Content:
- Determination of intermenstrual bleeding in the middle of the cycle
- Types of intermenstrual bleeding
- Causes of bleeding and menstruation in the middle of the cycle
- Diagnosis of bleeding in the middle of the cycle
- Treatment and prevention of bleeding in the middle of the cycle
- Poor blood flow during pregnancy
Many women experience menstruation in the middle of their cycle at least once in their lives.
Naturally, an irregular menstrual cycle causes anxiety in women. Such disorders can occur in teenage girls and women of reproductive age. Often, spotting in the middle of the cycle is not a symptom of any disease and is considered normal. But sometimes the appearance of bleeding between periods can be a sign of serious gynecological diseases.
Common systemic causes
These are systemic pathologies that can affect several systems, which among the symptoms can also produce vaginal bleeding.
For example:
- bleeding disorders such as hemophilia A and B, von Willebrand disease, platelet function disorders;
- leukemia and lymphomas;
- liver failure;
- renal failure;
- severe dysthyroidism.
An important and fundamental classification for tracking the various causes of vaginal bleeding is the classification by age group.
Determination of intermenstrual bleeding in the middle of the cycle
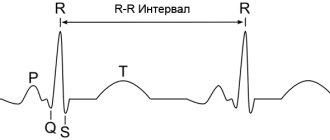
Menstruation is one of the phases of the menstrual cycle of the female body, characterized by the release of blood from the vagina. The beginning of the menstrual cycle is counted from the first day of menstruation.
Sometimes it can be difficult to distinguish dysfunctional uterine bleeding from normal menstruation. Many girls do not remember when their menstrual cycle began and do not know how to calculate their menstrual cycle, so they may mistakenly think that menstruation came earlier or later than expected. For each woman and girl, the duration of the monthly cycle is individual
How to calculate the monthly cycle? It is not difficult. The easiest way is to keep a monthly calendar. It needs to mark 1 day of the onset of menstruation and 1 day of the next menstruation. The number of days between them will be the duration of the menstrual cycle. You need to know that normal menstruation lasts 2-7 days, and the normal menstrual cycle is 21-35 days. The most optimal duration of the monthly cycle is 28 days. Women who experience an irregular menstrual cycle should consult a gynecologist.
Ovulation is the process of the release of a mature egg from the follicle. In women with a normal monthly cycle, ovulation occurs approximately on the 14th day from the start of menstruation. With an irregular menstrual cycle, it may occur earlier or later than this time. After ovulation, the level of estrogen in the female body decreases, and bleeding does not occur because the corpus luteum maintains hormonal balance. A sharp increase or decrease in the level of the hormone estrogen during ovulation can provoke uterine bleeding between, before and after menstruation, and this is not a deviation from the norm. This phenomenon is observed in 30% of women.
Symptoms
Along with vaginal bleeding, other symptoms sometimes occur due to the underlying pathology. The most common:
- abdominal or pelvic pain (due to anovulation and other causes);
- vaginal discharge (with genital infection);
- asthenia and general malaise;
- nausea and vomiting;
- feeling tired;
- pallor and tachycardia associated with anemia secondary to bleeding that reduces hemoglobin levels.
Types of intermenstrual bleeding
Intermenstrual bleeding often occurs 10-16 days after the end of the last menstrual period. They are not very abundant and last from 12 to 72 hours. But if the bleeding lasts longer or gets worse, consult your gynecologist.
Spotting in the middle of the cycle is more common than intermenstrual bleeding. A woman's vagina comes out with a little blood that can barely be seen on the toilet paper. This is usually mucus that has a pinkish color. Such discharge appears approximately 14 days before the onset of menstruation and is not a pathology. Intermenstrual bleeding indicates that the egg is ready for fertilization.
Frequent periods can also occur with proyomenorrhea (short monthly cycle). Periodically appearing and usually not intense bleeding lasts 2-3 days. Such spotting is caused by premature rejection of the uterine mucosa due to a decrease in estrogen production in the middle of the menstrual cycle.
