Percussion is the main clinical method for determining the boundaries of the heart and vascular bundle, their size and position. When percussing over the area of the heart, a dull sound occurs, since the heart is a muscular organ. But the heart is surrounded on both sides by the lungs and partially covered by them, therefore, when percussing over this part, a dull sound occurs, that is, relative dullness of the heart
, the definition of which corresponds to the true size of the heart.
Dullness, which is determined by percussion over the area of the anterior surface of the heart not covered by the lungs, is called absolute dullness of the heart.
and is formed by the right ventricle.
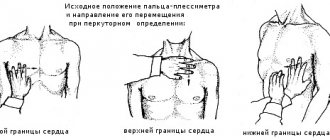
The procedure for performing cardiac percussion.
First, the boundaries of the relative dullness of the heart, the configuration of the heart are determined and its transverse size is measured, then the boundaries of the absolute dullness of the heart, the vascular bundle and its dimensions are determined.
General rules for cardiac percussion.
(1) the position of the patient - sitting or standing, in severe patients - lying down;
(2) mediocre finger-to-finger percussion is used;
(3) the force of percussion when percussing the boundaries of relative dullness is quiet, absolute dullness is quiet;
(4) percussion from clear pulmonary sound to dull when determining the boundaries of relative dullness, and from clear pulmonary sound to dull when determining the boundaries of absolute dullness;
(5) when a change in percussion sound is obtained, the border is marked along the outer (facing the lungs) edge of the pessimeter finger;
(6) the pessimeter finger is installed parallel to the desired boundaries. Determination of the boundaries of relative dullness of the heart.
The right, upper and left borders of the heart are distinguished. When determining the relative dullness of the heart, the right border is first determined, having previously determined the lower border of the right lung along the midclavicular line. Then they rise one intercostal space above (IV) and percussion from the midclavicular line towards the heart until the transition of a clear pulmonary sound into a dull one, while the pessimeter finger is positioned vertically. Normally, the right border is located along the right edge of the sternum or 1 cm outward from it in the 4th intercostal space. The left border of the relative dullness of the heart is determined in the intercostal space where the apex beat is previously palpated. In this case, the pessimeter finger is placed vertically outward from the apical impulse and moved inward. If the apical impulse is not palpable, percussion is performed in the 5th intercostal space from the anterior axillary line to the right. Normally, the border of relative dullness of the heart is located in the 5th intercostal space 1-1.5 cm medially from the midclavicular line.
When determining the upper limit of the relative dullness of the heart, percussion is carried out to the left of the clavicle down between the sternal and parasternal lines, the pessimeter finger is located parallel to the desired border. Normally, the upper border is located on the third rib.
Having determined the boundaries of the relative dullness of the heart, its transverse size is measured. To do this, use a ruler to measure the distance from the extreme points of relative dullness of the heart to the anterior midline. Normally, the distance from the right border of relative dullness (4th intercostal space) to the anterior midline is 3-4 cm, from the left (5th intercostal space) - 8-9 cm, the sum of these values is the transverse size of the heart (11-13 cm ).
The limits of relative and absolute dullness of the heart are normal
| borders of the heart | relative dullness | absolute stupidity |
| right | 4th intercostal space on the right edge of the sternum | 4th intercostal space on the left edge of the sternum |
| top | 3rd rib on the left | 4th rib on the left |
| left | 5th intercostal space 1-1.5 cm medially from the midclavicular line | 5th intercostal space 1-1.5 cm medially from the border of relative dullness or coincides with it |
From a diagnostic point of view, a shift in the boundaries of the relative dullness of the heart and a change in its transverse dimensions are important.
Shift of the borders of relative dullness associated with extra-cardiac causes (1) the border of relative dullness of the heart shifts upward and to the sides (horizontal position of the heart) with a high diaphragm (hypersthenic body type, flatulence, significant ascites), the transverse size of the heart increases;
(2) the boundaries of the relative dullness of the heart shift downward with a simultaneous decrease in the transverse size when the diaphragm is low (asthenic body type, splanchnoptosis) - vertical position of the heart;
(3) when the body position changes, the boundaries of the relative dullness of the heart shift: in the position on the left side by 3-4 cm to the left, on the right side - by 1.5-2 cm to the right;
(4) in the presence of exudate or gas in the pleural cavity, or a mediastinal tumor, the boundaries of the relative dullness of the heart are shifted to the side opposite from the lesion; with obstructive atelectasis of the lung, adhesions between the pleura and mediastinum - in the direction of the lesion.
