discussion
This clinical example confirms the data of numerous studies that COVID-19 aggravates the course of existing CVDs and leads to the development of new ones; the addition of acute myocardial injury leads to a pronounced worsening of the disease, contributes to the occurrence of multiple organ dysfunctions and is a significant risk factor for an unfavorable outcome, despite the therapy; the presence of acute myocardial damage can cause sudden circulatory arrest.
The incidence of COVID-19 complications from the cardiovascular system, according to various authors, ranges from 5 to 38% among hospitalized patients [4, 7, 8].
Complications manifest themselves in the form of acute heart failure (ACS, myocarditis, arrhythmias) and venous thromboembolism. Complications of CVS in COVID-19 are closely related to existing heart and vascular diseases, especially hypertension (23.3%) [4]. The reasons for this relationship remain to be determined. The medical history of patient Z. clearly shows that this risk factor (stage II hypertension, stage II arterial hypertension, risk 2), even without coronary heart disease and severe atherosclerosis in a woman under 65 years of age, can become a significant cause of the development of damage to the heart muscle and progression of cardiac dysfunction in COVID-19.
The literature notes that cardiovascular complications diagnosed upon admission to the hospital in 41.3% lead to a severe course of the disease and rapid transfer to the ICU [4]. In our case, this happened on the 3rd day from the moment of admission.
The causes of AHF and venous embolic complications are quite well understood, since they are a direct consequence of the main cardiovascular complications that develop during COVID-19 (ACS, myocarditis, arrhythmias, hypercoagulation, vasospasm). At the same time, the pathogenesis of acute myocardial injury is quite difficult to differentiate, since the mechanisms underlying it are of a mixed ischemic and non-ischemic nature.
The pathogenesis of cardiac injury includes vasoconstriction [due to increased angiotensin II concentrations following SARS-COV-2 blockade of angiotensin-converting enzyme II (ACE II) receptors]; impaired oxygen delivery and consumption due to respiratory failure; myocardial infarction (types 1 and 2) against the background of acute viral myocarditis and “cytokine storm”; thrombosis due to Covid-associated coagulopathy [9] (see Fig. 2).
The pathogenesis and microscopic picture of COVID-19 in patient Z. with acute myocardial injury are presented in Fig. 3.
Rice. 3.
Pathogenesis and microscopic picture of COVID-19 acute myocardial injury: 1. Fragmentation, discoid and block decomposition of myocardiocytes; 2. Necrosis of groups of myocardiocytes (absence of nuclei in cardiomyocytes). The zone of necrosis is delimited from the preserved myocardium by a zone of plethora and leukocyte infiltration (demarcation inflammation); 3. Wave-like deformation of cardiomyocytes (cause of fibrillation); 4. Arteriole thrombus; 5. Congestion, hemorrhages, stagnation of leukocytes in capillaries with access to interstitial spaces (necrosis lasts about 1 day); 6. Blocky decomposition of cardiomyocytes
Fig. 3.
Pathogenesis and microscopic picture in acute covoid myocardial damage
(hematoxylin and eosin, X100).
1. Fragmentation, discoid and blocky decomposition of myocardiocytes; 2. Necrosis of myocardiocyte groups (lack of nuclei in cardio-myocytes). The area of necrosis is delimited from the preserved myocardium by the zone of plethora and leukocyte infiltration (demarcation inflammation); 3. Wave-like deformation of cardiomyocytes (the cause of fibrillation); 4. Arterioles thrombus; 5. Plethora, hemorrhages, stasis of leukocytes in the capillaries with access to interstitial spaces (necrosis lasts about 1 day); 6. Blocky decomposition of cardiomyocytes
An important role in the pathogenesis of myocardial damage is played by the effect of SARS-CoV-2 on ACE II receptors [10]. The virus directly binds to ACE II and leads to a decrease in its expression. Thus, under the influence of the virus, the concentration of angiotensin II increases and the concentration of angiotensin 1-7, which has cardioprotective properties, decreases [10]. Angiotensin II, in turn, has a vasoconstrictor and proatherosclerotic effect [11]. In addition, the expression of TNF-α is increased, increasing the local and systemic inflammatory response and promoting further myocardial damage [12]. These effects can be both local and systemic in nature. Direct entry of the virus into cells can also lead to necrosis of cardiomyocytes and ultimately to myocardial damage [13].
In COVID-19, a “cytokine storm” caused by an uncontrolled and dysfunctional immune response by T helper cells 1 and 2 leads to the continuous activation and proliferation of various cytokines that cause apoptosis and necrosis of myocardial cells, and also predispose to plaque rupture [10].
Respiratory failure and generalized inflammation lead to a mismatch between oxygen consumption and delivery to tissues, causing hypoxia, which promotes excessive intracellular calcium deposition, leading to myocardial cell apoptosis and damage [11].
