Considering that today, according to statistics, diseases of the cardiovascular system are the leading causes of death in civilized countries, it is not surprising that not only their main varieties, but also any terminology related to this topic, and all pathological processes, are of increased interest. occurring in the heart muscle. Hypertrophy of the left ventricular myocardium also relates to such questions, in particular: where does its development begin and is it possible to stop the pathological process?
General information about pathology
In fact, myocardial hypertrophy of the left ventricle of the heart is a pathology characterized by an increase in the mass of the heart muscle as a result of constantly elevated pressure in the patient (we can say that this is an “additional ailment of hypertensive patients”).
Interestingly, initially, this is not a disease, but simply a protective reaction of the body to too frequent increases in blood pressure. Then, hypertrophy leads to a thickening of the mass of the walls of the ventricles, as well as to modification of the septum. In this regard, the elasticity of the wall decreases, and the thickening can concern both certain areas and occur evenly.
For a more visual representation, this process can be considered using the example of the hands: the muscles, reacting to an ever-increasing load, gradually thicken and increase in size. The same thing happens with the heart muscle, but only if for the biceps this process is desirable and useful, then for the myocardium it is the opposite. The problem is that the vessels are not able to grow as quickly, and therefore they will not be able to provide the cells with sufficient oxygen and nutrients, which will subsequently lead to oxygen starvation.
I want to know the cost of treatment
Right ventricular hypertrophy
Atrial enlargement (dilatation or hypertrophy) can cause severe P wave deformation, but changes in the QRS complex are associated primarily with ventricular hypertrophy . On the electrocardiogram, typical signs of ventricular hypertrophy appear, and not just their enlargement.
Electrocardiogram changes caused by right and left ventricular hypertrophy can be predicted by knowing the normal shape of the QRS complexes. Normally, depolarization of the LV and RV occurs simultaneously . The electrical potentials of the left ventricle predominate, since its mass is greater (see section “Normal cardiogram”). rS-type complexes appear in the right chest leads (for example, in lead V1) .
In rS complexes, a deep negative P wave reflects the spread of depolarization from right to left. qR-type complexes appear in the left precordial leads (for example, in leads V5 and V6) .
In the qR complex, a high, positive R wave reflects the predominant direction of LV depolarization to the left.
With severe RV hypertrophy, its potentials prevail over the LV potentials. At the same time, high R waves appear in the right chest leads, which indicates the spread of positive potentials from the hypertrophied RV to the right.
Rice. 6-7. The shape of the QRS complex in LV and RV hypertrophy can be assumed by knowing the basic principles of electrophysiology. LV hypertrophy leads to the appearance of deep S waves in the right precordial leads and tall R waves in the left. With RV hypertrophy, on the contrary, the QRS vector is shifted to the right, so tall R waves appear in the right precordial leads.
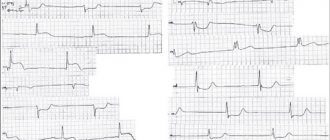
In Fig. 6-8 and 6-9 are other examples of electrocardiograms for right ventricular hypertrophy. Instead of the normal rS complex, a high positive R wave appears in lead V1 - a sign of right ventricular hypertrophy .
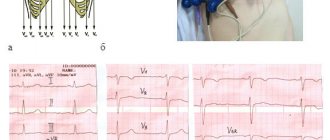
Rice. 6-8. High R wave and negative T wave with RV overload in lead V1 in a patient with tetralogy of Fallot. A sharp deviation of the EOS to the right (the R wave in lead III is higher than in lead II).
Rice. 6-9. With RV hypertrophy, a tall R wave (part of the qR complex) can sometimes appear in lead V1; due to an increase in PP in leads II, III, V1 - high P waves; negative T waves in lead V1 (arrow) and ST segment depression in leads V2, V3 are associated with RV overload; The PR interval is also lengthened (0.24 s).
How high should the R wave be in lead V1 for RV hypertrophy?
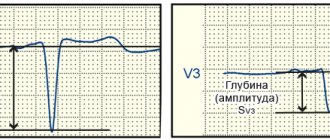
In adults, the R wave in lead V1 is normally smaller than the S wave. If the amplitude of the R wave exceeds the amplitude of the S wave in lead V1, this is an indirect, but not diagnostic sign of RV hypertrophy. Sometimes in this lead a small q wave precedes a tall R wave (see Fig. 6-8).
