Action potential, its phases, their origin.
An action potential is a rapid fluctuation in membrane potential that occurs when the membrane is excited.
Phases: 1) slow depolarization (also a local response) - occurs due to an increase in membrane permeability for sodium ions. The subthreshold stimulus is not sufficient to cause rapid depolarization immediately. The duration of the phase depends on the strength of the stimulus.
2) rapid depolarization - characterized by a rapid decrease in membrane potential and even recharging of the membrane (overshoot): its inner part becomes positively charged for some time, and the outer part negatively. This occurs due to an avalanche of sodium entering the cell. Unlike the local response, the speed and magnitude of depolarization does not depend on the strength of the stimulus. The duration of the depolarization phase in the frog nerve fiber is about 0.2 - 0.5 ms.
3) repolarization (duration 0.5-0.8 ms) - the membrane potential is gradually restored and reaches 75 - 85% of the resting potential.
Phases 2 and 3 are called the peak of the action potential.
4) trace depolarization - is a continuation of the repolarization phase and is characterized by a slower (compared to the repolarization phase) restoration of the resting potential
5) trace hyperpolarization - is a temporary increase in membrane potential above the initial level.
Phases 4 and 5 are called trace phenomena
The relationship between the phases of excitability and the phases of the action potential. Refractoriness and its causes.
The level of cell excitability depends on the AP phase. During the local response phase, excitability increases. This phase of excitability is called latent addition. In the phase of AP depolarization, when all sodium channels open and sodium nonas rush into the cell like an avalanche, no even very strong stimulus can stimulate this process. Therefore, the phase of depolarization corresponds to a phase of complete inexcitability or absolute refractoriness, i.e. During the repolarization phase, an increasing part of the sodium channels closes. However, they can reopen under the influence of a suprathreshold stimulus. Those. excitability begins to rise again. This corresponds to a phase of relative inexcitability or relative refractoriness. During trace depolarization, the MP is at a critical level, so even subthreshold stimuli can cause cell excitation. Consequently, at this moment her excitability is increased. This phase is called the phase of exaltation or supernormal excitability.
At the moment of trace hyperpolarization, the MP is higher than the initial level, i.e. further CUD and its excitability is reduced. It is induced in the phase of subnormal excitability. Rice. It should be noted that the phenomenon of accommodation is also associated with a change in the conductivity of ion channels. If the depolarizing current increases slowly, this leads to partial inactivation of sodium and activation of potassium channels. Therefore, the development of PD does not occur.
Trace phenomena, their origin.
Trace phenomena are associated with recovery processes that slowly develop in nerve and muscle fibers after stimulation. There are two types of trace phenomena:
1) A trace negative potential or a trace depolarization of the membrane. The occurrence of the trace depolarization phase is explained by the fact that a small part of the slow sodium channels remains open. Trace depolarization is well expressed in the pulpal nerve fibers.
2) Trace positive potential or trace hyperpolarization of the membrane. Trace hyperpolarization is associated with increased, after PD, potassium conductivity of the membrane and the fact that the sodium-potassium pump, which removes sodium ions that entered the cell during PD, is more active. Trace hyperpolarization is well expressed in non-pulp nerve fibers.
Local and spreading excitation. Local response
Excitation can be of 2 types:
-local (local response);
-propagating (pulse).
Local excitation is the most ancient type (lower forms of organisms and low excitable tissues - for example, connective tissue). Local excitation also occurs in highly organized tissues under the influence of a subthreshold stimulus or as a component of an action potential. With local excitation there is no visible response.
Features of local excitation:
-there is no latent (hidden) period - it occurs immediately upon the action of the stimulus;
-no irritation threshold;
- local excitation is gradual - the change in the charge of the cell membrane is proportional to the strength of the subthreshold stimulus;
-there is no refractory period; on the contrary, a slight increase in excitability is characteristic;
-spreads with decrement (attenuation).
Impulse (spreading) excitation is inherent in highly organismal tissues and occurs under the influence of threshold and superthreshold stimuli.
Features of impulse excitation: -has a latent period - some time passes between the moment of application of irritation and the visible response; -has a threshold of irritation; -not gradual - the change in the charge of the cell membrane does not depend on the strength of the stimulus; - presence of a refractory period; -impulse excitation does not fade.
Local response (LR) is an active reaction of the cell to an electrical stimulus, but the state of ion channels and ion transport changes slightly. LO does not manifest itself in a noticeable physiological reaction of the cell. LO is called local excitation, since this excitation does not spread across the membranes of excitable cells.
What does a violation of repolarization processes on the ECG mean in adults?
Every person knows: his health and life expectancy largely depend on how well his heart works. Therefore, if in an adult’s ECG transcript, instead of the word “normal,” the entry “impaired repolarization processes” appears, then he begins to feel anxious. What does such a verdict mean and how dangerous is it?
What does a violation of repolarization processes on an ECG indicate? In adults, this can be either a normal option that does not require medical attention or a warning about a serious pathology. Let's try to describe the essence of the phenomenon in simple language.
The heart's activity is based on the alternation of excitation (depolarization) and relaxation (repolarization). The functioning of this organ is controlled by the brain. He sends him electrical impulses. They are picked up by nerve cells and transmitted to the corresponding receptors.
When such a signal passes, the structure of the cell membrane changes at the molecular level - without this, sodium ions simply will not be able to move freely through it. Repolarization is the process of restoring the electrical charge of a cardiomyocyte (muscle cell of the heart) after a nerve impulse has passed through it, causing its excitation.
It occurs in those short moments when the heart rests before the next contraction.
Repolarization disruption can be caused by a number of factors. This phenomenon is often caused by increased physical activity - intense training or simply quickly climbing the stairs. A deviation in the ECG may also appear because the person drank cold water before the test or was nervous.
Signs of repolarization are often found in women during pregnancy and menopause. But heart pathologies (ischemic heart disease, cardiosclerosis), disorders of the nervous system, kidney disease, and hormonal imbalance can also cause such a disorder. Similar deviations sometimes occur while taking adrenergic agonists.
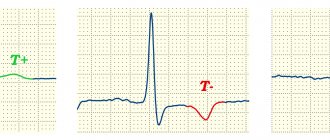
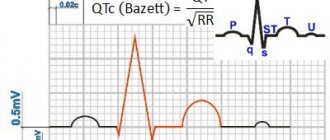
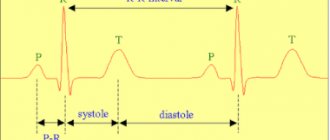
During repolarization, the heart muscle is in a state of complete rest. On the cardiogram this is reflected in the QT segment. Its duration, if everything is normal in a person, is 0.3-0.4 s.
A decrease or increase in the duration of this interval indicates that the repolarization process is disrupted.
However, the diagnostician takes into account not only this indicator - he also evaluates the shape and size of the teeth, the presence of additional waves.
An increase in QT often accompanies congenital pathologies that are associated with gene disorders. An extended QT interval appears on the cardiogram, the T wave changes. Such a deviation can be manifested by the following symptoms:
- sudden rapid heartbeat due to strong emotions or physical overload;
- fainting.
If the QT is short, it is usually due to potassium channel dysfunction. In this case, you can see on the graph that the value of the interval is less than or equal to 0.33-0.35 s. How might the patient feel? Sometimes this does not manifest itself by external signs, but the following warning symptoms may be observed:
- slow heart rate at any time of the day;
- acceleration of the pulse in the form of an attack of atrial fibrillation or tachycardia;
- loss of consciousness.
There is an increased content of calcium and potassium in the blood. In addition, an increase in the acidity of the pH of the internal environment of the body is detected.
Another variant of the disorder is early repolarization.
The main signs of such a deviation, which are visible on the graph, are additional notches and waves on the descending part of the R wave (it is called “pseudo-wave R”), a change in the ST segment, which is expressed in its oblique or horizontal increase above the isoline (this creates a bend, directed downward).
If repolarization affects the entire myocardium, then this negatively affects general well-being, which manifests itself as follows:
- change in heart rate towards increase or decrease;
- stabbing, aching or cutting pain in the heart;
- decreased performance;
- dizziness;
- fainting;
- “quick tears”, irritability.
If a certain area of the heart muscle is affected, then one symptom prevails. So, if a patient’s pulse often jumps, then we can assume that this is a violation of the repolarization processes in the myocardium of the left ventricle.
If there is a disturbance in the repolarization processes in the lower wall of the left ventricle, this is manifested by the fact that when performing work that requires physical effort, the person begins to feel dizzy, spots float before the eyes, and blood pressure rises. Then shortness of breath develops and swelling appears in the legs.
Disruption of repolarization processes in the anteroseptal region, caused by hyperactivity of nerve fibers passing in the anterior wall of the myocardium and the interventricular septum, is often recorded with VSD.
Treatment will depend on how serious the cause of the pathology is. If it cannot be found, then the following treatment regimen is used:
- multivitamin and mineral complexes;
- corticotropic hormones;
- cocarboxylase hydrochloride (restores carbohydrate metabolism, normalizes the functioning of the cardiovascular system);
- in the most severe cases - beta blockers Anaprilin, Panangin.
No one will argue that it is best to have an ideal cardiogram. But if you have discovered violations of the repolarization processes, then you should not make hasty conclusions.
Get an ultrasound of the heart to make sure there is no coronary artery disease, do a stress test. If, according to the results of such a diagnosis, everything is normal, then the worst thing can be ruled out.
Most often, to normalize the condition, it is enough to review your regimen and take vitamins.
So, excitability, in physiology, is the ability of a cell or tissue to respond to a stimulus and generate some kind of impulse. As we found out, cells need a certain charge - polarization - to work. The increase in charge from minus to plus is called depolarization.
