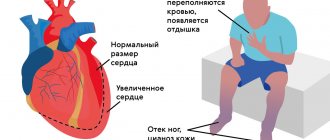
Causes of an enlarged heart
The weight of an average man’s heart is 332 grams, a woman’s – 253. It is considered normal if the weight of the organ varies within these limits.
As for the sizes, they are usually correlated with a person’s fist. For an organ to function normally, it is very important that all its parts (atria, ventricles) are normal, or more precisely, the thickness of their walls, length and width as a whole.
What to do if fluorography (x-ray, ultrasound) showed that the heart is enlarged and dilated?
How dangerous is it to literally have a big heart? And as a result of what can the organ become larger? Let's figure it out in order.
The most important reasons why the heart is larger than normal in a fluorography image include:
- great physical activity;
- diseases.
In people who engage in heavy physical labor every day, as well as in professional athletes, the heart also works harder: it is forced to beat more often and pump blood faster.
This leads to the fact that there are often more heart muscle cells and they grow. As a result, the weight of the organ and its size increase.
If physical activity in the future is moderate, an enlarged heart for this reason does not pose a health risk.
If a person subjects his body to excessive stress for a long time, then it is possible to develop a pathology such as a hypertrophied heart, which is already fraught with serious complications and even life-threatening.
The reason that the heart is enlarged in size can be diseases of the cardiovascular system (coronary diseases: for example, hypertension, coronary disease) and the heart itself (viral, inflammatory diseases), as well as heart defects.
So, if there is a defect and the organ is unable to function normally in order to properly supply the entire body with blood, the organ can enlarge.
What is cardiac radiography?
X-ray of the heart is a fairly old research method and is to a certain extent inferior to some modern diagnostic procedures. However, to this day, radiography is quite informative. It allows you to quickly and accurately find out the condition of the heart chambers and great vessels. You can also obtain data on the contractility of the organ. Heart disease can be detected without radiography; it is often prescribed as an adjunct. X-rays of the heart are possible in both public and private clinics. This diagnostic method is very common.
Coronary diseases
Hypertension is the most common cause of heart enlargement.
This is explained by the fact that due to increased blood pressure, the organ is forced to pump large volumes of it and work in enhanced mode.
This causes the heart muscles to enlarge and the organ itself to expand.
If a person has ischemia, the heart muscle cells constantly do not receive enough nutrients, as a result of which they degenerate, and connective tissue appears in their place.
The latter, unlike muscle tissue, is not capable of contraction; as a result, the organ cavities become deformed and increase in size.
What to do if an x-ray showed that the organ is enlarged, and the cause of this phenomenon is a disease of the cardiovascular system?
The answer to this question is simple and obvious - treat the root cause and return the organ to normal limits.
If a patient is diagnosed with hypertension, he is usually prescribed pharmaceuticals that lower blood pressure. The latter helps restore the normal size of the organ.
A patient with hypertension or coronary artery disease who has been diagnosed with an enlarged heart must take medications.
The fact is that despite the increased size of the organ, a large heart performs its most important function - pumping blood - much worse, which means that human organs and systems do not receive the nutrients they need - heart failure develops, and the whole body suffers.
That is, returning the organ to its normal size helps prevent heart failure, which in some cases can simply save a person’s life.
Big heart of a man
Simon, what does a man's big heart mean to you?
Simon Matskeplishvili:
“A man with a big heart” - who doesn’t want that to be said about him? This is the name given to kind, sympathetic people who can always understand and help, who know how to sympathize with the pain of others, who sincerely rejoice in the happiness of other people, who give a good mood and share the warmth and light of their soul with everyone.
I deliberately gave such a long and exclusively positive definition of a “big heart” in order to contrast it with a medical, namely cardiological, “look from the outside.” After all, for doctors, an enlarged heart in a patient is a serious problem.
This issue is especially relevant from the perspective of men’s health, which in our country requires close attention. Opening the congress in Sochi, the President of the Russian Society “Male and Reproductive Health”, Academician Armais Kamalov, presented his vision of the problem. He said that “for the modern man, the desire to increase life expectancy should not be determined by the fact that he will live longer in old age, but by the fact that old age should come much later.” Well, ancient Chinese wisdom generally says that “The trick of life is to die young, but to do it as late as possible.”
