Diagnosis and treatment of patients with cardiac syndrome X
About the article
17732
0
Regular issues of "RMZh" No. 14 dated June 26, 2009 p. 903
Category: Cardiology
Authors: Lupanov V.P. , Dotsenko Yu.V.
For quotation:
Lupanov V.P., Dotsenko Yu.V. Diagnosis and treatment of patients with cardiac syndrome X. Breast cancer. 2009;14:903.
Epidemiology Approximately 10–20% of patients undergoing diagnostic coronary angiography for acute or chronic cardiac ischemic syndrome have intact coronary arteries. Even if we assume that in some of them the symptoms of ischemia may be due to other cardiac and non-cardiac causes, then at least one out of ten patients with typical angina pectoris does not have hemodynamically significant stenoses of the coronary arteries.
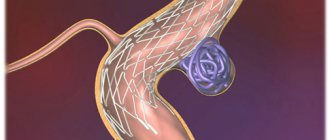
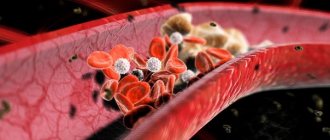
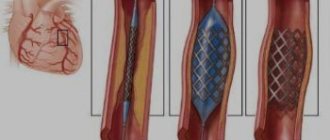
Epidemiology Approximately 10–20% of patients undergoing diagnostic coronary angiography for acute or chronic cardiac ischemic syndrome have intact coronary arteries. Even if we assume that in some of them the symptoms of ischemia may be due to other cardiac and non-cardiac causes, then at least one out of ten patients with typical angina pectoris does not have hemodynamically significant stenoses of the coronary arteries. Definition The presence of typical angina with unchanged coronary arteries was first described by N. Kemp in 1973 [1]. This syndrome is called "syndrome X". Syndrome X is diagnosed in patients with typical chest pain, positive stress tests, angiographically normal epicardial coronary arteries, and no clinical or angiographic evidence of coronary artery spasm. In addition, patients should not have systemic arterial hypertension with or without left ventricular hypertrophy, as well as disturbances in left ventricular systolic function at rest. During exercise, systolic function may be normal or slightly altered. Quite rarely, patients with syndrome X develop blockade of the left bundle branch with the subsequent development of dilated cardiomyopathy. Although most patients with typical chest pain on exercise and a positive stress test usually have overt (obstructive) coronary artery disease, especially when underlying risk factors are identified, approximately 10–20% of them have normal coronary angiograms [2]. These patients are classified as cardiac (cardiac) syndrome X, for which there is no universal definition. In the absence of changes in the coronary arteries during angiography, there is often occlusive pathology of the distal vessels (microvascular angina) [3]. Some authors use the term “microvascular angina,” meaning that patients with typical angina have a normal coronary angiogram and reduced coronary reserve. Syndrome X is usually classified as one of the clinical forms of coronary artery disease, since the concept of “myocardial ischemia” includes all cases of imbalance in oxygen supply and myocardial demand for it, regardless of the reasons causing it. It should be noted that the capabilities of the angiography method in assessing the state of the coronary bed, in particular microvascular, are limited. Therefore, the concept of “angiographically unchanged coronary arteries” is very arbitrary and indicates only the absence of atherosclerotic plaques narrowing the lumen of the vessels in the epicardial coronary arteries. The anatomical features of the small coronary arteries remain “angiographically invisible.” Syndrome X includes various groups of patients, among them, apparently, women in menopause predominate. A significant proportion of patients, especially women who undergo coronary angiography to clarify the cause of chest pain, do not have significant changes in the coronary arteries. In such cases, the characteristics of the pain allow us to consider 3 possibilities: 1) non-anginal pain; 2) atypical angina, including vasospastic; 3) cardiac (cardiac) syndrome X. Positive results of stress tests are observed in 10–20% of individuals with normal coronary arteries and complaints of chest pain [4]. These are usually patients aged 30–45 years, more often women, usually without risk factors for atherosclerosis and with normal left ventricular function. Etiology and pathogenesis The etiology of syndrome X remains unclear. Until now, only some pathophysiological mechanisms have been established that lead to the development of typical clinical and instrumental manifestations of the disease: increased sympathetic activation, endothelial dysfunction, structural changes at the level of microcirculation, metabolic changes (hyperkalemia, hyperinsulinemia, “oxidative stress”, etc.), increased sensitivity to intracardiac pain, chronic inflammation, increased arterial stiffness, etc. There are a number of hypotheses that determine the pathogenesis of syndrome X. According to the first of them, the disease is caused by myocardial ischemia due to functional or anatomical disorders of microcirculation in the intramuscular (intramural) prearterioles and arterioles, i.e. in vessels that cannot be visualized by coronary angiography. The second hypothesis assumes the presence of metabolic disorders leading to disruption of the synthesis of energy substrates in the heart muscle. The third hypothesis suggests that syndrome X occurs with increased sensitivity to painful stimuli (decreased pain threshold at the level of the thalamus) from various organs, including the heart. Despite intensive research over the past 35 years regarding the pathogenesis of coronary syndrome X, many important questions remain unanswered. Among them are the following: 1) whether the chest pain is of cardiac origin; 2) whether pain causes myocardial ischemia; 3) whether other mechanisms (besides ischemia) are involved in the origin of pain; 4) what is the role of myocardial dysfunction and a decrease in the pain threshold in the long-term prognosis of the disease. In recent years, various mechanisms of the formation of IHD have been intensively studied. At the cellular and molecular level, the state of endothelial cells, their metabolism, the role of the receptor apparatus, etc. is assessed. Various interactions between pain threshold and microvascular dysfunction may explain the heterogeneity of the pathogenesis of cardiac syndrome X. Both pain threshold and microvascular dysfunction have gradations in severity and are modulated by various factors such as endothelial dysfunction, inflammation, autonomic neural influences and psychological mechanisms. Among the listed causes, endothelial dysfunction in cardiac syndrome X appears to be the most important and multifactorial, i.e. associated with major risk factors such as smoking, obesity, hypercholesterolemia, as well as inflammation. For example, high plasma levels of C-reactive protein, a marker of inflammation and damage, correlate with the “activity” of the disease and the severity of endothelial dysfunction. Endothelial dysfunction is the earliest link in the development of atherosclerosis, it is determined already in the period preceding the formation of an atherosclerotic plaque, before the clinical manifestations of the disease, and damage to the endothelium, causing an imbalance in the synthesis of vasoconstrictor and vasorelaxant substances, leads to thrombus formation, adhesion of leukocytes and proliferation of smooth muscle cells in arterial wall. Endothelial dysfunction with decreased bioavailability of the endothelium-dependent relaxant factor nitric oxide (NO) and increased levels of endothelin-1 (ET-1) may explain the impaired microcirculation in cardiac syndrome X. In addition, low NO/ET-1 ratios are directly correlated with the severity of pain in these patients. Changes in the structure of blood vessels with impaired endothelial function lead to complications such as myocardial ischemia, heart attack, and stroke. Patients with multiple risk factors often have early coronary atheroma (undetected on coronary angiogram), which can impair endothelial function. Again, it is noteworthy that there is a predominance (approximately 70%) of postmenopausal women in the population of patients with cardiac syndrome X. They often present with atypical chest pain that lasts longer than with typical angina and may be resistant to nitroglycerin. Sometimes these women have mental illness. Estrogen deficiency is a pathognomonic factor that affects blood vessels through endothelium-dependent and endothelium-independent mechanisms. Symptoms Less than 50% of patients with cardiac syndrome X have typical exertional angina, and the majority have atypical chest pain. Despite its atypicality, pain in this syndrome can be very intense and can significantly impair not only the quality of life, but also ability to work. Many patients with cardiac syndrome X experience: a decrease in the internal pain threshold, the occurrence of chest pain during intravenous administration of adenosine, and a tendency to spastic reactions of the smooth muscles of internal organs. Symptoms accompanying cardiac syndrome X resemble vegetative-vascular dystonia. Cardiac syndrome X is often found in people who are suspicious, with a high level of anxiety, against the background of depressive and phobic disorders. Suspicion of these conditions requires consultation with a psychiatrist. Diagnosis Although there is no generally accepted definition of syndrome X, its clinical picture suggests the presence of three signs: 1) typical angina that occurs during exercise (less commonly, angina or shortness of breath at rest), 2) a positive result on an exercise ECG or other stress tests (ST segment depression on ECG, myocardial perfusion defects on scintigrams), 3) normal or non-narrowed (initial changes) coronary arteries on an angiogram. Therefore, syndrome X resembles stable angina. However, clinical manifestations in patients with syndrome X are very variable, and in addition to exertional angina, attacks of resting angina can also be observed. In patients with chest pain and “normal” coronary arteries, arterial hypertension is often identified, with or without ventricular hypertrophy. Hypertensive heart is characterized by endothelial dysfunction, changes in the ultrastructure of the myocardium and coronary bed, and a decrease in coronary reserve. Together or separately, these changes impair coronary blood flow and can cause angina. In such cases, control of arterial hypertension is of primary importance, allowing to restore the functional and structural integrity of the cardiovascular system. Using adequate provocative tests (with acetylcholine, etc.), the clinic tries to exclude spasm of the coronary arteries. In certain situations, for example, in the presence of a widespread perfusion defect or a focus of asynergy of the left ventricular wall and angiographically unchanged artery, intracoronary echocardiography (intravascular ultrasound) may be performed to exclude obstructive changes in the vessel. Table 1 shows the recommendations of the ESC (2006) for the examination of patients with the classic triad of syndrome X. Thus, cardiac syndrome X is diagnosed by exclusion. First of all, coronary atherosclerosis and other diseases of the coronary arteries are excluded. You should carefully collect an anamnesis with an analysis of concomitant symptoms and risk factors for cardiovascular diseases, the results of non-invasive stress tests, and also carry out a differential diagnosis with diseases and dysfunction of other organs (esophagus, spine, lungs and pleura, abdominal organs), certain diseases and valvular cardiac anomalies - vasospastic angina, mitral valve prolapse. It is necessary to differentiate cardiac syndrome X from cardialgia associated with impaired motility of the esophagus, fibromyalgia and osteochondrosis. Some cardiologists believe that in addition to chest pain typical of angina and ischemic ECG changes (horizontal or downsloping ST segment depression of 1 mm or more) or other evidence of heart damage (for example, detection of a transient defect in myocardial perfusion on thallium scintigraphy - 201), the subepicardial coronary arteries should be angiographically completely unchanged. However, even these strict angiographic criteria have their limitations, since it is known that coronary angiography may be uninformative (since it does not detect early atherosclerotic changes within the arterial wall, is not sensitive enough in diagnosing intracoronary thrombosis, does not help determine the internal structure of plaques and identify plaques prone to rupture and ulceration). At the same time, the stress ECG test in some patients with syndrome X may be uninformative due to its premature termination at low load due to fatigue, shortness of breath or chest discomfort. In these cases, a transesophageal electrical stimulation test or an intravenous dobutamine test can be used to detect myocardial ischemia. In cardiac syndrome X, transient perfusion defects have been shown to occur in areas supplied by poorly affected arteries. Single-photon emission computed tomoscintigraphy of the myocardium, along with the assessment of myocardial perfusion, allows one to determine the parameters of left ventricular contraction [5,6]. In some patients, local disturbances in the mobility of the heart wall are detected during stress echocardiography, magnetic resonance imaging, or disturbances in myocardial metabolism are determined during positron emission tomography. Intravascular ultrasound examination of the coronary arteries is of greatest importance precisely in cases where coronary angiography reveals normal or slightly altered coronary arteries. It allows you to study the surface and internal structure of atherosclerotic plaques, verify plaques of complex configuration, give them a quantitative assessment, examine the condition of the vascular wall around the plaque, and identify coronary artery thrombosis. However, the complexity of the technique, its high cost, and the need for highly qualified personnel prevent the widespread use of this valuable method. Table 2 shows the characteristic signs and examination plan of a patient with cardiac syndrome X. Differential diagnosis The group of patients with cardiac syndrome X is heterogeneous. Some experts include patients with systemic arterial hypertension, hypertrophic cardiomyopathy, or idiopathic dilated cardiomyopathy. However, most of them believe that patients with muscle bridges, arterial hypertension, pulmonary hypertension, valvular heart disease, mitral valve prolapse, left ventricular hypertrophy and diabetes mellitus should be excluded from coronary syndrome X, since in these cases it is assumed that the causes for the appearance angina pectoris are known. When diagnosing the disease in question, the following should also be excluded: patients with spasm of the coronary arteries (vasospastic angina), patients in whom non-cardiac causes of chest pain have been documented by objective methods (for example, musculoskeletal - osteochondrosis of the cervical spine, etc.; neuropsychic – anxiety-depressive syndrome, etc.; gastrointestinal – esophageal spasm, gastroesophageal reflux, gastric or duodenal ulcer, etc.). In addition to cardiac syndrome X (microvascular angina), there is also metabolic syndrome X. This “multi-metabolic syndrome” describes a combination of certain clinical signs and risk factors for CAD: abdominal obesity (waist/hip index >0.85), hypertension, impaired carbohydrate tolerance or type 2 diabetes mellitus, dyslipidemia (hypertriglyceridemia and decreased high-density lipoprotein levels). The unifying factors for all these clinical conditions in metabolic syndrome X are hypertriglyceridemia and tissue resistance to insulin [7]. Other characteristics of these patients include hyperuricemia, physical inactivity, and premature aging. However, both described syndromes X can be combined in one patient. Drug treatment Insufficient attention of cardiologists to the pathology in question does not lead to the disappearance of the problem. Treatment for the group of patients with syndrome X remains not fully developed, so the right drug strategy can improve the quality of life of patients and reduce the financial costs of healthcare. Various approaches to drug treatment are used (antianginal drugs, ACE inhibitors, angiotensin II receptor antagonists, statins, psychotropic drugs, etc.). The choice of treatment is often difficult for both treating physicians and the patients themselves. The success of treatment usually depends on the identification of the pathological mechanism of the disease and is ultimately determined by the participation of the patient himself. An integrated approach to the treatment of patients with cardiac syndrome X is often necessary. General advice on changing the quality of life and treating risk factors, especially aggressive lipid-lowering therapy with statins (reducing total cholesterol to 4.5 mmol/l, LDL cholesterol to less than 2.5 mmol/l ), should be considered as vital components of any chosen treatment strategy. Antianginal drugs such as calcium channel blockers (nifedipine, diltiazem, verapamil, amlodipine) and
Pathophysiology of coronary microvascular dysfunction (CMD)
The myocardium is an aerobic muscle tissue that requires a continuous supply of oxygenated blood to produce the energy needed to maintain the pumping function of the heart. Under basic cardiac conditions, 60–70% of the required oxygen can be obtained from arterial blood, so the increased myocardial oxygen demand can only be met by increasing coronary blood flow. The proximal coronary bed consists of epicardial arteries with a diameter of 5 to 0.5 mm and gives rise to intramural vessels. The distal coronary bed is represented by prearterioles, arterioles with a diameter of 40 to 400 μm and capillaries with a diameter of less than 10 μm, which constitute the main coronary circulatory system [10]. At rest, the tone of the coronary microvasculature is high, but arteriolar diameter can change rapidly, responding to increased myocardial oxygen demand and increasing coronary blood flow [11]. Capillaries and venules are an important component of the coronary microcirculation, therefore, structural and functional disorders at this level (for example, a drop in blood pressure in the capillary network or microembolization) can cause the development of myocardial ischemia. Depending on the clinical picture, different pathogenetic mechanisms of microvascular dysfunction are distinguished (Table 1) [12].
According to A. Faccini et al., inflammation is another potentially important cause of the development of CMD [13]. Coronary microvascular spasm, originally described in [14], can, like epicardial spasm, cause myocardial ischemia in the absence of increased myocardial oxygen demand and initiate resting angina. Today, there is no doubt that MWS is a heterogeneous syndrome, the development of which may be based on various pathogenetic mechanisms. Proposed mechanisms of CMD include altered regulation of coronary microcirculation by the autonomic nervous system and generalized vascular disorders. Thus, in one of the large studies by P. Ong et al. [15, 16] during testing of patients for acetylcholine, every fourth patient experienced microvascular spasm, characterized by ischemic changes on the ECG without visible changes in the diameter of the epicardial coronary arteries. AL Arrebola-Moreno et al. [17] reported that coronary microvascular spasm induced by intracoronary acetylcholine leads to disturbances in myocardial perfusion and contractility. In the VR study, Taqueti et al. [18] found a direct connection between CMD and the development of heart failure in patients with preserved ejection fraction. However, in most cases, MWS develops as a result of isolated CMD [19], which is the only (or predominant) mechanism responsible for the development of an attack of angina or asymptomatic myocardial ischemia [20].