Benign organic pathologies
Uterine fibroids and endometrial polyps are among the most common causes of vaginal bleeding during the fertile phase. The former are nothing more than abnormal growths of muscle tissue, and the latter are the endometrial mucosa. They can increase in size and often, in combination with hormonal changes, cause bleeding in the form of menorrhagia and metrorrhagia. In this category, it is also important for us to consider ovarian cysts.
Endometriosis means the abnormal presence of endometrium in organs other than the uterus, such as the ovary, fallopian tube, peritoneum, vagina, intestines, lungs. These ectopic lesions may also bleed during the normal menstrual cycle.
Occasional light-colored spotting, possibly worsening with sexual intercourse, may be caused by the presence of an ectropion (an "ulcer" on the cervix).
Genital infections can cause various types of vaginal discharge, but only rarely do they cause bleeding. The most common are those that are sexually transmitted - chlamydia and gonorrhea.
Causes of bleeding and menstruation in the middle of the cycle
Often, an irregular menstrual cycle is observed in teenage girls, since at their age the hormonal background has not yet become stable. If, after 2 years after the first menstruation, girls still have periods in the middle of the cycle, then you need to consult a gynecologist who will prescribe treatment to normalize the menstrual cycle.
Constant strong stressful situations, smoking, and alcohol have a bad effect on the body. As a result, women experience irregular menstrual cycles and may experience periods mid-cycle. Such phenomena often occur in women with frequent dysfunction of the genitourinary system; bleeding in such cases is more profuse.
If you move to another city, country or go on vacation to the sea, be prepared for the fact that the start of your menstrual cycle may occur earlier than usual and your period may begin in the middle of the cycle. After all, climate change is also stressful for the body, and it needs time to get used to it.
There can be many factors that provoke bleeding between periods. The main ones:
- pathologies of the endocrine system (diseases of the thyroid gland and adrenal glands, etc.);
- uterine fibroids;
- hormonal disbalance;
- miscarriage;
- the presence of an intrauterine device;
- gynecological procedures (cauterization or cervical biopsy);
- taking certain medications and contraceptives;
- vaginal trauma and vaginal infections.
- depression and stress.
- infectious diseases;
- poor blood clotting;
- deficiency of vitamins K and C;
- inflammation of the urogenital system;
- pathologies of the development of the internal genital organs of a woman (uterine inflection);
- ovarian tumors and cysts;
- chronic diseases (heart, kidney, liver and metabolic disorders);
- physical injuries.
Also, intermenstrual discharge may indicate such serious problems of the female genital area as uterine cancer, polyps and fibroids of the uterus, and the presence of adhesions.
The main causes of vaginal pathological bleeding
There are many causes of vaginal bleeding, but they can generally be grouped into 5 broad categories:
Complications during pregnancy (sometimes undiagnosed, that is, which the woman does not yet know about) include:
- abortion (miscarriage);
- ectopic pregnancy;
- gestational trophoblastic disease.
Dysfunctional reasons:
- anovulatory cycles;
- polycystic ovary syndrome;
- less often metrorrhagia.
Benign organic pathologies:
- uterine fibroids;
- uterine polyps;
- adenomyosis;
- endometriosis;
- genital infections.
Malignant organic pathologies:
- endometrial cancer;
- cervical cancer;
- vaginal cancer;
- sarcomas.
Common systemic causes:
- blood clotting pathologies;
- leukemia;
- hypothyroidism;
- liver and kidney failure.
Spotting may occur during the first cycles of taking hormonal contraceptives (birth control pills) and after using the hormonal IUD.
Diagnosis of bleeding in the middle of the cycle
First of all, to diagnose the causes of intermenstrual bleeding, a gynecological examination is necessary. In addition, you must undergo the following examinations:
- cytological studies of aspirate from the uterine cavity;
- Ultrasound of the pelvic organs;
- study of the hormonal background of the body;
- thyroid examination;
- hysteroscopy and curettage of the uterine cavity and cervical canal;
- histological examination of scrapings obtained from the uterine cavity and cervical canal.