You may ask: why exactly men’s health and “what are women to blame for?” I will answer, of course, they have nothing to do with it. But... Firstly, Russian men live 13 years less than women. And, secondly, despite the presence of a large number of programs for the protection of maternal and childhood health in our country, there is no unified state program for the protection of men’s health. Well, since they say that in every joke there is only a part of the joke, then the statement “the weaker sex is actually the male”, by and large, is true. It is very important that the forum involved an exchange of experience between specialists in various fields. Moreover, a separate meeting was devoted to interdisciplinary problems of men's health.
At which you gave a presentation...
Simon Matskeplishvili:
In addition to me, a cardiologist, endocrinologists, somnologists, gynecologists and even psychiatrists spoke. And they agreed that the thesis “Take care of men” is more relevant than ever.
What is the problem with a “big heart”?
Simon Matskeplishvili:
An increase in its size indicates some kind of trouble. Moreover, this is not necessarily a heart disease. For example, among professional athletes we often observe this phenomenon, which develops in response to excessive physical activity. That is why leaving high-performance sports requires mandatory medical support and observation, with careful rehabilitation and a gradual transition to a “less athletic life.” Exactly the same way we rehabilitate truly sick people.
But, unfortunately, heart enlargement most often develops as a result of heart diseases, which can have completely different causes and manifestations. Hypertension, or increased blood pressure, prevails here. Since in this condition the heart has to pump blood under increased load, the volume of muscle tissue increases, just like with physical exercise. When working “under pressure,” the heart muscle gradually thickens and leads to an increase in the size of the heart itself. In the future, this can lead to a deficiency of nutrients and oxygen, the increased need for which cannot always be compensated by the body.
Another fairly common cause of heart enlargement is cardiomyopathy. This is a disease in which dystrophy of the heart muscle occurs, its thinning and significant expansion of the cavities of the heart. The pathology can be hereditary, but often occurs as a result of heart damage from viruses or, for example, excessive alcohol consumption. The heart can also enlarge with long-term arrhythmia, diseases of the heart valves, or after a heart attack.
“Big heart” is always scary...
Simon Matskeplishvili:
The thing is that this condition necessarily leads to the development of heart failure. And failure is the final outcome of almost all heart diseases, the mortality rate from which significantly exceeds that from all types of malignant neoplasms. After all, as they say, everyone is afraid of dying from cancer, but they die from heart failure. That is why diseases of the cardiovascular system must be treated at the earliest stages, before irreversible changes occur. The most effective measure to reduce mortality from them is prevention. Yes, a healthy lifestyle imposed on everyone, giving up bad habits, regular physical activity, proper diet and sleep. As academician Yuri Buziashvili says, and one cannot but agree, 320 out of 365 days a year we must take care of our health in order to be able to allow ourselves to relax in the remaining 45 days.
Back in 2002, one well-known Russian newspaper asked me to answer a reader’s question: “Is it possible to continue sexual activity after a heart attack?” I, unaware of the consequences, gave a detailed answer in which I said that, firstly, of course, it is possible and, secondly, we carry out certain studies that allow us to accurately answer this question for each individual patient and give him recommendations how to make this process safer. The very next day, the corridor in front of my office was filled with young and not so young men. I realized how relevant this problem is. Let me give you a simple example. In Great Britain, more than 100 thousand married couples were surveyed: what do they consider the main condition for a normal family life, what is important for a happy marriage? So, honesty and respect between spouses came first and second. And the third is sexual relations. Left behind were income, everyday and religious problems. And even children.