Shift of the borders of relative dullness associated with cardiac causes (1) shift of the border of relative dullness to the right is caused by expansion of the right atrium or right ventricle with insufficiency of the 3-leaf valve, narrowing of the mouth of the pulmonary artery, with diseases accompanied by pulmonary hypertension, mitral stenosis;
(2) a shift of the border of relative dullness to the left occurs with dilatation and hypertrophy of the left ventricle with hypertension, aortic heart defects, atherosclerosis, aneurysm of the ascending aorta, etc.;
(3) a shift of the border of relative dullness up and to the left is caused by a significant expansion of the left atrium with mitral stenosis, mitral valve insufficiency;
(4) a shift in the border of relative dullness in both directions (“bull’s heart”) can be due to several reasons: damage to the heart muscle due to myocarditis, myocardiosclerosis, dilated cardiomyopathy; simultaneous enlargement of the left and right ventricles and left atrium with combined valvular heart defects; when fluid accumulates in the pericardial area (exudative pericarditis), the shape of dullness resembles a triangle or trapezoid, with the base facing downward;
Reducing the size of relative dullness
occurs with prolapse of the diaphragm, emphysema, pneumothorax. In such cases, the heart not only moves downwards, but also takes a more vertical position - a hanging or drip heart.
The right border of absolute dullness is determined by placing a pessimeter finger vertically in the 4th intercostal space outward from the border of relative dullness and moving it to the left until a dull sound appears (use the quietest percussion). Normally, it is located along the left edge of the sternum.
The left border of absolute dullness is determined by the 5th intercostal space. The pessimeter finger is placed slightly outward from the left border of relative dullness and moved inward until a dull sound appears. Normally, the left border of absolute dullness is located 1-1.5 cm inward from the border of relative dullness or coincides with it.
To determine the upper limit of absolute dullness, the finger-pessimeter is placed outward from the upper limit of relative dullness, moving it down between the sternal and parasternal lines. Normally it is located on the 4th rib.
An increase in absolute dullness of the heart in healthy people is observed with a high position of the diaphragm. At the moment of deep exhalation, when the upper part of the body is tilted forward, the anterior edges of the lungs shift outward, which increases the area of absolute dullness of the heart.
Changes such as pneumosclerosis, obstructive atelectasis, and adhesions lead to an increase in the absolute dullness of the heart due to a shift in its boundaries towards the lesion. If there is liquid or gas in the pleural cavity, the boundaries of absolute dullness of the heart shift to the side opposite to the lesion. An increase in the limits of absolute dullness of the heart can also be due to hypertrophy and dilatation of the right ventricle.
A decrease in the absolute dullness of the heart under physiological conditions is detected with a deep breath. Extracardiac causes include pulmonary emphysema, an attack of bronchial asthma, and a low position of the diaphragm (splanchnoptosis).
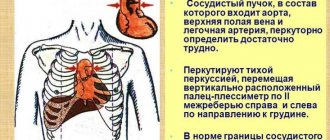
Determination of the boundaries of the vascular bundle.
The vascular bundle is formed by the superior vena cava and the aortic arch on the right, and the pulmonary artery on the left.
The boundaries of the vascular bundle are determined in the 2nd intercostal space by quiet percussion. The pessimeter finger is placed in the second intercostal space on the right along the midclavicular line parallel to the expected dullness, quietly percussing, and gradually moving it towards the sternum until a dull sound appears. The boundary is marked along the side of the finger facing the clear sound. Percussion is performed on the left in the same way. Normally, the diameter of the vascular bundle is 6 cm.
Expansion of dullness of the vascular bundle can be observed with tumors of the mediastinum, enlargement of the thymus gland. An increase in dullness in the second intercostal space to the right occurs with expansion of the aorta, to the left - with expansion of the pulmonary artery.
Determination of the boundaries of relative cardiac dullness
When determining the boundaries of relative dullness of the heart, the right boundary is first established, then the left, and then the upper.
To identify the right border of relative cardiac dullness
along the right midclavicular line, the upper limit of absolute dullness of the liver (or the lower limit of the lung) is established, which is normally located in the VI intercostal space (Fig. 39, a). After this, going up to the IV intercostal space (to get away from hepatic dullness masking cardiac dullness), the pessimeter finger is placed parallel to the desired border and moved towards the heart along the IV intercostal space (Fig. 39, b). A change in percussion sound from clear pulmonary to dull will indicate reaching the limit of relative dullness of the heart. It should be noted that the pessimeter finger should be moved a short distance each time so as not to miss the boundaries of cardiac dullness. The first appearance of dullness indicates that the inner edge of the finger has crossed the border and is already within the location of the heart. The right border is marked along the outer edge of the finger, facing the clear percussion sound. It is formed by the right atrium and is normally located in the fourth intercostal space, protruding 1-1.5 cm beyond the right edge of the sternum.