After depolarization there is always repolarization. The charge inside after the excitation phase must again become negative so that the cell can prepare for the next reaction.
When the voltmeter readings are fixed at 80, this is the rest phase. It occurs after the end of repolarization, and if the device shows a positive value (greater than 0), it means that the phase reverse to repolarization is approaching the maximum level - the critical level of depolarization.
general characteristics
Action potentials can differ in their parameters depending on the type of cell and even on different parts of the membrane of the same cell. The most typical example of differences is the action potential of the heart muscle and the action potential of most neurons. Nevertheless, the basis of any action potential is the following phenomena:
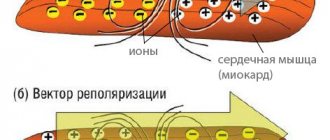
- “The membrane of a living cell is polarized” - its inner surface is charged negatively in relation to the outer one due to the fact that in the solution at its outer surface there is a larger number of positively charged particles (cations), and at the inner surface there is a larger number of negatively charged particles (anions).
- “A membrane has selective permeability” - its permeability to different particles (atoms or molecules) depends on their size, electrical charge and chemical properties.
- “The membrane of an excitable cell is capable of quickly changing its permeability for a certain type of cations, causing a transition of positive charge from the outside to the inside
The first two properties are characteristic of all living cells. The third is a feature of excitable tissue cells and the reason why their membranes are able to generate and conduct action potentials.
The main mathematical model describing the generation and transmission of action potentials is the Hodgkin-Huxley model.
Delayed afterdepolarization and triggered sustained rhythmic activity
frequency leads to a decrease in amplitude. In addition, if a premature action potential during stimulation occurs at a constant frequency, then the subsequent afterdepolarization has a greater amplitude than that observed after a regular action potential. Moreover, the earlier during the main cycle the premature action potential occurs, the greater the amplitude of the premature afterdepolarization.
At a high enough frequency of sustained stimulation or after a sufficiently early premature stimulus, afterdepolarization can reach threshold and produce unstimulated action potentials. The first spontaneous impulse is observed after a shorter interval compared to the duration of the main cycle, since the post-depolarization due to which it arose begins soon after the repolarization of the previous action potential.
Consequently, the spontaneous impulse causes another post-depolarization, which also reaches the threshold level, causing the appearance of a second spontaneous impulse (see Fig. 3.8). This last impulse causes the next afterdepolarization, which initiates the third spontaneous impulse, and so on throughout the duration of the trigger activity.
Triggered activity may cease spontaneously and, if it does, the last unstimulated pulse is usually followed by one or more subthreshold afterdepolarizations. Fig. 3.8. Induction of trigger activity in the atrial fiber of the mitral valve in a monkey. Each fragment shows only the lower part of the action potentials.
The horizontal lines in fragments I and II are drawn at a level of -30 mV, and in fragment III - at a level of -20 mV. fragment IA and 1B: trigger activity resulting from a reduction in the duration of the main stimulation cycle. IA: stimulation cycle duration is 3400 ms; and each action potential is followed by a subthreshold delayed afterdepolarization.
in the occurrence of trigger activity due to premature stimulation. IIIA: A premature impulse (arrow) is produced during the repolarization phase of the afterdepolarization, and the amplitude of the subsequent afterdepolarization increases. IIIB: the premature impulse (large arrow) is followed by a post-depolarization that reaches the threshold (small arrow) and leads to the appearance of a series of trigger impulses [40].
Story
The main provisions of the membrane theory of excitation were formulated by the German neurophysiologist Yu. Bernstein
In 1902, Julius Bernstein put forward a hypothesis according to which the cell membrane allows K ions into the cell, and they accumulate in the cytoplasm. The calculation of the resting potential value using the Nernst equation for the potassium electrode satisfactorily coincided with the measured potential between the muscle sarcoplasm and the environment, which was about -70 mV.
This model was developed in their 1952 work by Alan Lloyd Hodgkin and Andrew Huxley, in which they described the electrical mechanisms responsible for the generation and transmission of a nerve signal in the squid giant axon. For this, the authors of the model received the Nobel Prize in Physiology or Medicine for 1963. The model is called the Hodgkin-Huxley model
In 2005, Thomas Heimburg and Andrew D. Jackson proposed the soliton model, based on the assumption that the signal propagates through neurons in the form of solitons - stable waves propagating along the cell membrane.
Adaptation mechanism
It happens that under certain conditions the depolarizing current does not switch for a long time. This is characteristic of sensory fibers. A gradual, long-term increase in such current above the norm of 50 mV leads to an increase in the frequency of electronic pulses.
In response to such signals, the conductance of the potassium membrane increases. Slower channels are activated. As a result, the nervous tissue becomes capable of repeated responses. This is called nerve fiber adaptation.
During adaptation, instead of a large number of short signals, cells begin to accumulate and release a single strong potential. And the intervals between two reactions increase.