Along with high R waves in the right precordial leads, two other signs are often detected with RV hypertrophy - deviation of the EOS to the right and inversion of T waves in leads V1-V4.
RV hypertrophy affects the process of depolarization (QRS complex) and repolarization (ST-T complex). With myocardial hypertrophy, the normal sequence of repolarization is disrupted, the reasons for which have not been sufficiently studied. A characteristic sign of pancreatic hypertrophy is the appearance of negative T waves in leads V1-V4 (see Fig. 6-8, 6-9). These T wave changes have previously been associated with RV load. The preferred term is “T wave inversion associated with RV overload.”
The reasons for the development of pancreatic hypertrophy (congenital heart pathology, lung diseases) also often cause overload of the pancreas. Thus, often signs of RV hypertrophy can be combined with high P waves. Most often, RV hypertrophy with LA overload occurs with mitral stenosis.
Blockade of PNPG is not considered a sign of pancreatic hypertrophy. However, the presence of complete or incomplete blockade of PNPG with deviation of the EOS to the right is possible with enlargement of the RV.
So, with RV hypertrophy, high R waves appear on the electrocardiogram in the right precordial leads. In lead V1, the R wave may be higher than the S wave. With RV hypertrophy in the left precordial leads, different variants of the QRS complex are possible. Sometimes in leads V3-V6 there is no growth of the r wave, the rS or RS complexes are visible before lead V6 (see Fig. 6-9). In other cases, the normal growth of the R wave is preserved, in the left chest leads there are R waves (see Fig. 6-8). In addition, EOS deviation to the right and T wave inversion in the right precordial leads often occur. Sometimes with pancreatic hypertrophy, only one of these signs is present.
The appearance of all three signs (deviation of the EOS to the right, high R waves and T wave inversion in the right precordial leads) indicates severe RV1 hypertrophy.
Note. 1 Modern guidelines for electrocardiography usually distinguish 3 types of ECG changes during RV hypertrophy: 1) rSK-mun ECG (rSK complex is recorded in lead V1), indicating a moderate increase in RV mass; 2) R-mun ECG (qR or Rs with a high R wave is recorded in lead V1) – pronounced RV hypertrophy; 3) S-mun ECG (S wave is recorded in all chest leads V1-V6), which is more often detected in patients with severe pulmonary emphysema, when the heart is sharply displaced posteriorly. Note, ed.
Pancreatic hypertrophy is possible in various clinical conditions. An important reason is congenital malformations of the heart: pulmonary artery stenosis, atrial septal defect [in patients with enlarged right ventricle, the most common atrial septal defects often show signs of PNPG block (RSR complex in lead V1), EOS is vertical or deviated to the right], tetralogy of Fallot , Eisenmenger syndrome. In patients with chronic lung diseases, pulmonary hypertension syndrome and pancreatic hypertrophy may occur. As mentioned earlier, with mitral stenosis, LA overload and RV hypertrophy can be combined. Possible inversion of the G wave in leads V1-V3 due to overload of the RV. There are no other signs of pancreatic hypertrophy, as in acute pulmonary embolism (Chapter 11), on the electrocardiogram.
In patients with pulmonary emphysema and RV overload, the described changes in the electrocardiogram may be absent. Instead of high R waves in the right precordial leads, only a slight increase in their amplitude is noted. A deviation of the EOS to the right is also usually observed.
Types of hypertrophy
Depending on the ratio of the ventricular mass index and the relative thickness of its walls, hypertrophic changes are divided into the following types (A. Ganau classification):
- eccentric hypertrophy of the left ventricular myocardium (it is characterized by normal wall thickness and an increased ventricular mass index);
- concentric hypertrophy of the left ventricular myocardium (both indicators are increased);
- concentric remodeling of the left ventricle (wall thickness is increased, while the ventricular mass index remains normal);
- normal ventricle size.
The next division occurs according to forms, according to which there can be symmetrical hypertrophy of the myocardium of the left ventricle (also concentric) and asymmetrical (in the left ventricle the lower, middle or upper part, the septum is hypertrophied).
How to arrive for treatment
What consequences can the pathology have?