Also, if necessary, the gynecologist can prescribe a study of the pituitary gland using magnetic resonance imaging, radiography, computed tomography. Sometimes the brain is also examined using these methods.
Brown discharge instead of menstruation
Finding brown “smudge” or clots on the pad instead of the usual menstrual discharge is frightening and makes you think about the worst. But brown color is not always a sign of pathology. Temporary changes in the nature of menstruation can be caused by:
- Taking medications. Antibiotics, hemostatic agents, antidepressants and drugs for the treatment of peptic ulcers cause brown marks instead of menstruation.
- Features of lifestyle. Changes in menstrual discharge are provoked by smoking, heavy physical activity, working in hazardous industries, and alcohol abuse.
- Climate change.
- Diets. Restriction in food leads to insufficient intake of beneficial microelements into the body, and this affects the nature of menstruation.
- Age characteristics. In girls, when the menstrual cycle begins, brown lochia may be released instead of blood for the first time. Before menopause, changes in hormonal levels can cause scanty brown periods.
Brown periods can be caused by:
- inflammation of the reproductive system;
- tumors in the uterus;
- polyps;
- ectopic pregnancy;
- venereal diseases.
Benign tumors of the uterus
Whether the condition is dangerous or caused by relatively “harmless” reasons, only a gynecologist can answer.
Treatment and prevention of bleeding in the middle of the cycle
Treatment methods for bleeding in the middle of the cycle depend on the causes of this deviation, as well as on the woman’s age. Treatment can be conservative or surgical. In case of ovulatory bleeding, conservative treatment is carried out. For anovulatory bleeding (not associated with ovulation), both surgical and conservative treatment may be necessary. The exception is anovulatory bleeding in adolescents, when surgical treatment is used only as a last resort.
Conservative treatment is based on the use of hormonal drugs to normalize the irregular menstrual cycle and stop bleeding. Your doctor may also prescribe sedative medications to treat untimely periods caused by stress.
For severe bleeding, women are prescribed iron supplements. It should be remembered that a balanced diet (including foods such as beef, legumes, liver, vegetables and fruits), proper rest and sleep will help restore health faster.
To prevent bleeding in the middle of the cycle, you need to: regularly see a gynecologist, refuse abortions, have a regular sex life, control your weight, play sports, give up bad habits.
If you notice that your period starts earlier or later each time, please consult a qualified healthcare professional. Untimely treatment of pathologies that cause disruption of the monthly cycle and bleeding can lead to anemia, infertility, and cervical cancer.
Diagnostics
The diagnosis is made based on observation of symptoms and the general clinical picture associated with the use of instrumental studies.
Gynecologist assesses bleeding characteristics:
- duration;
- intensity;
- associated symptoms;
- main pathologies.
If the bleeding is quite cyclical and regular, it is likely due to benign organic lesions or anovulation. If bleeding is irregular, the possibility of malignancy should also be considered.
Blood tests are performed to assess whether the patient has anemia, which in severe cases requires supportive care, including blood transfusion.
Blood tests
From an instrumental point of view, the gold standard for diagnosing vaginal bleeding is transvaginal ultrasound, which can identify both benign and malignant organic lesions, evaluate the characteristics of the endometrial mucosa and any changes in the ovaries.
The ultrasound results may then require other methods such as
- CT scan of the abdomen and pelvis;
- Nuclear magnetic resonance;
- In case of organic lesions - hysteroscopy and endometrial biopsy.
But first of all, the possibility of pregnancy is always excluded using an hCG test.
Poor blood flow during pregnancy
During pregnancy, it is extremely important to continuously monitor the state of the maternal body of the mother and the baby, it is important that they perform all vital functions. One of the most significant studies is the analysis of blood flow in the arteries of the uterus, the woman’s umbilical cord, as well as cerebral vessels and the fetal aorta. The main causes of perinatal morbidity and mortality include disorders of the uteroplacental blood flow of 1A, 1B, second and third degrees.
Blood flow in the placenta
The placenta, in which the fetus is located, supplies the embryo with nutrients, as well as oxygen from the mother’s blood; it also removes waste products from the child’s body. It is this organ that unites two rather complex vascular systems - the female, which connects the vessels of the uterus and placenta, and the fetal, which passes into the umbilical arteries and leads to the child.
The circulatory systems mentioned above are separated by a membrane, which does not allow maternal and child blood to mix. The placenta is a kind of barrier that is resistant to numerous harmful substances, as well as viruses.
Often, for completely different reasons, placental insufficiency may appear, which inevitably affects the performance of transport, metabolic, trophic, endocrine and other vital functions of the placenta. In this condition, the metabolism between the maternal and child organisms deteriorates significantly, which is fraught with various consequences.
What are the causes of impaired placental blood flow?
Poor circulation in the uterine cavity can be caused by pneumonia, increased blood pressure, various intrauterine infections, as well as insufficient oxygen supply to the child’s body (hypoxia).
To diagnose the blood flow system in modern obstetric practice, three-dimensional ultrasound (so-called Doppler ultrasound) is used, with which the vessels are visible in a 3D (three-dimensional) image. With the help of this diagnostic technique, there is a prospect of diagnosing retroplacental bleeding and assessing cardiac malformations by monitoring blood flow. This technique is irreplaceable, since with its help it is possible to examine defects even in the most microscopic vessels that form the microvasculature, to observe the peculiarities of the formation and development of intraplacental hemodynamics, and in addition to control the amount of nutrients, as well as oxygen, that should enter the fetal body . New prospects have opened up for the early detection of obstetric complications, and if treatment or correction is started without wasting time, then circulatory disorders and subsequent pathologies associated with it can be almost completely avoided.
Hemodynamic disorders during pregnancy
Hemodynamic disorders are divided into 3 degrees of severity:
1. 1st degree includes two subtypes:
- disturbance of patello-placental blood flow 1Is the mildest. Fetal-placental blood circulation is preserved with it. Intrauterine infections often lead to this problem;
- in degree 1B, uteroplacental blood flow is preserved, but fetal-placental pathologies appear.
2. Grade 2 is characterized by the presence of disturbances in both blood flow systems, however, these disturbances do not carry any fundamental changes. 3. In grade 3, uterine circulation disturbance causes defects in normal blood circulation at the level of the fetus.
In the case of the first degree of violations, timely detection and adequate treatment can avoid fetal death. In the case of the second degree, perinatal mortality is about 13.3 percent, in the case of the third - 46.7 percent. During Doppler diagnostics, it was revealed that treatment aimed at correcting placental insufficiency in women with third-degree uterine blood flow disorders was ineffective. In this situation, with conservative childbirth, perinatal mortality was 50 percent, then, thanks to a cesarean section, losses can be avoided. 35.5 percent of newborns are admitted to the intensive care unit with grade 1 blood flow disorders, 45.5 percent with grade 2, and 88.2 percent with grade 3.
Vaginal discharge: normal and pathological. Or what a woman needs to pay attention to.
Vaginal discharge: normal and pathological. Or what a woman needs to pay attention to.
Many women, “obsessed” with the cleanliness of the body, strive in every possible way to get rid of vaginal discharge, considering it a manifestation of “uncleanliness” and ill health. They do not understand that the presence of vaginal discharge is as physiological as the formation of saliva, tears, gastric juice and other physiological secretions. Getting rid of these secretions is pointless and unsafe.
On the other hand, there are a number of diseases in which changes in the nature of the discharge are the first alarming sign, forcing a woman to consult a gynecologist. Let's try to figure out where the border between normality and pathology lies.
Before finding out which discharge is normal and which is clearly pathological, it is important to understand what vaginal discharge is: where it comes from and what it consists of.
Vaginal discharge includes:
- mucus produced by the glands of the cervical canal (cervical canal);
- epithelial cells of the cervical and vaginal canal, which are constantly exfoliated from the walls into the vaginal lumen;
- microflora, represented by 5-12 types of microorganisms (bacteria, viruses, fungi) that normally populate the vagina (the cervix, uterine cavity, tubes and ovaries are normally sterile).
Normal vaginal flora in women of reproductive age is mainly represented by lactic acid bacteria (lactobacillus, Dederlein bacilli) - the number of colonies found during bacterial culture of secretions is 10 to 7 degrees and higher. Streptococci, bacteroides, enterobacteria, and fungi are found in small quantities. In very small quantities (less than 10 to the 4th power) opportunistic microorganisms are found - mycoplasma, ureaplasma, fungi of the genus Candida, Gardnerella. The mere fact of detecting these microbes does not indicate the presence of a disease.
Thanks to lactobacilli, vaginal discharge normally has an acidic environment (pH value 3.8-4.4), which causes the discharge to have a sour odor (not always).
Normal discharge
There are several types of normal vaginal discharge, the nature of which depends on the woman’s age, hormonal status, the presence or absence of sexual activity and other factors.
Let’s immediately make a reservation that girls should not have vaginal discharge before puberty. This fact is due to the characteristics of the hormonal profile and the structure of the genital organs in this age period. The appearance of vaginal discharge in a girl under 10-12 years of age, especially discharge that has color and odor, indicates trouble either in the reproductive system or in the nearby digestive or urinary tract.
About a year before the start of the first menstruation, girls begin to experience vaginal discharge due to hormonal changes in the body, the transition of the body from the “girl” state to the “girl” state. These discharges are liquid, sometimes mucous, have a whitish color or a faint yellow tint, are odorless or have a faint sour odor. These secretions are physiologically normal and necessary to moisturize the vaginal wall and protect the genitals from infectious agents. Naturally, normal discharge is not accompanied by sensations such as pain, itching, burning and does not lead to redness and swelling of the skin and mucous membrane of the external genitalia.
After the onset of menstruation and the establishment of a regular menstrual cycle, normal vaginal discharge is characterized by a cyclic change in properties and qualities depending on the phase of the menstrual cycle. In the first phase of the menstrual cycle (with a 28-day cycle - from the end of menstruation to the 12-13th day of the cycle, which is counted from the first for menstruation 0) - the discharge is light (1-2 ml per day - the diameter of the spot on a panty liner is 2- 3 cm), watery or slimy in nature, have a uniform consistency (or there may be impurities in the form of small (up to 2 mm) lumps), they are colorless or have a whitish or yellowish tint, odorless or with a weak sour odor.
During the period of ovulation (1-2 days in the middle of the cycle), the amount of discharge increases to 4 ml per day (the size of the spot on a panty liner increases to 5 cm), it becomes mucous, viscous, and sometimes the color of the discharge becomes beige.
In the second half of the menstrual cycle, the amount of discharge (compared to the ovulatory period) decreases, and the discharge may become creamy or jelly-like in nature. A few days before the onset of menstruation, a repeated increase in the amount of discharge is typical. This cyclical change in the nature of discharge is conditionally maintained throughout the woman’s entire reproductive period - from the establishment of a regular menstrual cycle to the appearance of the first signs of extinction of the hormonal function of the ovaries in premenopause.
However, there are many factors that, while not pathological, change the nature of vaginal discharge.
Such factors include the onset of sexual activity and a change of sexual partner, sexual intercourse itself, taking hormonal contraceptives, changing intimate hygiene products or the composition of underwear, pregnancy, and the postpartum period.
Let us consider the influence of these factors on the nature of discharge in detail.
The onset of sexual activity and a change of sexual partner lead to the fact that a new, alien, unfamiliar, although absolutely normal, non-pathogenic microflora enters the woman’s genital tract. As a result, over a certain period of time (purely individual for each woman), the reproductive system and the woman’s entire body adapt to the “new residents.” This period is characterized by an increase in the amount of discharge, a change in color and consistency. The main thing is that there are no unpleasant sensations (discomfort, itching, burning).
Sexual intercourse itself also contributes to the appearance of specific vaginal discharge. Within a few hours after unprotected sexual intercourse (without using a condom), vaginal discharge looks like transparent clots with a white or yellowish tint. 6-8 hours after sexual intercourse, the nature of the discharge changes: it becomes liquid, white, and abundant. If sexual intercourse was protected by a condom or the method of interrupted sexual intercourse was used, then after it the release of a creamy, white, scanty secretion consisting of “worked-out” vaginal lubrication is characteristic.
Taking hormonal contraceptives helps to change the hormonal profile, which plays a fundamental role in the formation of vaginal discharge. Inhibition of ovulation, on which the action of almost all hormonal contraceptives is based, leads to a decrease in the amount of discharge (during the period of taking the pills). After discontinuation of the contraceptive, the nature of vaginal discharge is restored.
Breastfeeding has a similar effect on the nature of discharge. At the end of the postpartum period, the amount of vaginal discharge is very small (provided the baby is fed “on demand” and there are no periods).
During pregnancy, the hormonal status of the body also changes, affecting the structure and function of many organs. The amount of vaginal discharge in pregnant women, as a rule, increases due to increased blood supply to the organs of the reproductive system and the penetration of a small amount of plasma (the liquid part of the blood) through the walls of the vagina into its lumen. The discharge becomes abundant, watery and causes the need to change panty liners more often.
At the end of pregnancy, the amount of discharge increases further due to mucus leaving the cervical canal, which serves as a harbinger of the approaching birth. A pregnant woman should be very attentive to her condition, including monitoring the nature of vaginal discharge. For example, the appearance of very thin discharge in the second half of pregnancy should necessarily alert a woman and become a reason to consult a doctor, since a similar picture can be observed when amniotic fluid breaks.
Normal discharge after childbirth is called lochia.
Lochia is a physiological postpartum discharge from the uterus, consisting of blood, mucus and rejected, non-viable tissue (decidua of the uterus). Normally, the duration of lochia discharge is 3-6 weeks after birth (sometimes up to 8 weeks). It is important that there is a tendency towards lightening and a decrease in the number of lochia. In the first week after birth, lochia is comparable to regular periods, only they are more abundant and may contain clots.
Then their number decreases every day. Gradually they acquire a yellowish-white color due to a large amount of mucus (become similar to egg whites), and may contain a small admixture of blood. Approximately by the 4th week, scanty, “spotting” discharge is observed, and by the end of the 6-8th week after birth, vaginal discharge acquires the same character as before pregnancy. The amount of discharge during perimenopause (the period that includes the period of time before the end of menstruation, the last menstruation and the entire subsequent life of the woman) progressively decreases. Coccal microorganisms (staphylococci, streptococci) predominate in vaginal discharge during this period (as well as in girls before puberty). We remind you once again: normally there should not be the slightest sensation of discomfort in the genital area, no pain, no itching, no burning. The appearance of these symptoms, even against the background of a supposedly normal discharge, should be a signal of the need for immediate consultation with a gynecologist.
Pathological discharge
Now let's talk about clearly pathological vaginal discharge.
Let us say right away that by the nature of the discharge it is almost impossible to accurately establish a reliable diagnosis, since in most cases there is a combination of two or more pathological processes, and doctors are often faced with atypical manifestations of a particular disease. Therefore, based on the appearance of the discharge, one can only assume the development of a certain pathological process, and its presence must be proven by the data of clinical, laboratory and instrumental examinations.
