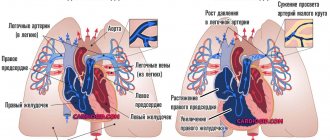
Anticoagulants are drugs that slow down blood clotting. Doctors prescribe such drugs to patients who have an increased risk of developing blood clots (thrombi). In a healthy person, the formation of a blood clot is necessary as a protective mechanism in case of injury or bleeding. In a patient, the formation of blood clots in large vessels can be life-threatening, worsen the course of the disease, and can cause serious complications (especially when blood clots form in the vessels that supply vital organs - the heart, lungs, brain, kidneys, etc.).
| Need specialist advice? to the doctor. Online. For free. ASK A CARDIOLOGIST A QUESTION |
Anti-clotting drugs have different mechanisms of action. "Direct" anticoagulants
(for example, heparin) the patient receives by injection, usually in a hospital. They are analogues of molecules in the human body, their action begins immediately after administration. For long-term prevention, tablet drugs are used, most often “indirect” anticoagulants such as warfarin. They are called “indirect” because the slowdown in blood clotting is caused not by the drug itself, but by its indirect effect in the body.
Why is this necessary?
If you have suffered deep vein thrombosis of the lower or upper extremities, your doctor will most likely prescribe you indirect anticoagulants.
The main drug in this group today, both here and abroad, is warfarin. In our country, another drug of this group is used quite widely - phenylin. Other coumarin drugs (acenocoumarol, marcumar, marivan) can be used. The recommendations given are mostly applicable to any anticoagulant. The purpose of this medication is to prevent blood clots from recurring, which could cause your condition to worsen or cause life-threatening complications. The risk of recurrence of thrombosis is quite high during the first year after the first episode of the disease, therefore, taking into account various factors, warfarin is prescribed for a period of 2 to 12 months. In rare cases, longer therapy is performed. Indirect anticoagulants have no effect on an already formed blood clot.
To determine the duration of treatment, special (including genetic) blood tests are sometimes required to identify an increased tendency to blood clots.
A very large number of patients around the world receive the treatment you have prescribed. It is used not only in phlebology, but also in such areas of medicine as vascular surgery. In addition to deep vein thrombosis, the basis for prescribing anticoagulant therapy is often previous heart attacks, cardiac arrhythmias, valve and peripheral vessel replacement, and much more.
Who do doctors prescribe “indirect” anticoagulants (warfarin)?
Patients who need treatment and prevention of thrombosis and embolism of blood vessels, including: – heart rhythm disturbances (atrial fibrillation); – heart valve diseases;
– presence of prosthetic heart valves or blood vessels, incl. in combination with aspirin (acetylsalicylic acid); – acute venous thrombosis (phlebothrombosis) and pulmonary embolism (in combination with heparin); – recurrent venous thrombosis; – repeated pulmonary embolism; – thrombosis of peripheral, coronary and cerebral arteries; – postoperative thrombosis; – myocardial infarction, complicated by the development of an aneurysm and intracardiac thrombus; – during surgical or thrombolytic treatment of thrombosis; – when performing electrical cardioversion of atrial fibrillation (as an additional therapy); – congenital diseases accompanied by pathological thrombosis (thrombophilia).
How to monitor treatment
Carrying out antithrombotic (anticoagulant) therapy can save your life and health, but requires increased attention and mandatory compliance with the doctor’s recommendations. Warfarin is a drug that reduces the ability of blood to clot, so its excess can lead to hemorrhagic complications, i.e. to bleeding. To avoid complications, the required dose of warfarin is monitored using a blood test called INR (International Normalized Ratio). This may sometimes be referred to as INR in laboratory responses. During the entire period of taking warfarin, the INR should be in the range of 2.0 - 3.0. If the INR is less than 2.0, then blood clotting is not reduced and thrombotic complications are possible. If the INR is more than 4.0, hemorrhagic complications are very real. An increase in INR from 2.5 to 4.0 indicates the need to reduce the dose of the drug, but usually does not pose a direct threat. For some diseases, the required upper limit of INR is 4.0 - 4.4.
In the absence of the ability to determine INR, monitoring by prothrombin time (PT) is acceptable, but this method is much less reliable. No other blood tests are needed to calculate your warfarin dose. To identify the side effects of the drug, a general blood test, urine test and some biochemical tests are periodically prescribed.
Warfarin
Information for downloading: — Life with warfarin, word >>> — Diary: Life with warfarin, pdf >>> — School for patients, WinRAR >>>
You have been prescribed WARFARIN
Why is this necessary?
The purpose of prescribing this medicine is to prevent the recurrence of blood clots, which could cause a sharp deterioration in your condition or the development of life-threatening complications. To determine the duration of treatment, special (including genetic) blood tests are sometimes required to identify an increased tendency to blood clots. The treatment prescribed to you is received by a very large number of patients all over the world. It is used not only in phlebology, but also in such areas of medicine as vascular surgery. In addition to deep vein thrombosis, the basis for prescribing anticoagulant therapy is often previous heart attacks, cardiac arrhythmias, valve and peripheral vessel replacement, and much more.
Warfarin dose selection
The most difficult and responsible stage. Dose selection can be carried out both with and without the use of low molecular weight heparins (Fraxiparine, Clexane), both in the hospital and on an outpatient basis. The selection period on average takes from 1 to 2 weeks, but in some cases it increases to 2 months. At this time, you will need frequent INR determinations, up to 2 - 3 times a week or daily. Each time, after receiving the next test result, your doctor will determine a change in the dose of the medication and the date of the next test. If in several tests in a row the INR remains in the range of 2.0 - 2.5, this means that the dose of warfarin has been adjusted. Further monitoring of treatment will be much easier.
How to take the drug
Warfarin is taken in the entire daily dose at one time, preferably at 17:00 - 19:00. Take the tablets with water. It is not recommended to take it with food, but can be taken on an empty stomach. Most often, the “starting” and “maintenance” doses of the drug are 2 tablets per day. In many cases, for more “fine” adjustments, you will change the dose of the medicine that you take not per day, but per week. This may require either dividing the tablet in half or taking different numbers of tablets on different days. To make it easier to monitor your treatment, you may be given a special account book, or you can keep a notebook with a treatment diary, where it is useful to note the doses of warfarin, INR level, and other laboratory data.
How to monitor treatment
Carrying out antithrombotic (anticoagulant) therapy can save your life and health, but requires increased attention and mandatory compliance with the doctor’s recommendations. Warfarin is a drug that reduces the ability of blood to clot, so its excess can lead to hemorrhagic complications, i.e. bleeding. To avoid complications, the required dose of warfarin is monitored using a blood test called INR (International Normalized Ratio). This may sometimes be referred to as INR in laboratory responses. During the entire period of taking warfarin, the INR should be in the range of 2.0 - 3.0. If the INR is less than 2.0, then blood clotting is not reduced and thrombotic complications are possible. If the INR is more than 4.0, hemorrhagic complications are very real.
WHAT CAN AFFECT TREATMENT
- Any concomitant diseases (including “colds” or exacerbation of chronic diseases)
- The use of drugs that affect the blood coagulation system. This is especially true for a large class of drugs that includes aspirin. It also includes many drugs prescribed as anti-inflammatory and painkillers (diclofenac, ibuprofen, ketoprofen, etc.). As a mild analgesic during treatment with warfarin, it is better to use paracetamol in normal dosages. In any case, the need for a new medication and the duration of its use must be agreed with the attending physician. When warfarin and aspirin are prescribed simultaneously, the INR is maintained in the range of 2.0 - 2.5.
- The use of drugs that affect the absorption, excretion and metabolism of warfarin. Most often, it is necessary to take into account the prescription of broad-spectrum antibiotics and oral antidiabetic agents. However, taking any new medicine may change how warfarin works. If concomitant treatment is necessary, additional INR analysis is usually prescribed at the beginning and end of therapy.
- Diet changes.
Warfarin acts on blood clotting through vitamin K, which is found in varying amounts in food.
There is no need to avoid foods high in vitamin K! Nutrition should be complete. You just need to make sure that there is no significant change in their proportion in the diet, for example, depending on the season. If you significantly increase your intake of foods rich in vitamin K while on a stable dose of warfarin, this may greatly weaken its effect and lead to thromboembolic complications.
The maximum amount of vitamin K (3000 - 6000 mcg/kg) is found in dark green leafy vegetables and herbs (spinach, parsley, green cabbage), and in green tea up to 7000 mcg/kg; intermediate amounts (1000 - 2000 mcg/kg) - in plants with paler leaves (white cabbage, lettuce, broccoli, Brussels sprouts). A significant amount of the vitamin is found in legumes, mayonnaise (due to vegetable oils), and green tea. Fats and oils contain varying amounts of vitamin K (300 - 1000 mcg/kg), more of it in soybean, rapeseed, and olive oils. The content of vitamin K in dairy, meat, bakery products, mushrooms, vegetables and fruits, black tea, coffee is low (no more than 100 mcg/kg).
Taking multivitamins that contain vitamin K may reduce the effect of warfarin.
What you should immediately tell your doctor about
- Black (tarry) stool color
- Pink or red urine
- Bleeding from the nose or gums (including when brushing teeth)
- Unusually heavy or prolonged menstrual bleeding
- Bruises or swelling on the body that occur for no apparent reason
- Any significant changes in well-being or health
- The appearance of skin spots on the thighs, abdominal wall, mammary glands
What to avoid
- Engaging in traumatic sports where blows, bruises, and falls are possible.
- Intramuscular injections. In outpatient treatment, in most cases, medications can be selected for oral administration.
- Repeatedly take the medicine within one day. If you do not remember whether you took warfarin today, skip the dose.
Products containing vitamin K. They should be LIMITED in the diet:
| Products | Mkg/100g product |
| Green tea, leaves | 964 |
| Lettuce, green leaves | 850 |
| Chard, leaves raw | 830 |
| Brussels sprouts, top leaves | 817 |
| Spinach, leaves raw | 487 |
| Spinach, leaves, fresh/frozen, cooked | 438 |
| Black tea | 383 |
| Raw cabbage, boiled | 360 |
| Chicory, raw | 342 |
| Red leaf salad | 289 |
| Broccoli raw | 289 |
| Soybean oil | 231 |
| Broccoli, fresh/frozen, cooked | 210 |
| Green onions | 205 |
| Beans | 193 |
| Iceberg lettuce | 123 |
Hemostasis
Problems with the hemostatic system - what is it for the average person? Interview with hemostasiologist Anatoly Brazhnikov and head of the laboratory “Hemostasis and Genetics” Marina Bubenshchikova
How to take the drug
Warfarin is available in 2.5 milligram tablets. Most often, the “starting” and “maintenance” doses of the drug are 5 milligrams (2 tablets) per day. In many cases, for more “fine” adjustments, you will change the dose of the medicine that you take not per day, but per week. This may require either dividing the tablet in half or taking different numbers of tablets on different days. To make it easier to monitor your treatment, you may be given a special account book, or you can keep a notebook with a treatment diary, where it is useful to note the doses of warfarin, INR level, and other laboratory data.
Warfarin is taken in the entire daily dose at one time, preferably at 17:00 - 19:00. Take the tablets with water. It is not recommended to take it with food, but can be taken on an empty stomach. Phenyline is usually taken in 2 doses.
Warfarin dose selection
The most difficult and responsible stage. “Loading” initial doses of warfarin (more than 5 mg) are not recommended.
Dose selection can be carried out both with and without the use of low molecular weight heparins (Fraxiparine, Clexane), both in the hospital and on an outpatient basis. The selection period on average takes from 1 to 2 weeks, but in some cases it increases to 2 months. At this time, you will need frequent INR determinations, up to 2 - 3 times a week or daily. Each time, after receiving the next test result, your doctor will determine a change in the dose of the medication and the date of the next test.
If in several tests in a row the INR remains in the range of 2.0 - 2.5, this means that the dose of warfarin has been adjusted. Further monitoring of treatment will be much easier.
Use (effect) of warfarin, dose, overdose
The body needs vitamin K to ensure blood clotting.
A person gets vitamin K from food, mainly from vegetables. Vitamin K can also be produced in the human intestine by special intestinal bacteria. From the intestines, vitamin K is absorbed into the blood and goes to the liver, the “laboratory” of the body. In the liver, with the participation of vitamin K, blood clotting factors necessary for the formation of a blood clot (thrombus) are synthesized. These are prothrombin (factor II), factors VII, IX and X. They are called “vitamin K-dependent factors”.
The action of warfarin is to reduce the formation of vitamin K-dependent factors. As long as warfarin is regularly injected into your body, your blood's clotting time is prolonged and this prevents blood clots from forming. There is also a risk of bleeding if the dose of the drug is excessive.
The effect of warfarin on blood clotting varies from person to person.
Therefore, each patient receives his own, individually selected dose. To achieve the desired effect, a minimum of 4-5 days is required, often dose selection lasts up to 2-3 weeks. Prescription of the drug and further monitoring are carried out using the determination of INR. The daily dose of warfarin is taken orally once a day, in the evening (at 18.00-19.00 hours); if necessary, the tablet or part of it can be chewed and washed down with water.
What should you tell your doctor about if you start taking warfarin or are already being treated with it?
About all problems associated with bleeding or its risk (stomach or duodenal ulcers, colon; hemorrhoidal bleeding; heavy menstruation), liver and kidney diseases, high blood pressure and diabetes. Very important if you are planning a pregnancy or are already pregnant. Warfarin has a teratogenic effect. This means that taking it can lead to various deformities in the fetus (if taken in the first trimester of pregnancy) or to intrauterine bleeding (in later stages). Therefore, women whose pregnancy occurred while taking warfarin are recommended to terminate it.
Monitoring the dose of warfarin
If the dose of the drug is selected, less frequent monitoring is sufficient - first once every 2 weeks, then once a month. The frequency of additional studies is determined separately. The need for an extraordinary determination of the INR may arise in a number of cases, which we will discuss below. If in any doubt, ask your doctor for advice.
Currently, there are portable devices for self-determination of INR (similar to systems for monitoring blood sugar levels in patients with diabetes), but their cost is very high and, in most cases of deep vein thrombosis, purchasing them is impractical.
What may affect treatment
- Any concomitant diseases (including “colds” or exacerbation of chronic diseases)
- The use of drugs that affect the blood coagulation system. This is especially true for a large class of drugs that includes aspirin. It also includes many drugs prescribed as anti-inflammatory and painkillers (diclofenac, ibuprofen, ketoprofen, etc.). As a mild analgesic during treatment with warfarin, it is better to use paracetamol in normal dosages. In any case, the need for a new medication and the duration of its use must be agreed with the attending physician. When warfarin and aspirin are prescribed simultaneously, the INR is maintained in the range of 2.0 - 2.5.
- The use of drugs that affect the absorption, excretion and metabolism of warfarin. Most often, it is necessary to take into account the prescription of broad-spectrum antibiotics and oral antidiabetic agents. However, taking any new medicine may change how warfarin works. If concomitant treatment is necessary, additional INR analysis is usually prescribed at the beginning and end of therapy.
- Diet changes.
Warfarin acts on blood clotting through vitamin K, which is found in varying amounts in food.
There is no need to avoid foods high in vitamin K! Nutrition should be complete. You just need to make sure that there is no significant change in their proportion in the diet, for example, depending on the season. If you significantly increase your intake of foods rich in vitamin K while on a stable dose of warfarin, this may greatly weaken its effect and lead to thromboembolic complications.
The maximum amount of vitamin K (3000 - 6000 mcg/kg) is found in dark green leafy vegetables and herbs (spinach, parsley, green cabbage), and in green tea up to 7000 mcg/kg; intermediate amounts (1000 - 2000 mcg/kg) - in plants with paler leaves (white cabbage, lettuce, broccoli, Brussels sprouts). A significant amount of the vitamin is found in legumes, mayonnaise (due to vegetable oils), and green tea. Fats and oils contain varying amounts of vitamin K (300 - 1000 mcg/kg), more of it in soybean, rapeseed, and olive oils. The content of vitamin K in dairy, meat, bakery products, mushrooms, vegetables and fruits, black tea, coffee is low (no more than 100 mcg/kg). Regular consumption of berries and cranberry juice may increase the effect of warfarin.
Small doses of alcohol with normal liver function do not affect anticoagulant therapy, but alcohol consumption must be treated with caution.
Taking multivitamins that contain vitamin K may reduce the effect of warfarin.
Diet while taking warfarin. Vitamin K content
Warfarin is absorbed in the stomach and jejunum, so changes in the intestinal microflora that produce vitamin K may affect the effect of the drug. The activity of warfarin can also be affected by the food the patient eats. The diet when taking warfarin should take into account those foods that contain large amounts of vitamin K, which can weaken the effect of warfarin, and the lack of vitamin K in the diet can enhance the effect of the drug. Therefore, if you are prescribed warfarin, try to eat a balanced diet and try not to change your diet dramatically so as not to change the amount of vitamin K you get from food.
| Vitamin K content in foods (µg/100 g) | |
| Beef liver | 93 |
| Cheese | 35 |
| Butter | 30 |
| Egg | 11 |
| Soybean oil | 193 |
| Broccoli | 175 |
| Cabbage | 125 |
| Salad | 129 |
| Watercress | 200 |
| Head lettuce | 120 |
| Spinach | 415 |
| Cauliflower | 80 |
| Green tomatoes | 80 |
| Beans | 45 |
| Cucumbers, zucchini | 30 |
| Potato | 16 |
| Green tea | 712 |
| Note: daily requirement of vitamin K is 0.03-1.5 mcg/kg/day (up to 105 mcg/day) | |
Warfarin and alcohol
Alcohol is not recommended during warfarin treatment.
You can indulge in a glass of wine once or twice a week. Exceeding this norm may lead to increased effects of the drug and, as a result, possible bleeding. Illnesses that affect appetite and digestion (vomiting, diarrhea) can also reduce or increase the effect of warfarin, so tell your doctor about any changes in how you feel.
Be sure to tell us about all the medications you are taking or have taken shortly before starting warfarin treatment, as well as new prescriptions if you are already taking warfarin therapy. Many drugs can increase or decrease the effect of warfarin on blood clotting. Keep all prescriptions and write down the names of medications you take. The table shows the most commonly prescribed drugs that can affect the effectiveness of warfarin.
How to take medications correctly
It is important
Always tell any health care professional you see that you are taking anticoagulants. It is advisable to carry your “account” book or treatment diary with you.
Most dental procedures (except tooth extraction) can be performed without changing your treatment regimen. When removing a tooth, it is usually sufficient to use a tampon with a local hemostatic agent (aminocaproic acid, thrombin sponge).
If you have problems with blood pressure, you need to regularly monitor it and maintain it at a level not higher than 130/80 mmHg.
Warfarin and pregnancy
During pregnancy, taking warfarin is contraindicated. In the event of pregnancy, indirect anticoagulants are immediately discontinued; if further prevention of thrombosis is necessary, heparins are usually used. Therefore, if you suspect pregnancy, refrain from taking the drug until you consult your doctor.
It is possible to use warfarin during breastfeeding. Warfarin is excreted in breast milk in extremely small quantities and does not affect the baby's blood clotting processes, but for complete safety it is recommended to refrain from breastfeeding during the first three days of the mother's treatment with the drug.