But the whole point is that men with heart disease are simply afraid to continue or resume this very sexual activity. And we, cardiologists, help them with this very little. It is cardiologists, and not urologists or andrologists, to whom they mainly turn. A recent Dutch study of nearly 1,000 cardiologists found that only 3 percent—31 in total—discussed sexual activity with their patients. “The patient didn’t ask”, “There was no time”, “I was shy”... These are the explanations received from cardiologists, among many other reasons that prevent the solution of the most important task for men. What can we say about our country, in which the majority of cardiologists are women, and the majority of patients are men. And they expect the doctor himself to start the discussion, they are worried, they are afraid. Men rarely go to doctors in general. And the most common reason for visiting a cardiologist: my wife forced me to.
But maybe the myths, of which there are many around this topic, are also getting in the way?
Simon Matskeplishvili:
There are many myths. For example, this: sex leads to overload of the cardiovascular system. In fact, in terms of physical activity, it is no higher than riding a bicycle or ironing clothes. We often say: if a patient can climb to the 2-3 floor without problems and quickly, then he will not have problems with sex. Or another myth: sex can cause a heart attack or even death. Indeed, there is a small risk of cardiac complications when sexual activity is resumed after a myocardial infarction. But with normal rehabilitation, it does not exceed this risk in completely healthy men who do not suffer from any heart disease.
According to global data, at least 50% of deaths from heart attacks in men occur without what they consider to be a cardiovascular disease. And here I would like to say about the most important thing. Many men suffer from so-called erectile dysfunction, or, as it is often called, sexual weakness, or impotence. So, for a man under 55 years of age with erectile dysfunction without the presence of diseases of the cardiovascular system, the risk of dying from an acute heart attack is 50 (!!!) times higher than for his peer with normal sexual function.
If the patient can quickly climb to the 2-3 floor, then he will not have problems with sex
Moreover, the so-called third Princeton consensus, adopted in 2012, states: “A man with erectile dysfunction without clinical manifestations of cardiovascular disease is a serious cardiac patient.” The bottom line is that the cause of both erectile dysfunction and fatal heart attacks is most often the same process, which manifests itself in the form of impaired sexual function 3-4 years before it leads to serious heart disease. In other words, nature gives us one of the best signals that should force both doctors and patients to pay serious attention to identifying hidden problems and successfully preventing dangerous complications. So the expression that the way to a man’s heart is through his stomach can also be considered a myth. In a cardiological sense, this path lies through a completely different organ.
What is the conclusion?
Simon Matskeplishvili:
Let our men have a “big heart” only in a figurative sense. So that everyone feels good and calm next to them, and let their “fiery engine” remain at normal sizes for many years.
Non-coronary diseases
Another fairly common cause of an enlarged heart is inflammatory processes affecting muscle tissue (carditis), primarily rheumatic carditis.
So, if a person has suffered a serious infection such as tonsillitis or scarlet fever, complications (rheumatism) can also affect the most important organ that transports blood.
In this case, the muscle loses its elasticity, and the ventricles are overstretched, as a result of which the size of the organ can increase several times, and its functionality, accordingly, will decrease several times.
In this regard, timely treatment of rheumatic carditis is very important. To date, drugs have been developed to completely eliminate streptococcal infections and prevent overstretching of the heart.
If therapy is not followed, the person may die. In addition, being a carrier of streptococcus, the patient infects others.
Endocarditis is an inflammatory disease that affects the internal cavity of the heart and its valves.
Endocarditis in an advanced stage causes expansion of the organ, loss of muscle elasticity and ability to contract. The disease requires immediate treatment.
Myocarditis is a consequence of viral infections, accompanied by arrhythmia and shortness of breath, and heart failure may occur. Video:
In this regard, a patient with myocarditis needs immediate medical attention and supportive care.
Chronic alcohol consumption can cause cardiomyopathy and cardiac dystrophy, as a result of which the heart cavities expand and the heartbeat rhythm changes significantly.
Also, patients with alcoholism, as a rule, have high blood pressure - another factor that contributes to the modification of the heart muscle.
If a person recovers from alcoholism and stops drinking alcohol, and if he has hypertension, takes blood pressure-lowering medications, after some time the organ will restore its normal size.
Thus, if a fluorography image reveals an increase in the size of the heart, you should immediately contact a specialist, find out the cause of the pathological changes and, if necessary, begin therapy: the problem is solvable in most cases.
