Cardiac aneurysm (aneurysma cordis) is a limited protrusion of a thinned area of the heart wall. Most often develops as a result of myocardial infarction. Congenital, infectious, traumatic, and postoperative cardiac aneurysms are much less common. Traumatic aneurysms occur due to closed or open heart injuries. This group also includes aneurysms that occur after operations for congenital heart defects.
In the overwhelming majority of cases, cardiac aneurysm is a complication after a myocardial infarction (usually transmural). Up to 25% of heart attack patients may be affected by this disease.
Dangerous complications of chronic cardiac aneurysm are gangrene of the limb, stroke, kidney infarction, pulmonary embolism, and repeated myocardial infarction. When a cardiac aneurysm ruptures, death occurs instantly.
Based on the time of occurrence, aneurysms are divided into acute (1-2 weeks from the onset of myocardial infarction), subacute (3-6 weeks) and chronic. Most often, post-infarction aneurysms are localized on the anterolateral wall and at the apex of the left ventricle; in 50-65% of cases they spread to the anteroseptal region.
Left ventricular aneurysm is diagnosed so often because of the maximum blood pressure in this ventricle. Up to 50% of the surface of the left ventricle may be damaged as a result of the pathological process.
1 Left ventricular aneurysm
Aneurysm of the posterior wall of the left ventricle is observed in 2-8% of patients. Blood clots are often found in the aneurysm cavity, but the incidence of thromboembolic complications is no more than 13%.
Definition:
A cardiac aneurysm is a pathological condition that is accompanied by protrusion of the wall of the heart muscle. It is one of the complications after a myocardial infarction and can develop within several months after its onset. An aneurysm not only negatively affects the functioning of the heart and its contractile functions, but also poses a serious danger to life due to the possibility of sudden rupture.
ARTERIO-VENOUS ANEURYSMA OF THE LUNG
V. D. Stonogin
2nd Department of Clinical Surgery (headed by Professor Timofey Pavlovich Makarenko) of the Central Institute for Advanced Medical Studies on the basis of the Central Clinical Hospital No. 1 of the Ministry of Railways (headed by V. N. Zakharchenko), Moscow, Russia.
The publication is dedicated to the memory of Vasily Dmitrievich Stonogin (1933-2005)
Patient Ch., 37 years old, was admitted to the clinic on June 10, 1970. with complaints of shortness of breath when walking, periodically increasing, sometimes suddenly occurring at rest, periodically suddenly occurring weakness. The patient considers himself to be about 5 years old when the above complaints appeared. An X-ray examination at the place of residence (Tula) revealed a darkening in the left lung and a diagnosis of tuberculosis of the left lung was made. A course of anti-tuberculosis treatment was carried out, but it had no effect. Heredity is not burdened. She grew up healthy. I have had my period since I was 13 years old, had 6 pregnancies, 3 births. Signs of the disease appeared after the last birth.
Objectively: the patient’s general condition is satisfactory, with a correct physique, good nutrition, and slight cyanosis of the lips. The chest is of the correct configuration, both halves participate evenly in the act of breathing, 20 breaths per minute. On percussion there is a clear pulmonary sound over both lungs, on auscultation there is vesicular breathing, no wheezing. Heart sounds are of satisfactory volume, rhythmic pulsation. Pulse 82 per minute, blood pressure 120/80mm/Hg.
X-ray (Fig. 1) on the left in the reed segments reveals an irregular spherical formation measuring 3*3.5*4 cm, dense, homogeneous with clear contours. The interlobar pleura on the left is compacted, the roots are not expanded. The pleural sinuses are free. The heart and aorta are without visible changes.
Figure 1 - Direct radiograph of the chest of patient Ch. A spherical formation in the middle pulmonary field on the left.
Conclusion: the differential diagnosis should be made between a benign tumor and tuberculoma.
Upon consultation with a phthisiatrician, a diagnosis of a retention cyst of metatuberculous origin was made.
In order to clarify the diagnosis of the patient, they tried to perform bronchial sounding to obtain an aspirate directly from the formation and subsequent cytological examination of it, but it was not possible to penetrate the lingular bronchus with the probe (fortunately!).