The most common causes of changes in the nature of vaginal discharge are specific infectious and inflammatory diseases of the reproductive system, namely trichomoniasis, candidiasis, chlamydia, gonorrhea, as well as bacterial vaginosis and nonspecific inflammatory diseases of the genital organs.
Let's figure out what the discharge looks like during these pathological processes, and using what methods you can confirm or refute the diagnosis.
Trichomoniasis.
Copious white, yellowish or greenish foamy discharge with an unpleasant odor, accompanied by itching and/or burning, painful urination. To clarify, it is necessary to study a native smear or a smear after Romanovsky-Giemsa staining, or a PCR study of vaginal discharge or a cultural method.
Thrush (candidiasis).
Thick discharge, similar to lumps of yellowish cottage cheese, the amount of discharge is significantly increased. As an accompaniment - exhausting intense itching of the genitals and irritation (redness, swelling) of the external genitalia. Confirmation - microscopic examination of vaginal smears, bacterial culture of discharge.
Bacterial vaginosis.
The amount of discharge increases significantly, the color of the discharge is grayish-white, an unpleasant odor appears (the smell of rotten fish) and a mild, periodic itching of the external genital organs appears. Symptoms worsen after sexual intercourse. If the process lasts for a long time, the discharge becomes yellow-green, sticky, and when examined in the mirror, it is evenly “smeared” over the walls of the vagina. To confirm the diagnosis, bacterial culture of vaginal discharge is performed.
Chlamydia.
Increased discharge is uncommon. The discharge is characterized by a yellow color (this sign is especially noticeable to the doctor when examining a woman in the mirror, since the discharge comes from the cervical canal and flows down the walls of the vagina), often accompanied by pain in the lower abdomen, painful urination, enlargement and soreness of the Bartholin gland. The diagnosis is confirmed by cultural examination and PCR examination of discharge from the cervical canal.
Gonorrhea.
Moderate yellowish-white vaginal discharge, accompanied by pain in the lower abdomen, pain when urinating and, often, intermenstrual bleeding. To confirm the diagnosis, microscopic examination of discharge, bacteriological culture and PCR research are used.
Nonspecific vaginitis (colpitis).
Vaginal discharge is the main symptom. Their characteristics are varied: liquid, watery, sometimes thick, purulent, often foul-smelling, often mixed with blood. Acute inflammation is accompanied by itching, burning or heat in the genital area. The diagnosis is confirmed by microscopic examination of vaginal smears.
A special place in gynecology is occupied by vaginal discharge mixed with blood.
In most cases, spotting outside of menstruation indicates the presence of a disease and indicates the need to see a doctor. Some doctors believe that intermenstrual vaginal bleeding is a harmless phenomenon caused by hormonal fluctuations associated with ovulation. However, such discharge sometimes occurs in connection with menstrual irregularities, and may also indicate the presence of a sexually transmitted infection (for example, gonorrhea), endometriosis, polyposis, chronic inflammation of the uterus (endometritis), etc. and therefore require special attention and examination (consultation with a gynecologist, microscopic and bacteriological analysis of discharge, colposcopy, ultrasound of the pelvic organs).
Any bloody discharge (of any color, in any quantity, of any duration) that occurs during pregnancy should be alarming. Even if they are not accompanied by pain. The cause of such discharge may be the threat of miscarriage, incorrect location of the placenta (placenta previa), or premature placental abruption. A less dangerous cause of bleeding in pregnant women is micro-ruptures in the vessels of the eroded cervix that occur after sexual intercourse. Only a doctor can determine the true cause of bleeding, so if such discharge appears, a visit to the doctor is indicated.
How to distinguish normality from pathology: vaginal pH test CITOLAB
One of the main criteria that allows you to assess the state of the vaginal microflora is the pH level of the discharge. In a normal state, the ratio of vaginal microflora is balanced: lactobacilli predominate, which create an acidic environment (pH 4.0-4.4). This is a natural protection against the entry and proliferation of pathogenic microorganisms. Changes in the pH of the vaginal environment can be associated with various reasons: candidiasis, trichomonas or bacterial infection.
Today it is possible to determine the pH of vaginal discharge without resorting to complex tests. Thanks to the creation of the CITOLAB vaginal pH test from , determining the pH of vaginal discharge has become possible even at home. Using this test, you can determine the deviation of the acidity of the vaginal environment from the normal level (pH≥4.7), which is a sign of a vaginal infection.
The CITOLAB pH test makes it possible to detect the disease at an early stage and begin treatment on time, which is important, as it allows you to avoid complications of the disease. However, you should remember that to clarify the causative agent of the disease, you will need additional examinations, which your gynecologist will prescribe for you.
Finally
To summarize the above material, we repeat: vaginal discharge, in most cases, is normal. Their absence, changes in characteristics, the appearance of blood, itching, burning, and discomfort should be alarming. In all of the above cases, it is necessary, without delay, to seek advice from a gynecologist. Take care of your health!
Articles on the topic All about colposcopy. Diagnostics,... What is the thyroid gland?...
A little about women's rules of feminine hygiene Breast care before and during... Eat right during... How to increase immunity? Interview…
Prices for services
Initial appointment with a gynecologist + ultrasound (assessment of complaints, medical history, examination in a gynecological chair, pelvic ultrasound, consultation)
Primary appointment – visiting a doctor of a specific specialty for the first time. Make an appointment
1800 ₽
Repeated appointment with the gynecologist
With the exception of repeated appointments with doctors: Blatsios N.D., Dzhashiashvili M.D. Make an appointment
1200 ₽
Ultrasound of the pelvis in women (uterine cavity, ovaries)
Make an appointment
1300 ₽
Endometrial hyperplasia
Spotting, bloody, brown discharge at the end of the cycle before menstruation or for a long time after menstruation may indicate endometrial hyperplasia. The causes of hyperplasia can be of different nature. Most often, this pathology develops due to hormonal imbalances, as well as carbohydrate, lipid and other types of metabolism. An important role may be played by hereditary predisposition, the presence of uterine fibroids, cancer of the genital organs and breast, hypertension and other diseases, manifestations of damaging effects during the prenatal period of development, diseases during puberty and the disorders of menstrual and subsequently reproductive function caused by them. The appearance of hyperplasia in adulthood is often preceded by previous gynecological diseases, abortions, and genital surgeries.
Doctors' opinion
According to experts, spotting cannot be ignored. After all, they can cause hormonal imbalance, pathologies, and diseases. And in this case, timely treatment will provide effective results.
According to doctors, urine with blood in women without pain is not always a pathology, but still requires diagnosis. In this case, a number of examinations are carried out:
- General urine and blood tests that reveal inflammation and suggest what actions the doctor needs to take in the future.
- Biochemical tests, thanks to which it is possible to determine the content of components such as proteins.
- A three-glass urine test, with which you can clearly determine the cause of the appearance of blood.
- The Nechiporenko urine collection method, which reveals a more detailed picture of the disease.
- Bacterial urine analysis, thanks to which you can determine the type of infectious agents (if any).
- Ultrasound of the genitourinary system - shows the condition of the woman’s organs.
- X-ray of the kidneys and reproductive system is necessary if the ultrasound did not give a complete picture.
- Cystoscopy, urethroscopy - in this case, a smear is taken for biochemistry to exclude the presence of dangerous diseases.
- CT and MRI are indicated only for those women in whom doctors suspect the presence of tumors.
Each of these studies is very important, but a urine test should be ordered first. With its help, the doctor determines the basic picture of the disease and draws up a plan for further action.
Doctors also insist that you should not self-medicate. Only after a complete examination is complex therapy or surgery prescribed, and the patient must constantly notify the gynecologist about his condition. In this case, we can talk about a quick solution to the problem and the return of health to the woman.