With COVID-19, an increase in the frequency of arterial thrombosis is recorded, causing strokes, ACS and episodes of sudden death. The pathogenesis of these thrombotic complications is multifactorial and repeats elements of known coagulation disorders (sepsis-induced coagulopathy, disseminated intravascular coagulation, hemaphagocytic syndrome and hemaphagocytic lymphohistiocytosis, antiphospholipid syndrome, thrombotic microangiopathy, thrombotic thrombocytopenic purpura, hemolytic uremic syndrome, heparin-induced thrombocytopenia) [14] .
Acute myocardial injury is characterized by an increase and/or decrease in the concentration of markers of myocardial damage: cardiac troponin (cTnI/cTnT) above/below the 99th percentile in the absence of clinical signs of myocardial ischemia may be accompanied by an increase in the level of B-type natriuretic peptide (BNP) or N-terminal fragment brain natriuretic peptide (NT-proBNP) [15].
With COVID-19, 2 types of myocardial damage can be suspected: primary or secondary. With primary injury, patients predominantly present with cardiac rather than respiratory complaints. The cause of the primary injury may be acute myocardial infarction (type 1), viral myocarditis, or stress-induced cardiomyopathy. Patients complain of chest pain, tests reveal elevated cardiac enzymes, and echocardiography reveals LV dysfunction and changes associated with the ST-T
on the ECG, but with normal patency of the coronary vessels on the angiogram [10].
Secondary damage is associated with direct damage to cardiomyocytes by the virus, generalized inflammation, expressed by a tendency to increase cTnI in parallel with an increase in inflammatory biomarkers (interleukin-b, D-dimer, ferritin and LDH). F. Zhou et al. [16] showed that the incidence of cTnI elevation was significantly higher among non-survivors and was a predictor of in-hospital death (odds ratio 80.07; 95% CI 10.34–620.36; p
<0.0001) [3]. The results [17, 18] noted a dynamic increase in cTnI in the group of non-survivors, with the most dramatic increase in its concentration after the 16th day from the onset of the disease and the maximum value on the 22nd day. Notably, the median time to death from symptom onset was 18.5 days (interquartile range, range 15–20 days). Similarly, the level of NT-proBNP >88.64 pc/ml in patients with severe COVID-19 is an independent factor that increases in-hospital mortality [19].
From the moment of admission to the hospital, patient Z. already showed signs of myocardial damage: increased levels of cTnI and NT-proBNP, serum transaminases, cardiac cavities, signs of pulmonary hypertension. Changes in laboratory parameters were not accompanied by characteristic complaints, there was no anamnestic information about the presence of ischemic disease, and no changes of ischemic origin were recorded on the ECG. One day before the onset of an unfavorable outcome (8th day in the ICU and 19th from the onset of the disease; this time period coincides with the data presented in the work of G. Lippi et al. [17]) an increase in the levels of cTnI and NT-proBNP was noted - almost 1.5 times from the initial values and a slight decrease in the LV ejection fraction on EchoCG, an increase in the characteristic indicators of microthrombosis and progression of the severity of organ dysfunction against this background. Clinical and laboratory characteristics are confirmed by the results of an autopsy, which revealed characteristic pathological changes in the macroanatomy of the heart (weight, size, wall thickness, presence of hemorrhage in the interventricular septum) and the structure of cardiomyocytes (fragmentation, edema, decay of cardiomyocytes). The protocol noted the appearance of a fresh area of myocardial necrosis (one day before the onset of death) with an area of perifocal inflammation and thrombus in the lumen of the arteriole, which coincided with the obtained laboratory parameters. It was possible to record a section of the myocardium with wave-like deformations of cardiomyocytes, which could be the morphological cause of the development of rhythm disturbances and sudden death [20].
Cardiac arrhythmias occur in 7-17% of cases in patients with COVID-19 and are detected significantly more often in those who require intensive care (44.4 vs. 6.9%, p
<0.001) [5, 6].
The pathogenesis of arrhythmias includes ischemia and myocardial damage caused by viral infection, hypoxia, fever, metabolic disorders, neurohormonal dysregulation and inflammatory stress, and the use of drugs that cause prolongation of the QT period (
chloroquine, hydroxychloroquine, azithromycin) [21]. It is typical that the risk of arrhythmias is greater in patients with previously diagnosed CVD. According to the literature, an increase in troponin levels along with the appearance of arrhythmia may indicate the addition of fulminant myocarditis [13].
Cases of sudden cardiac death have also been described in patients with COVID-19 [22], which can be caused by any of the cardiovascular complications described above.
Thus, in the presented clinical case, the risk factor for the development of complications from the cardiovascular system was hypertension; the cause of acute myocardial damage was ischemic and non-ischemic effects characteristic of the pathogenesis of COVID-19 (generalized inflammation, myocarditis, myocardial ischemia, microthrombosis). Acute myocardial injury was characterized by elevated levels of cardiac enzymes, echocardiographic abnormalities and was clinically expressed in the progression of organ disorders (acute renal and hepatic dysfunction), AHF and sudden cessation of hemodynamics against the background of cardiac arrhythmias. Morphological and histological confirmation of organ structure disorders and suspected causes of death in a patient with COVID-19 was obtained.
Conclusion
In the context of the current threat of a pandemic of a new coronavirus disease, patients with underlying cardiovascular pathology represent a special risk group with high rates of adverse outcomes. Complications from the cardiovascular system significantly worsen the severity of COVID-19, are closely associated with the development of multiple organ dysfunctions and are the main cause of adverse outcomes. Even a slight but persistent increase in the level of high-sensitivity troponin I and the enzyme NT-proBNP can serve as a warning signal of myocardial damage associated with direct viral effects on cardiomyocytes or with cardiomyopathy or infarction that arose during the generalized response of the body and the course of COVID-19-associated pathologies processes. The greatest danger is caused by rhythm and conduction disturbances that occur when the heart is damaged, which can be a harbinger of cases of sudden death.
Literature
1. World Health Organization, Coronavirus disease 2019 (COVID-19): situation report, 121. 2021. P. 19.
2. Madjid M. et al. Potential effects of coronaviruses on the cardiovascular system: a review // JAMA Cardiol. 2021 Mar 27.
3. Russian Cardiological Society. Guidelines for the diagnosis and treatment of diseases of the circulatory system in the context of the CO-VID-19 pandemic // Russian Journal of Cardiology. 2021. T. 25. No. 3. P. 1-20.
4. Zadori N. et al. The negative impact of comorbidities on the disease course of COVID-19 // Intensive Care Med. 2021. P. 1-3.
5. Gopinathannair R. et al. COVID-19 and cardiac arrhythmias: a global perspective on arrhythmia characteristics and management strategies // J. Interv. Card. Electrophysiol. 2021. P. 1-8.
6. Liu K. et al. Clinical characteristics of novel coronavirus cases in tertiary hospitals in Hubei Province // Chin. Med. J. (Engl.). 2021. Vol. 133, N 9. P. 1025-1031.
7. Guo T. et al. Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2021 (COVID-19) // JAMA Cardiol. 2021 Mar.
8. Shi S. et al. Association of cardiac injury with mortality in hospitalized patients with COVID-19 in Wuhan, China // JAMA Cardiol. 2021. Vol. 5, N 7. P. 802-810.
9. Al Jaroudi WA, Hage FG Cardiovascular disease in the literature: a selection of recent original research papers // J. Nucl. Cardiol. 2021. Vol. 27, N 3. P. 712-714.
10. Tersalvi G. et al. Elevated troponin in patients with coronavirus disease 2021: possible mechanism // J. Card. Fail. 2020. Vol. 26, N 6. P. 470-475.
11. Mahajan K., Chandra KS Cardiovascular comorbidities and complications associated with coronavirus disease 2021 // Med. J. Armed Forces India. 2021 May.
12. Babapoor-Farrokhran S. et al. Myocardial injury and COVID-19: possible mechanisms // Life Sci. 2021. Vol. 253. Article ID 117723.
13. Driggin E. et al. Cardiovascular considerations for patients, health care workers, and health systems during the COVID-19 pandemic // J. Am. Coll. Cardiol. 2021. Vol. 75, N 18. P. 2352-2371.
14. Iba T. et al. The unique characteristics of COVID-19 coagulopathy // Crit. Care. 2021. Vol. 24, N 1. P. 360.
15. Huang C. et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China // Lancet. 2021. Vol. 395, N 10 223. P. 497-506.
16. Zhou F. et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study // Lancet. 2021. Vol. 395, N 10 229. P. 1054-1062.
17. Lippi G., Lavie CJ, Sanchis-Gomar F. Cardiac troponin I in patients with coronavirus disease 2021 (CO-VID-19): evidence from a meta-analysis // Prog. Cardiovasc. Dis. 2021 Mar.
18. Krittanawong C. et al. Coronavirus disease 2021 (COVID-19) and cardiovascular risk: a meta-analysis // Prog. Cardiovasc. Dis. 2020. Vol. 63, N 3. P. 390391.
19. Gao L. et al. Prognostic value of NT-proBNP in patients with severe COVID-19 // Respir. Res. 2021. Vol. 21, N 1. P. 83.
20. Smirnov V.P., Panysheva I.A. Pathomorphology of cardiomyocytes in sudden cardiac death // Medicine: challenges of today: materials of the III International Scientific Conference. Moscow: Buki-Vedi, 2021. pp. 43-46.
21. Kochi AN et al. Cardiac and arrhythmic complications in patients with COVID-19 // J. Cardiovasc. Electrophysiol. 2021. Vol. 31, N 5. P. 1003-1008.
22. Marijon E. et al. Out-of-hospital cardiac arrest during the COVID-19 pandemic in Paris, France: a population-based, observational study // Lancet Public Health. 2021. Vol. 5, N 8. P. e437-e443.