In the blood: Hb79% (13.2g%), color. indicator 1, er.3600000, l.5300, e.2%, p.3%, p.48%, lymph.39%, mon8%; POP3 mm/hour. Urinalysis is normal. Biochemical blood and urine tests without deviations from the norm. The Mantoux reaction is negative.
Examination of external respiration function: pulmonary volumes are within normal limits, reserve capacity is sufficient, there is no hyperventilation at rest. There is functional tension after the load at the 5th minute of rest.
The ECG shows a vertical electrical position of the heart, indicating diffuse changes in the myocardium. Radioisotope scanning of the lungs: a significant decrease in the accumulation of the isotope in the left lung, a uniform, intense accumulation on the right. Taking into account the radiological data, the duration of the disease, and the lack of tumor growth, it was decided to operate on the patient with a diagnosis of a benign tumor of the uvula, possibly tuberculoma.
On June 24, 1970, the operation was performed under endotracheal anesthesia. The pleural cavity was opened from a lateral approach along the sixth intercostal space. During the inspection, it was discovered that in the area of the uvula, closer to the root, there is a cystic formation, soft to the touch, about 5 cm in diameter. When pressing on it, a blowing noise is felt; after removing it from the formation of the hand, it pulsates. In the region of the lower surface of the reed segments, one of the walls of the formation is located superficially and the contents (blood) are visible through it, which is why the cyst has a dark blue color. The presence of an arteriovenous aneurysm of the lingular artery was established. The remaining parts of the lung are not changed. It was decided to remove the uvula along with the aneurysm. Mediastinotomy was performed. When isolating the vein of the uvula, it was found that 4 venous trunks emerge from the aneurysm.
The veins were sequentially treated, then the lingular bronchus and the artery of the lingular segments. After this, resection of the uvula was performed, immediately after which a contrast agent (diodone) was injected into the preparation through the artery of the uvula. The aneurysm cavity was completed last.
The postoperative period proceeded without complications. 24.VII.1970 The patient was discharged from the clinic in satisfactory condition. Before discharge, in order to exclude arteriovenous aneurysms of the right lung or unrecognized aneurysms of other parts of the left lung, the patient underwent angiopulmonography: no vascular pathology was detected on the right, and the stump of the lingular artery on the left (Fig. 2).
Figure 2 - Angiopulmonogram of the same patient one month after surgery.
The patient was examined 5 months after the operation: she feels well. All previous complaints disappeared. She still works as a milkmaid on a collective farm. Histological examination of the preparation (K. A. Makarova); the uvula measures 10*9*2 cm, the lung tissue is airy, in its middle part there is a cystic formation with a diameter of 2.5 cm, made of a blood clot. The inner surface is smooth and shiny. Microscopically: the cyst wall is represented by a sclerotic vein, in the lumen of the cavity there is a blood clot. In the lymph nodes there is dusting of tissue and hyperplasia of the reticular tissue. Along the periphery of the lung there is emphysema, small foci of atelectasis. The picture corresponds to the clinical diagnosis.
By citing this observation, we wanted to emphasize the importance of angiopulmonography in the differential diagnosis of spherical lung formations. If our patient had undergone pulmonary angiography before the operation, perhaps a diagnostic error would not have occurred.
Despite the undoubted diagnostic value of bronchial sounding, in some cases it can be dangerous. If during bronchial probing it was possible to penetrate into the lingular bronchus, there was a real possibility of causing dangerous bleeding from the aneurysm in our patient. Therefore, in doubtful cases, it is more appropriate to perform this study after angiopulmonography.
Author information:
| Vasily Dmitrievich Stonogin – Associate Professor of the 2nd Department of Surgery at TsOLIU, Head of the Academic Department, Candidate of Medical Sciences. Email |
Text restoration, computer graphics - Sergey Vasilyevich Stonogin.
Any copying of the material is prohibited without the written permission of the authors and editor.
The work is protected by the Federal Copyright Law of the Russian Federation.
Cause
Usually the cause of the formation of a cardiac aneurysm is a heart attack, most often of the left ventricle of the heart. When they talk about the development of myocardial infarction, the damaged parts of the heart are weakened, and under the influence of blood pressure they can bulge. Blood trapped in them forms a blood clot. Aneurysms occur in patients with atherosclerotic cardiosclerosis and cardiosclerosis of other origins. Much less common are aneurysms that arise due to other reasons: infections, injuries, and congenital defects.