Symptoms, diagnosis and treatment for cardiomegaly
Have you been struggling with HYPERTENSION for many years without success?
Head of the Institute: “You will be amazed at how easy it is to cure hypertension by taking it every day.
The heart is one of the most important organs of the human body. One of the most dangerous symptoms of diseases that affect not only the cardiovascular system, but also other organs, is an enlarged heart (cardiomegaly). This can manifest itself in different ways: in one case, the patient has symptoms characteristic of diseases of the heart muscle, in another, he lives for a long time and does not even suspect the presence of pathology.
Causes of pathology
The most important organ that ensures the vital functions of the entire body consists of 4 chambers: two ventricles and two atria. There are two sections of the heart - right and left, each of which includes an atrium and a ventricle. Normally, the boundaries of the heart change throughout life. People who play sports experience an increase in its size, which is considered a completely natural process and does not cause any cause for concern.
The weight of a man's heart is 332 grams, a woman's - 253 grams. An enlarged heart is observed when the myocardium grows and (or) expands its cavity. Most often, the organ enlarges to the left, which is observed in many diseases: hypertension, stagnation of blood in the systemic circulation, heart defects. Enlargement of all parts of the organ is dangerous. This condition is called “bull’s heart”, and only surgical intervention can improve a person’s quality of life.
The reasons influencing the enlargement of the organ are:
- Hypertonic disease. An increase in pressure leads to changes in the cardiovascular system: vascular tone increases, the thickness of the muscle layer increases, and the systemic circulation suffers.
- Coronary heart disease: angina pectoris, myocardial infarction. Oxygen starvation of the organ tissues occurs with the death of their cells and replacement with connective tissue, which leads to an increase in the size of its left section.
- Rheumatic heart disease. It is a consequence of tonsillitis (frequent tonsillitis). Rheumatic disease is manifested by an inflammatory process occurring in the tissues of the organ. As a result, the valves suffer and defects form.
- Myocarditis.
- Renal dysfunction.
- Alcohol abuse. The most common example is alcoholic cardiomyopathy.
- Smoking.
- Acute pericarditis (inflammation of the serous membrane).
- Congenital heart defects.
The presence of pathology in close relatives is considered a risk factor, therefore, under certain conditions, the disease can manifest itself in other family members. A common cause of changes in the heart muscle is an increase in pressure (above 140/90 mm Hg), which has a detrimental effect on the state of the cardiovascular system and in some cases leads to an enlargement of the organ up to the “bull heart”.
Congenital heart disease is of great importance. Today, it is treated in the first years of life, but there are also forms that are discovered only at an older age. An example is non-closure of the interventricular septum. The left ventricle contains oxygen-rich blood (arterial), and the right ventricle contains carbon dioxide (venous).
Normally, the blood does not mix, but with pathology of the interventricular septum, blood flows from the left ventricle to the right. There are different variations in the size of the defect. Improper distribution of blood within the organ leads to its enlargement.
Myocarditis in the daily practice of a doctor (part 2)
00:00
Vladimir Trofimovich Ivashkin , academician of the Russian Academy of Medical Sciences, Doctor of Medical Sciences:
– Next – infectious diseases, since we needed to exclude infectious myocarditis. You see that indicators of viral infections (chlamydia, ureaplasma, trichomonas, mycoplasma, herpes simplex viruses, brucella, and so on) were practically negative. The same applies to cytomegalovirus. Blood was taken repeatedly for bacterial culture (culture) - and not once was a positive culture detected. Consequently, we also rejected the infectious nature of heart pathology.
This possibility of excessive sensitivity to certain drugs is sometimes observed in patients with certain genetic polymorphisms of regulatory mechanisms. In this regard, we conducted genetic studies and found that our patient was heterozygous for angiotensin-converting enzyme. She also turned out to be heterozygous for the first type receptor, angiotensin II.
But despite being heterozygous, the presence of angiotensin-converting enzyme levels was essentially unaffected. It turned out to be within normal limits. Therefore, this heterozygosity for angiotensin-converting enzyme and angiotensin type I receptor for angiotensin II essentially remains outside the brackets. We cannot, in one form or another, link these data to the clinical observations that we have in relation to this patient. Perhaps in the future we will be able to answer this question.
Here is an electrocardiogram from 2010. We do not see electrical alternation here. But what attracts attention is a very pronounced increase in the electrical activity of the left and right parts of the heart. Right leg block. But, what is important: after such a long time, the ST segment elevation in precordial leads V3, V4, V5 remains. This ST segment elevation forces us to continue to pursue our patient's differential diagnosis of what is causing her cardiac decompensation to be so severe.
The left picture shows a chest x-ray from 2008. On the right is an x-ray from 2010. You see some differences. The fluid content in the pleural cavities decreased. The boundaries of the aperture have dropped somewhat. Root stagnation has decreased. However, the heart remains large in diameter. The silhouette of the pulmonary artery and right atrium bulges. Consequently, all radiological signs of congestive heart failure remain. Kerley lines 2 are clearly visible. Our patient has signs of congestive interstitial edema.
04:19
A computed tomography scan of the chest (shown by arrows) shows a fairly significant protrusion in the pleural cavities and large chambers of the heart. Here, using the left atrium as an example, the large left atrium.
During computed tomography of the chest, the patient is positioned on her stomach. She could not lie on her back because she was choking with a cough and did not have enough air. We see signs confirming the presence of interstitial edema, thickening of the interlobular peribronchivascular interstitium. There is no evidence of infiltration of lung tissue.
On an echocardiogram in October 2010, we see signs of enlargement of the chambers of the heart, ventricles, and atria. Left ventricular ejection fraction – 22%. Systolic pressure in the pulmonary artery is 65 millimeters Hg. Art. Experts note an increase in the degree of dilatation of the left atrium, pulmonary hypertension and pressure in the right atrium.
Ultrasound examination of the abdominal cavity confirms signs of right heart decompensation. The portal vein is slightly dilated. And the inferior vena cava is expanded to 32 millimeters. The hepatic veins are dilated to 14 millimeters. No free fluid is detected in the abdominal cavity. Consequently, the presence of right heart decompensation is confirmed.
(Slide show).
In order to finally resolve the issue of the nature of the changes in the myocardium that we encountered, a series of studies were carried out. In particular, the patient underwent perfusion tomoscintigraphy. You see the results of the examination of the apex and anterior wall.
Experts note a massive zone of hypoaccumulation of the indicator, indicating a perfusion defect in the anteroseptal-posterior localization. A conclusion is made about the presence of a sign of large-focal myocardial damage. Essentially, these changes coincide with those changes in the electrocardiogram that we saw in previous electrocardiographic pictures.
07:08
The patient underwent multislice computed tomographic angiography. She put us in a difficult position because it was noted that there was no contrast enhancement in the distal segment of the right coronary artery. The question arose again about the possibility of myocardial infarction suffered by our patient. This required either direct confirmation or denial of this possibility.
(Slide show).
Here is a continuation of this research. In the area of the apex there is a suspicion of the presence of a blood clot. Here we have projected on a diagram the data that we obtained using electrocardiography, echocardiography, scintigraphy and multislice computed tomography. It turns out that the apex, septum and lateral wall of the left ventricle are hypoperfused, that is, damaged.
(Slide show).
The cardiac surgeon consulted our patient and recommended probing of the heart cavities and coronary angiography. The patient underwent coronary angiography. You see that the left type of blood supply to the heart is marked. The anterior interventricular branch is not changed. Noteworthy is the small number of diagonal and septal branches. The trunk of the left coronary artery is not changed. The circumflex branch is also unchanged. Normal picture of the coronary vessels.
(Slide show).
Here is the right coronary artery. You remember that during multislice computed tomography, there was a suspicion of occlusion of the right coronary artery in its distal part. When performing coronary angiography, you see that the coronary artery has smooth contours. Essentially, it is not changed along its entire length, including in the distal sections.
Consequently, we rejected the thromboischemic nature, that is, simply myocardial infarction in this patient. With transesophageal echocardiography, attention is drawn to the hyperechogenicity of the myocardium of the interventricular septum, as well as the pronounced trabecularity of the posterolateral wall of the left ventricle, which allows us to think about myocardial non-compaction syndrome with its infiltration, that is, the possibility of sarcoidosis or amyloidosis. Although, of course, the clinical picture itself does not coincide with the assumption of sarcoid granulomatous or amyloid myocardial damage.
10:17
(Slide show).
The patient underwent magnetic resonance imaging of the heart. It was noted that there is akinesis of the anterior and inferior walls of the left ventricle in the apical and middle segments, the interventricular septum, and the apical segment. Hypokinesis of the interventricular septum in the middle segment, basal segments of the anterior and inferior walls. Increased trabecularity of the apical segment of the lateral wall is noted (without criteria for myocardial non-compactness).
Consequently, we can largely (given the clinical picture) ignore amyloidosis and sarcoidosis. And the data obtained coincide with previous studies on massive myocardial damage in our patient.
Thus, no evidence of space-occupying lesions of the heart or myocardial non-compaction syndrome has been identified. The magnetic resonance image, as experts note, may correspond to myocarditis affecting the left and right ventricles.
(Slide show).
Let's return to the differential diagnosis table. So, we have to guess based on the clinical data that we have. This table, of course, does not completely cover all the symptoms of myocarditis. Only those data that were most clearly and clearly identified in our patient are included here.
The first is ST segment elevation. In what forms of myocarditis is ST segment elevation usually observed? This is either acute hypersensitive eosinophilic myocarditis, or acute (or subacute) necrotizing eosinophilic myocarditis.
What next should we pay attention to? In what forms of myocarditis can we encounter severe myocardial necrosis? In fact, with all forms of myocarditis (infectious, autoimmune, giant cell), very small areas of myocardial necrosis are possible.
But such massive myocardial necrosis, which we assume in our patient, can occur either in acute hypersensitive eosinophilic myocarditis or in acute necrotizing eosinophilic myocarditis.
But if we talk about these two forms, then in acute hypersensitive eosinophilic myocarditis the main clinical picture is rhythm disturbance. Arrhythmia of various kinds characterizes acute hypersensitive eosinophilic myocarditis, occurring with ST elevation. Whereas acute necrotizing myocarditis (or subacute necrotizing myocarditis) is characterized by massive myocardial damage with the development of congestive heart failure.
13:45
Now, if we turn to the rate of myocardial development that characterizes the development of all these adverse consequences, such a subacute course is characteristic of idiopathic giant cell myocarditis and subacute necrotizing myocarditis. In idiopathic giant cell myocarditis, the main clinical form is still severe rhythm disturbances. They determine the course and prognosis of the disease. Whereas in subacute necrotizing myocarditis we are talking about rapid development, the formation of congestive heart failure.
Therefore, based on these criteria (plus a differential diagnosis involving numerous instrumental studies), we finally settled on the possibility that our patient had subacute necrotizing eosinophilic myocarditis, secondary dilated cardiomyopathy, and pulmonary hypertension. Relative insufficiency of the mitral and tricuspid valves. Relatively minor rhythm and conduction disturbances, incomplete blockade of the right leg, and so on. In this case, in our opinion, we were talking about subacute necrotizing myocarditis.
(Slide show).
Naturally, such an unfavorable trend in the decline of contractile function forced us to consult and invite specialists from the Research Institute of Transplantology and Artificial Organs named after Academician Shumakov. We agreed with the director of the Institute, Academician Gauthier. He referred specialists, and the patient was transferred to the Transplantation Institute.
There she underwent a heart transplant and was diagnosed. Postmyocardial cardiosclerosis with dilatation of the heart cavities. Relative insufficiency of the mitral and tricuspid valves, and so on. Our ideas that she suffered from myocarditis coincided.
Unfortunately, we were unable to obtain the results of a histological study that would confirm or reject our idea of the nature of myocarditis. But the mere fact of the coincidence of our clinical diagnosis and surgical diagnosis, plus the presence of slight eosinophilia in peripheral blood and a slight increase in immunoglobulin E, still confirms us in the assumption of the presence of subacute destructive necrotizing myocarditis.
17:08
Further, after heart transplantation, the patient was naturally recommended the necessary medications, which are indicated here.
A year later she is back in our clinic. We see that she feels great. She is still so graceful - she weighs 55 kg, height - 168. Respiration rate - 17. Normal blood pressure. Some tendency to tachycardia is typical.
Here is her electrocardiogram, actually, the cardiogram of the transplanted heart. We see a completely different picture. The echocardiogram shows everything is good and favorable. The sizes of the heart chambers correspond and are not bad. They will tend to the atrium to shrink. Contractile function – ejection fraction of almost 60%.
Most often, surgeons perform transplantation for the following pathologies:
1. Coronary heart disease.
2. Dilated cardiomyopathy.
3. Acquired heart defects.
4. Congenital heart defects.
5. Heart retransplantation.
6. Other pathologies.
Our patient falls into the category of dilated cardiomyopathy as a result of severe necrotizing myocarditis. This is one of the most common forms of indication.
What specific indications for transplantation did our patient have? The drug-refractory end-stage of chronic heart failure in our patient has, of course, already formed. Left ventricular ejection fraction is less than 20%. In our patient it is 15%.
End-diastolic pressure in the left ventricle is more than 25. Our patient also had high end-diastolic pressure. Her cardiac index was less than 2 liters per minute per square meter. Consequently, her heart transplant was performed on time.
What is the forecast? Our patient has been living for a year and a half. The prognosis is good. One-year survival rate - she was included in this group (86%). Three-year – 77%, five-year – 69%. We will hope that our patient will always be in these successful groups. We wish her health and prosperity in her future life. Thank you for your attention.
20:25
Oksana Drapkina : Thank you very much, Vladimir Trofimovich. Questions are already coming in.
Question: Why was this woman not given a myocardial biopsy?
Vladimir Ivashkin : Myocardial biopsy is not an easy procedure. It is advisable to perform it when the condition of the patient allows this procedure.
Our patient experienced progressive cardiac decompensation. Therefore, the large volume of conservative diagnostic studies that have been carried out has convinced us that we are right. We are talking about myocarditis, and not about any other forms. Therefore, in agreement with the transplantologists, we referred the patient. They accepted her, and, you see, everything went well.
I hope this patient has a good life prognosis. First of all, she is a young woman. Secondly, she has no risk factors. You see, she is an elegant woman with normal blood pressure. She has an absolutely clear coronary angiogram (as you looked at), there are no associated diseases. Nothing clouds her future. Let's hope everything goes well.
Oksana Drapkina : Thank you very much, Vladimir Trofimovich. I think there will be more questions. We have finished the section “Lectures, master classes, clinical analysis”.
Symptoms of the disease
Manifestations of cardiomegaly are purely individual. In some cases, symptoms do not occur at all, and a person learns about the expansion of the organ’s boundaries by chance, for example, during fluorography or a doctor’s examination. If the pathology makes itself felt, its manifestations are not much different from the symptoms of diseases of the cardiovascular system. But there are cases when the pathological process develops so rapidly that a “bull’s heart” quickly forms.
Signs include:
- Pain behind the sternum.
- Dizziness, loss of consciousness for no reason.
- Fast fatiguability.
- Shortness of breath with slight exertion.
- Arrhythmia (change in rhythm).
- The appearance of edema (especially in the lower extremities in the evening).
- Cough not associated with respiratory diseases.
Expanding the size of such an important organ of the cardiovascular system entails very dangerous consequences. If the heart rhythm is disturbed, there is a risk of cardiac arrest. The occurrence of noise should be monitored by a doctor, because it indicates a change in the structure of the valves. An enlarged heart affects the quality of the entire cardiovascular system. Over time, there will come a point when the organ cannot pump the required amount of blood, so the risk of developing heart failure increases over the years. If the problem is ignored, then you can get a serious complication - “bull heart” (an increase in the size of the organ to critical).