Hypertrophied heart muscle faces many complications, among them the following should be noted:
- arrhythmia (heart rhythm disturbances);
- ischemic disease (impaired blood supply to the myocardium);
- angina pectoris (insufficient supply of oxygen and nutrients to the heart, i.e. oxygen starvation);
- heart failure (a condition in which the heart muscle does not have time to pass the required volume of blood);
- heart attack (stopping blood supply);
- cardiac arrest.
Attention! Despite the huge number of dangerous consequences, people live with the disease for decades. When making this diagnosis, there is no need to panic, you just need to follow preventive measures and then your heart will not fail.
Reasons for violations
Cardiac dysfunction in the human body occurs for the following reasons:
- Regular consumption of drinks containing strong alcohol;
- Constant smoking;
- Heart disease;
- Heart failure;
- Excess thyroid hormones;
- Mitral valve protrusion;
- Uncontrolled use of glycosides or drugs against arrhythmia.
An increase in heart rate eliminates disturbances in a person’s respiratory activity.
An electrocardiogram (ECG) is not a new and time-tested method of identifying heart pathologies. This procedure requires very little time and does not require any preparatory steps. However, in order to get the correct result, transcript and doctor’s conclusion, sometimes you need to undergo such an examination several times. Based on the data obtained and clinical examinations, the cardiologist will diagnose the patient and prescribe treatment.
Causes leading to illness
The following diseases and conditions are considered to be the causes of myocardial hypertrophy:
- arterial hypertension;
- heart disease;
- idiopathic hypertrophy;
- excessive physical activity;
- sleep apnea (or otherwise - snoring). This is caused by involuntary cessation of breathing for a few seconds during sleep and a delay in oxygen supply.
Sign up for a consultation
The development of left ventricular myocardial hypertrophy usually occurs against the background of hypertension, but can be a consequence of excessive physical stress on the body. Therefore, heavy professions (masons, loaders) are called the reasons for the development of hypertrophy.
Attention! Active smokers and those people who lead a sedentary lifestyle are at particular risk.
Treatment
Therapy is carried out with beta blockers in combination with verapamil. This method can reduce symptoms caused by cardiovascular pathology. Diet is recommended as an adjunct to drug therapy. You also need to give up habits that harm the body, if any.
For treatment to be effective it is necessary to: give up cigarettes, reduce the level of dietary salt intake, and lose excess body weight.
The diet should be enriched with dairy and fermented milk products, seafood, fresh vegetables and fruits. You will need to reduce the amount of consumption of flour products, limit sweets and animal fats. Physical activity should be moderate.
Doctors do not rule out the possibility that surgery will be needed to remove a section of the heart muscle that has undergone hypertrophy. It is important to note that the development of this disease often occurs over several years of life.
How does treatment occur and how to increase its effectiveness?
Mandatory treatment of left ventricular myocardial hypertrophy includes the elimination of hypertension with the help of antihypertensive drugs. Also, the course of therapy includes: beta-blockers, angiotensin-converting enzyme inhibitors, thiazide diuretics. Calcium antagonists are also effective (by the way, they are designed for a long course of therapy).
Get more information
In dangerous stages of hypertrophy development (muscles grow, the thickness of the left ventricular wall increases, thereby squeezing the coronary artery of the myocardium), which leads to ischemic changes and infarction, the patient can be treated with surgery.
You can help yourself stop the development of pathology if you completely change your usual lifestyle and pay attention to periodic examinations (ultrasound and electrocardiogram should be done 1-2 times a year). Hiking in the fresh air, sports (running or other), giving up bad habits, reducing salt intake, and preventing stress should become mandatory.
Diagnostics
Only a cardiologist, who is guided by anamnesis and examination, can examine the patient.
One of the effective methods is electrocardiography, which allows you to measure the thickness of the heart muscle. With hypertrophy, the following changes are visible on the ECG:
- the vector of the average QRS relative to its position deviates strongly to the right side and forward;
- teeth Rv I, III and SI, V6 increase;
- the time of internal deviations increases;
- conductivity in the myocardium itself is disrupted;
- the electrical axis deviates towards the hypertrophied ventricle;
- the electrical position is modified;
- a shift occurs in the transition zone to another chest lead;
- incomplete or complete blockade of the His bundle.
In addition to the above diagnostic methods, the doctor conducts an examination using magnetic nuclear resonance, computed tomography and chest x-ray.