Diagnosis of cardiac aneurysm
In 50% of patients, pathological precordial pulsation is detected.
ECG signs are nonspecific - a “frozen” picture of acute transmural myocardial infarction is revealed, there may be rhythm disturbances (ventricular extrasystole) and conduction (left bundle branch block).
ECHO-CG allows you to visualize the aneurysm cavity, determine its size and location, and identify the presence of a parietal thrombus.
The viability of the myocardium in the area of chronic cardiac aneurysm is determined by stress echocardiography and PET .
Using chest x-ray, it is possible to detect cardiomegaly and congestive processes in the blood circulation.
1 ECG - a method for diagnosing cardiac aneurysm
2 ECHO-CG - a method for diagnosing cardiac aneurysm
3 Chest X-ray
ventriculography, MRI and MSCT are also used to determine the size of the heart aneurysm and detect thrombosis of its cavity.
For the purpose of differential diagnosis of the disease from coelomic pericardial cyst, mitral heart disease, mediastinal tumors, probing of the heart cavities and coronary angiography may be prescribed .
Classification
Depending on the time period after myocardial infarction the aneurysm formed, the following forms are distinguished:
- Acute and subacute - develop in the early stages after a heart attack, often complicated by incomplete rupture.
- Chronic - formed after acute due to the replacement of a dead section of the heart muscle with connective tissue. They can be muscular, musculofibrous or fibrous.
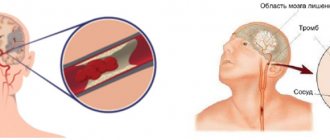
Management of a patient with a ruptured cerebral artery aneurysm
After subarachnoid hemorrhage in a patient in stupor or coma, intracranial pressure may be increased. Therefore, it is necessary to maintain sufficient cerebral perfusion pressure (CPP) while ensuring that mean arterial pressure does not increase excessively. To assess alveolar ventilation in the lungs, the content of gases in arterial blood should be monitored. In case of hypercapnia, the patient requires artificial pulmonary ventilation (ALV). If a subdural or intracerebral hematoma causes an increase in neurological disorders, surgical removal is advisable. During the operation, the neurosurgeon can also remove the found aneurysm from the bloodstream using a vascular clip at its base.
To avoid recurrent hemorrhage, all patients are advised to rest in bed and placed in a quiet, preferably darkened room. To prevent constipation as a result of a sedentary state, which then forces the patient with an aneurysm to push, laxatives are prescribed. At the same time, excessive restrictions on activity can lead to anxiety, so the patient is allowed to read, listen to the radio, and meet with relatives. For severe headaches and pain in the neck, mild sedatives and analgesics are prescribed. Acetylsalicylic acid (aspirin), which has an antiplatelet effect, is not recommended, but paracetamol (acetaminophen) or meperidine and phenobarbital or other sedatives can be used. Excessive prescription of sedatives to a patient with a cerebral artery aneurysm is undesirable, since it complicates the assessment of his initial and possible neurological symptoms.
Epileptic seizures at the time of aneurysm rupture are rare. Minor trembling, twitching, and an extended posture in the patient often accompany loss of consciousness, probably due to a sharp increase in intracranial pressure. Because generalized seizures increase the risk of aneurysm re-rupture, phenytoin (300 mg daily) or phenobarbital (30 mg three times daily) is sometimes given as preventive therapy.
Steroid medications help reduce pain in the head and neck caused by the irritating effect of blood in the subarachnoid space. There are no data on their effectiveness in cerebral edema, sometimes observed in patients immediately after subarachnoid hemorrhage.
Symptoms
Symptoms of acute cardiac aneurysm are weakness, shortness of breath, fever, pulmonary edema, sweating, heart rhythm disturbances, and swelling of the veins in the neck. During the transition to the subacute form, symptoms of coronary insufficiency quickly develop.
With chronic cardiac aneurysm, signs of cardiovascular failure are observed: edema, angina attacks, rhythm disturbances. Complications of the disease can be thromboembolic syndrome with damage to peripheral vessels and arteries of the brain. If you experience such signs, immediately contact the cardiology center.
When an acute aneurysm ruptures, death occurs almost instantly. In this case, the patient experiences severe pallor, hoarse, difficult breathing, cold sticky sweat, congestion of the neck vessels, and cold extremities.
Treatment of cardiac aneurysm
It is impossible to eliminate a cardiac aneurysm using conservative treatment methods, and when the first signs of heart failure appear, the question of surgery is raised. The main treatment method for cardiac aneurysm is surgical excision and suturing of the defect in the heart wall. In some cases, the aneurysm wall is strengthened using polymer materials.
In the preoperative period, cardiac glycosides, anticoagulants, antihypertensive drugs, oxygen therapy, and oxygen barotherapy are prescribed. Patients are advised to strictly limit physical activity.
The cardiology department of MedicCity has all the necessary equipment to carry out comprehensive diagnostics of a wide range of cardiac diseases. Reception is conducted by highly qualified cardiologists who have completed professional internships in Russia and abroad.
Which method of diagnosing a fusiform aneurysm to choose: MRI, CT, angiography
Selection method
- DSA (CT angiography, MR angiography).
Is MSCT of cerebral vessels informative for fusimorphic aneurysm?
- Tubular hyperdense structure in a typical location
- Fusiform aneurysm of the basilar artery: prepontine localization
- Fusiform aneurysm of the middle cerebral artery: Sylvian fissure
- Calcification of the vessel wall
- Significant enhancement after CS injection (CT angiography).
What will MRI images of the brain show for a fusiform aneurysm?
- In addition to other factors, the signal depends on the speed and direction of blood flow and on the presence and “age” of blood clots.
In what cases is angiography of cerebral vessels performed for an aneurysm?
- Allows you to visualize only the free lumen, but not thrombosed areas.
Risk group
Doctors are conflicted about which people are more susceptible to aneurysms. It is believed that AVA is a congenital pathology that begins in the womb. The disease is rare (what a pulmonary artery aneurysm is is known to 5-6 people among a population of 200 thousand).
Despite the congenital factor, the disease does not manifest itself at an early age (it is diagnosed in a small number of patients). People aged 20 to 45 years are at risk - they are admitted to hospitals with different manifestations.
Aneurysms affect women and men equally. A single form of AVA is common in patients (20% of cases are attributed to aneurysms).
The proper development of the cardiovascular system in the fetus is influenced by the mother’s way of life: her habits, the environment. At risk are children who were exposed to chemicals in the womb, both from the environment and drugs (the woman suffered from addiction during pregnancy).
There are cases when an aneurysm is preceded by hereditary factors. If there were similar precedents in the family, then the risk of pathology in younger relatives is higher than in others. After birth, AVA begins due to cirrhosis, stenosis and other dangerous pathologies. An arteriovenous aneurysm occurs.
A pulmonary aneurysm is preceded by a congenital heart defect. Patients with pathology should pay attention to their health, just like those who have had experience in treating syphilis - one reason for the appearance of vascular anomalies.
Cerebral aneurysm causes of occurrence
The final genesis of the arterial aneurysm is not clear. Some argue that this is a congenital phenomenon - an undeveloped, blindly ending short vessel. Others say that this is an acquired condition - a protrusion in a weak spot of the hemangion - the structural unit of the vessel, between the circular areas of smooth muscle. As a result of the impact of the shock wave, this protrusion gradually grows. The formation of de-novo aneurysms confirms the presence of new aneurysms during control angiography in already operated patients. There is also an autoimmune inflammatory theory of the occurrence of arterial aneurysms, which is being actively developed at the University of Helsinki with the participation of Professor J. Hernisniemi. Thus, he believes that eventually a drug will be developed that can treat and prevent aneurysmal disease (he considers himself the last of the Mohicans - i.e. "aneurysmal" surgeons).
Risk factors for developing aneurysms
The development of aneurysms is predisposed by the loss of elasticity and strength of the vessel wall. Weakness of the vascular wall may be due to congenital characteristics or the influence of external factors. The main reasons for the development of the disease:
- atherosclerosis - formation of cholesterol plaques;
- inflammation of the aortic wall (occurs with traumatic injury, syphilis, fungal infection);
- autoimmune diseases;
- congenital pathologies of connective tissue (cystic fibrosis, Marfan syndrome);
- trauma during diagnostic and therapeutic procedures (coronary angiography, heart surgery).
Diagnosis and treatment of arterial aneurysms in Medical
When should you see a doctor?
You should contact a cardiologist or cardiovascular surgeon if:
- the attending physician suspects an aneurysm;
- during an examination for another reason, a pathological dilatation of the artery was discovered;
- there are characteristic symptoms.
There are two tactics for managing patients: dynamic observation (for small sizes, asymptomatic course, minimal risk of complications), surgical treatment.
Observation is carried out under x-ray control. To reduce the risk of possible complications, antihypertensive and anticoagulant therapy and cholesterol reduction are carried out.
General information about arterial aneurysms
An aneurysm is a local expansion of a vessel with gradual thinning of its wall. The process is irreversible; over time, under the influence of blood flow pressure, the protrusion only increases and, one day, may rupture. This leads to internal arterial bleeding. Without timely medical attention, a ruptured aneurysm leads to death.
Other possible complications include: thrombosis, thromboembolism (when a blood clot breaks off and clogs other vessels), infection of the aneurysm.
Cerebral aneurysm - consequences after surgery
The consequences of the operation, as well as the natural course of the disease, very often is cerebral vasospasm, which leads to unsatisfactory treatment results - death or severe neurological deficit in the form of paresis and paralysis, aphasia, mental disorders (which is typical for aneurysms of the anterior communicating artery). Meningitis may be a complication of the operation itself, which is associated with the presence of blood - a rich nutrient medium in the subarachnoid space, in the basal cisterns, cerebral ischemia, and a rather long operation time.
Thus, the treatment of arterial aneurysms is a very urgent and difficult problem in neurosurgery, especially in the acute and acute periods of hemorrhage.
Author of the article: neurosurgeon Anton Viktorovich Vorobiev Frame around the text
Why choose us:
- we will offer the most optimal treatment method;
- we have extensive experience in treating major neurosurgical diseases;
- We have polite and attentive staff;
- Get qualified advice on your problem.
Complications
One of the most dangerous complications of an aneurysm, which often becomes fatal, is its rupture with subsequent hemorrhage.
· If the lesion is localized in the brain, the clinical picture will resemble a hemorrhagic stroke.
· Particularly massive hemorrhage, which can lead to rapid death, is observed when an aortic aneurysm ruptures.
· When the lesion is localized in the myocardium, cardiac arrest occurs.
Aneurysm rupture may be preceded by dissection of the arterial wall. Most often, dissection occurs in the aorta. In this case, a second (false) passage is formed, through which blood flow can continue. With large aneurysms, the development of thromboembolism is also possible.
Cerebral aneurysm - symptoms
Most often, an aneurysm debuts with rupture - the most serious, often fatal complication. Hemorrhage can be subarachnoid, parenchymal and ventricular , and there are also all kinds of combinations of this trinity.
Among the atypical manifestations is pseudotumor ; with a gigantic size of the aneurysm, it can behave like a tumor and compress the brain and nerves, causing focal neurological symptoms.
A migraine-like course is manifested by hemicranialgia.
Pseudoradicular simulates radiculitis - pain in the legs, which is caused by blood flowing into the terminal cistern of the spinal cord.
Meningitis-like - in this case, patients with suspected bacterial meningitis can be admitted to an infectious diseases hospital, where SAH and suspected aneurysm rupture are diagnosed only with a lumbar puncture.
Psychotic - the name speaks for itself.
What is a fusiform aneurysm?
- A spindle-shaped cerebral aneurysm is one of the types of aneurysms in which a uniform stretching of the walls of the blood vessel occurs.
- Diffuse dilatation of the vessel that does not occur in the region of the bifurcation or the mouth of the vessel
- Causes: Atherosclerosis, connective tissue diseases, traumatic dissection.
There are four forms:
- Type 1. Acute dissecting aneurysms.
- Type 2. Segmental ectasia.
- Type 3. Chronic dissecting aneurysms.
- Type 4. Aneurysms of atypical localization (not in the area of vessel bifurcation).
Histopathology: Fragmentation of the internal elastic membrane
- Angiogenesis in thickened intima
- Intramural hematoma and blood clots with blood vessels
- Repeated intramural hemorrhages.