Rice.
39. Determination of the limits of relative dullness of the heart: a - preliminary stage (establishing the upper limit of absolute dullness of the liver); b, c, d - definition of the right, left and upper boundaries, respectively; d - dimensions of the diameter of the relative dullness of the heart. Before establishing the left border of relative cardiac dullness
it is necessary to determine the apex impulse (see Fig. 38), which serves as a guide. If it cannot be detected, percussion is performed in the 5th intercostal space starting from the anterior axillary line towards the sternum. The plessimeter finger is placed parallel to the desired boundary and, moving it, percussion blows of medium strength are applied until dullness appears. The mark of the left border of relative dullness is placed along the outer edge of the pessimeter finger, facing the clear percussion sound. Normally, it is formed by the left ventricle, is located in the 5th intercostal space at a distance of 1-1.5 cm medially from the left midclavicular line (Fig. 39, c) and coincides with the apical impulse.
When determining the upper limit of relative cardiac dullness
(Fig. 39, d) a finger-pessimeter is placed near the left edge of the sternum parallel to the ribs and, moving it down along the intercostal spaces, blows of medium force are applied until dullness appears. A mark is placed along the upper edge of the pessimeter finger, facing the clear percussion sound. The upper limit of the relative dullness of the heart is formed by the contour of the pulmonary artery and the appendage of the left atrium and is normally located on the third rib along the left parasternal line.
Normally, the distance from the right border of relative dullness to the anterior midline is 3-4 cm, and from the left - 8-9 cm. The sum of these distances (11-13 cm) represents the diameter of the relative dullness of the heart (Fig. 39, e) .
The limits of relative cardiac dullness may depend on a number of factors, both extracardiac and cardiac in nature. For example, in people of asthenic physique, due to the low position of the diaphragm, the heart takes a more vertical position (a hanging “drip” heart) and the limits of its relative dullness decrease. The same is observed with prolapse of internal organs. In hypersthenics, due to the opposite reasons (higher position of the diaphragm), the heart takes a horizontal position and the limits of its relative dullness, especially the left one, increase. During pregnancy, flatulence, and ascites, the limits of relative dullness of the heart also increase.
The shift in the boundaries of the relative dullness of the heart, depending on the size of the heart itself, occurs primarily due to the increase (dilatation) of its cavities and is only to some extent determined by the thickening (hypertrophy) of the myocardium. This can happen in all directions. However, significant expansion of the heart and its cavities is prevented forward by the resistance of the chest wall, and downward by the diaphragm. Therefore, expansion of the heart is possible mainly backwards, upwards and to the sides. But percussion reveals only expansion of the heart to the right, up and to the left.
An increase in the right border of the relative dullness of the heart is most often observed with expansion of the right ventricle and right atrium, which occurs with tricuspid valve insufficiency and narrowing of the mouth of the pulmonary artery. With stenosis of the left atrioventricular orifice, the border shifts not only to the right, but also upward.
A shift of the left border of the relative dullness of the heart to the left occurs with a persistent increase in blood pressure in the systemic circulation, for example with hypertension and symptomatic hypertension, with aortic heart defects (aortic valve insufficiency, aortic stenosis). With aortic defects, in addition to the displacement of the left border of the relative dullness of the heart to the left, it also shifts down to the VI or VII intercostal space (especially with aortic valve insufficiency). A shift of the left border of relative dullness to the left and up is observed with bicuspid valve insufficiency.
Rice. 40. Normal (a), mitral (b) and aortic (c) configurations of the heart.
To determine the configuration of the heart, percussion is performed sequentially in each intercostal space: to the right of IV and above II, to the left of V and above - to II. In this case, the pessimeter finger is positioned, as usual, parallel to the expected dullness. The percussion blow should be of medium strength. The points obtained during percussion are connected to each other and, thus, the configuration of the heart is revealed (Fig. 40, a). It may vary depending on the nature of his pathology. Thus, with mitral heart defects (mitral valve insufficiency, mitral stenosis), the heart acquires a “mitral configuration” (Fig. 40, b). Due to the expansion of the left atrium and left ventricle, the waist of the heart is flattened due to an increase in the size of the left atrium. With aortic defects (aortic valve insufficiency, narrowing of the aortic opening), with pronounced forms of hypertension, the heart, as a result of isolated expansion of the left ventricle, acquires an “aortic configuration” - the appearance of a “boot” or “sitting duck” (Fig. 40, b). In the case of combined and combined defects, all parts of the heart may enlarge. When there is a very sharp displacement of the boundaries of the heart in all directions, it is called “ bull”
».
From 3:11 definition of the boundaries of relative dullness of the heart: