Arrhythmology Center
Rhythm disturbances are a pathological increase or decrease in heart rate, often a consequence of combined diseases (coronary heart disease, hypertension, endocrine disorders, disorders of the autonomic nervous system, etc.).
Many types of arrhythmia do not pose a threat, but some types of arrhythmia can be dangerous and threaten human life.
Symptoms of rhythm disturbance
— change in heart rate (the average heart rate at rest is from 40 to 120 beats/min)
- a feeling of interruptions in the work of the heart
- irregular heartbeat
- pre-fainting or fainting states
- weakness and dizziness
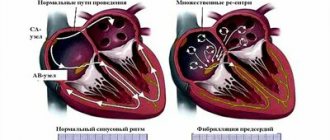
The most common arrhythmia, atrial fibrillation (atrial fibrillation), develops as a result of age-related changes in the heart and/or concomitant pathology of the cardiovascular system; occasionally it can be an independent disease, mainly in young patients.
Examinations are carried out using modern diagnostic equipment and performed by highly qualified experienced specialists. Based on their results, the patient receives an individual treatment and prevention program, which will undoubtedly help both prolong life and improve its quality.
If you are concerned about irregular heartbeat, do not ignore the unpleasant symptoms.
Our team has the most experience in the country in cryoballoon techniques for treating atrial fibrillation (atrial fibrillation), is in a leading position in the prevention of cardiogenic strokes by implanting a left atrial appendage occluder, as well as in high-density cardiac mapping, which makes the treatment of cardiac arrhythmias more personalized, increasing efficiency and reducing trauma to the body and heart in particular.
It may be dangerous!
The Center's arrhythmology team successfully treats patients with a wide range of diseases, including:
- Paroxysmal and persistent atrial fibrillation
- Sick sinus syndrome, AV block and other bradyarrhythmias
- Supraventricular tachycardia
- Ventricular extrasystole
- Ventricular tachycardia
- Management of patients with implanted pacemakers/defibrillators
- Chronic heart failure (CHF)
- Cardiomyopathies of various origins
- Genetic channelopathies
- Congenital disorders of cardiac rhythm and conduction
- Syncope
- Life-threatening cardiac rhythm and conduction disorders
Types of interventions
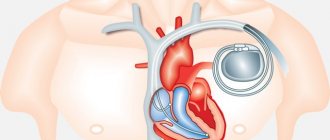
- Surgical treatment of cardiac conduction disorders using the installation of permanent pacemakers (artificial pacemakers)
- Minimally invasive treatment of chronic heart failure (CHF) using implantation of cardiac resynchronization therapy devices
- Treatment of refractory heart failure by installing a heart modulation system - “Optimizer”
- Implantation of a left atrial appendage occluding device for the prevention of cardiogenic strokes in atrial fibrillation
- Installation of cardioverter-defibrillators for the prevention of sudden cardiac death
- Implantation of long-term ECG monitoring systems (active ECG monitoring – from 1.5 to 3 years)
- Radiofrequency and cryoablation of arrhythmogenic areas of the heart - postoperative monitoring of patients, testing and reprogramming of implanted devices
Our advantages
- Many years of experience
- Modern minimally invasive surgical treatment methods, including unique ones
- Minimum percentage of complications compared to world statistics
- Maximum efficiency – along with the world’s leading clinics
- Continuous cooperation and joint operations with colleagues from Europe and Israel
- Use and co-authorship in national and international guidelines
About the department
In the department of surgical treatment of complex cardiac arrhythmias and cardiac pacing (OHP) of the City Clinical Hospital named after. I.V. Davydovsky carries out all types of interventional procedures for the treatment of cardiac arrhythmias (ventricular and supraventricular arrhythmias, atrial tachycardia, atrial flutter and fibrillation, atrial and ventricular extrasystole, etc.); implantation of a wide range of devices for the diagnosis and treatment of cardiac arrhythmias (pacemakers, cardioverter-defibrillators, subcutaneous loop heart rate monitors, etc.).
Types of arrhythmias and their clinical manifestations
What to do if you have cardiac arrhythmia? Symptoms and treatment of cardiac arrhythmia depend on the type of pathology.
Extrasystole . Extraordinary contraction of the heart muscle. It develops due to the appearance of additional foci of excitation. Extrasystole often accompanies various heart diseases, and is also observed in persons with an easily excitable nervous system. Patients who have extrasystole clearly feel interruptions in the functioning of the heart. This can be evidenced by the pulse, during the measurement of which the premature appearance of a pulse wave can be traced. Patients note a strong heartbeat, after which there is a feeling of cardiac arrest. The condition is sometimes accompanied by a feeling of anxiety, fear, lack of air, and symptoms of cardiac arrhythmia are: high blood pressure and heart attacks. Weakness, sweating, and chest discomfort appear.
Paroxysmal tachycardia . A sharp disturbance in the heartbeat, in which the heart rate reaches 200–240 beats per minute, with all impulses coming from an additional focus, and not the sinus node. At the beginning of the attack, the patient feels a sharp shock in the heart area, after which a strong heartbeat begins. Weakness, dizziness, and tinnitus appear. A prolonged attack can cause loss of consciousness.
Heart block . Impairment of impulse conduction. Pathology accompanies many diseases, but most often occurs with rheumatism, myocarditis, and cardiosclerosis. In such patients the pulse is rare and weak. In severe cases, loss of consciousness is possible.
Atrial fibrillation . Rhythm disturbances manifested by contractions of individual muscle fibers, rather than the entire myocardium. They occur chaotically, the time intervals between them and the strength of contractions are not the same. Pathology is observed in cardiosclerosis, thyrotoxicosis, myocarditis, mitral valve stenosis. It happens in the form of attacks, but it can also bother you constantly. The most common symptoms of atrial fibrillation are palpitations, heart pain and frequent interruptions in its functioning. Patients suffer from shortness of breath, which worsens with the slightest physical exertion. They feel weak and afraid. Increased sweating and polyuria (increased urine production) appear.
Why are arrhythmias dangerous?
Patients often wonder why cardiac arrhythmia is dangerous. Like any pathology, in the absence of adequate therapy it can provoke the development of complications. The most severe of them is ventricular fibrillation. With it, dizziness and loss of consciousness suddenly occur, and involuntary urination occurs. Blood pressure cannot be determined, the pulse cannot be felt, breathing stops. If resuscitation measures are not carried out in time, death may occur.
With paroxysmal tachycardia, shortness of breath occurs due to chronic circulatory failure, and pulmonary edema may develop.
If atrial fibrillation is left untreated, the patient may have an ischemic stroke and may also develop severe heart failure.
With blockades, syncope may develop, which is accompanied by loss of consciousness, decreased muscle tone, and disturbances in the functioning of the lungs and cardiovascular system.
We do
Radiofrequency ablation of cardiac arrhythmias
Radiofrequency ablation (RFA) is a minimally invasive, highly effective surgical intervention in the heart, performed under the control of X-ray equipment. The procedure is carried out to treat extrasystole, supraventricular and ventricular heart rhythm disturbances. The therapeutic effect is achieved through a targeted effect on arrhythmogenic zones of the heart, high-frequency current (radiofrequency energy) with a temperature of 40-55 degrees or cooling (cryo-procedure) to -80 degrees. Catheter ablation is a very effective method of treating tachyarrhythmias and, being a fairly safe procedure, can permanently eliminate the cause of heart rhythm disturbances. In the vast majority of cases, this allows you to avoid constant medication use and still lead an active lifestyle.
Indications for RFA
Supraventricular rhythm disturbances:
- atrioventricular nodal reentrant tachycardia (AVNRT),
- atrioventricular reentrant tachycardia (AVRT) associated with the functioning of the accessory pathway (AP)
- atrial tachycardia (AT)
- atrial fibrillation (AF)
- atrial flutter (AF)
- atrial extrasystole
Ventricular arrhythmias:
- ventricular extrasystole
- idiopathic ventricular tachycardia
- ventricular tachycardia due to structural heart diseases.
Preparation for surgery : − it is necessary to refrain from eating and drinking water for 6-8 hours before the procedure. If necessary, in agreement with your doctor, you can take a few small sips of water if you need to wash down the medicine (for arterial hypertension, diabetes, etc.); − 2-3 days before the operation you will need to stop taking antiarrhythmic drugs (in consultation with the doctor); − be sure to tell your doctor or nurse if you are allergic to medications.
Catheters are inserted under local and intravenous anesthesia, usually in the groin (femoral vein access), neck (jugular vein access) or subclavian vein. The procedure uses special long flexible electrodes that can both record the electrical activity of the heart and stimulate the heart during electrophysiological testing (EPS). They are performed in the heart under fluoroscopic control.
EPI is part of a procedure performed to accurately diagnose cardiac arrhythmias.
By stimulating the heart, the doctor induces an arrhythmia and studies it. EPI helps to identify the localization of pathological pathways or ectopic foci. This is called "mapping". The EF laboratory has all the necessary equipment and medications for studying and stopping arrhythmias.
After EPI and identification of the source of arrhythmia, targeted radiofrequency or cryoablation is performed. This leads to the formation of a scar (3-4 mm in diameter), which does not conduct the electrical impulse and eliminates the arrhythmia.
To monitor the effectiveness of the procedure, repeated EPI is performed. If the arrhythmogenic focus is successfully eliminated, the procedure is completed.
Treatment of arrhythmia using ablation is a fairly lengthy procedure, usually requiring from 30 minutes to several hours.
After the procedure is completed and the electrodes are removed, pressure bandages are applied in the puncture area to prevent bleeding. On the first day, bed rest should be observed, which allows to stabilize the patient’s condition.
Atrioventricular nodal reentrant tachycardia (AVNRT)
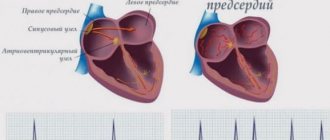
The normal propagation of the impulse from the sinus node to the ventricles passes through the region of the atrioventricular node. The heart valve rings separate the atrial myocardium from the ventricles and prevent direct passage of the impulse.
In patients with nodal tachycardia in the atrioventricular node, there are two pathways - slow and fast. And under certain conditions, a situation may arise when the impulse begins to quickly spin inside the node itself, and then almost simultaneously spread to the atria and ventricles.
The essence of the operation is to eliminate the “slow” path of impulse conduction in the AV node to prevent the tachycardia from spiraling. The effectiveness of the operation is 95-98%.
WPW syndrome (Wolff-Parkinson-White syndrome)
WPW syndrome is the second most common form of supraventricular tachycardia (after atrioventricular nodal tachycardia). In 1930, L. Wolff, J. Parkinson and P. White described the ECG syndrome of “functional bundle branch block” and short PQ interval, which is observed in young, physically healthy individuals suffering from attacks of tachycardia.
The anatomical substrate of WPW syndrome is the accessory atrioventricular (atrioventricular) junctions (ADJ), “bundles of Kent” or so-called “muscle bridges”. Additional atrioventricular connections are pathways between the myocardium of the atria and ventricles, existing in addition to the structures of the atrioventricular node.
The essence of the operation is to eliminate the “additional, abnormal” path of impulse conduction in the AV sulcus. The effectiveness of the operation is more than 98%.
Complications of the procedure. Like any surgical procedure, radiofrequency ablation is associated with certain risks. However, the risk is small (less than 1%) and the procedure is considered relatively safe: some patients experience bleeding at the site of insertion of the electrodes - this can cause the formation of a hematoma, in rare cases the procedure can lead to more serious complications associated with damage to the heart wall and blood vessels . Depending on the type and location of the pathological pathway, there is a risk of damage to the conduction system of the heart. Therefore, in some cases it may be necessary to implant a pacemaker. These complications are quite rare and the expected benefit from the procedure most often prevails over them. Doctors in our department do everything possible to reduce the risk of complications. Catheter ablation is a very effective method of treating tachyarrhythmias and, being a fairly safe procedure, can permanently eliminate the cause of heart rhythm disturbances. In most cases, this allows you to avoid constant medication use and still maintain an active lifestyle.
Ventricular heart rhythm disturbances
Ventricular heart rhythm disturbances can be in the form of extraordinary ventricular extrasystoles (VCs) or in the form of ventricular tachycardias (VT). RFA is performed in symptomatic patients and, most often, does not depend on the number of PVCs and when the patient with VT is hemodynamically stable. Preparation and surgery are almost the same as for supraventricular cardiac arrhythmias.
However, the effectiveness of the RFA procedure directly depends on the localization of the arrhythmogenic focus and on the patient’s concomitant structural diseases (coronary heart disease, valvular defects, cardiopathy, etc.)
Atrial fibrillation
More than 3 million people in Russia suffer from the most common form of tachyarrhythmia - atrial fibrillation or atrial fibrillation. Along with the need for frequent hospitalization, emergency calls, a sharp decline in the quality of life and the development of ischemic strokes in at least 40,000 patients a year, the state spends huge amounts of money without returning these patients to a socially active lifestyle.
After 60 years of life, up to 6% of the population suffers from this disease and despite the constant use of antiarrhythmic drugs and blood-thinning anticoagulants - 50-60% of patients remain symptomatic and the “sword of Dodocles” hangs over them - either sudden death or disability, progressively increasing from the moment onset of the disease.
Today, cardiologists and cardiac surgeons, or rather specialists in the field of interventional arrhythmology, have found a new approach to diagnosis (also called electrophysiological) and elimination of the so-called paroxysmal and early persistent form of atrial fibrillation, when arrhythmogenic foci that trigger the arrhythmia are localized in the vessels flowing into the left atrium . Using various systems of electrophysiological diagnostics, using catheter technology (without a scalpel), specialists from the City Clinical Hospital named after. I.V. Davydovsky perform these procedures in previously incurable patients who have suffered from this arrhythmia for decades.
Currently, we are only at the beginning of the use of modern technologies for diagnosing and treating heart diseases and arrhythmias using so-called “bloodless surgery”, which does not require incisions.
Preparing for surgery:
includes a full diagnostic examination of the patient - ECG, echocardiography, Holter monitoring, blood tests. It is very important that the patient receives anticoagulant therapy (warfarin, Eliquis, Pradaxa or Xarelto) at least 3-4 weeks before surgery, since the operation will be performed in the “arterial chamber” of the heart. All medications the patient receives are discontinued in the clinic by the attending physician. At the clinic, the patient undergoes computed tomography and/or transesophageal echocardiography to exclude a “thrombus in the left atrial appendage. The presence of a blood clot is an “absolute” contraindication to surgical interventions and requires a change in anticoagulant therapy.
The procedure is performed through venous access (femoral, subclavian, jugular veins). Diagnostic electrodes are inserted into the region of the coronary sinus and a long introducer into the cavity of the right atrium. Under the control of X-ray, transesophageal or intracardiac echocardiography, a puncture of the interatrial septum is performed and instruments are passed into the cavity of the left atrium.
Depending on the anatomy of the left atrium, either Radiofrequency or Cryo-isolation of the pulmonary veins (PV) is performed. At the moment, the methods show equal effectiveness. The choice of PV isolation technique occurs before or during the procedure. If the patient underwent computed tomography before the operation, the anatomy of the left atrium and pulmonary veins allows you to select the desired technique (if TEE is performed before surgery, angiography of the left atrium is performed during the operation).
- if the left atrium is not enlarged in size and the pulmonary veins flow into the left atrium with separate orifices, the choice falls on cryo-isolation;
— if the atrium is enlarged or the PVs have a “collector” or “vestibular” entrance, or the size of the pulmonary veins is more than 25 mm (cryoballoon size 28 mm), we choose the radiofrequency isolation technique.
The operation is performed under intravenous anesthesia (propafol, fentanyl), the patient is completely awake, but does not experience pain. All pulmonary veins are sequentially isolated (cryo- or radiofrequency destruction), the effectiveness of electrical isolation is checked, and a repeat electrophysiological study is performed.
After the procedure is completed, the administration of anesthetic drugs ends, and the patient is transferred for 5-6 hours (sometimes longer) to the intensive care unit, where he is monitored. Then a control echocardiogram is performed and the patient is transferred to the ward under the supervision of the attending doctor. Another day of observation is carried out, antiarrhythmic and anticoagulant therapy is selected - then the patient is discharged. The patient is in the hospital for 3-4 days from the start of hospitalization. Changes in the length of hospitalization depend on the orders of the treating cardiologist. In the postoperative period, episodes of chest pain, dizziness, interruptions in heart function and attacks of arrhythmia associated with the operation (edema) may occur, which are not signs of a “relapse” of arrhythmia.
This is followed by a 3-month “blind period”, when the formation and normalization of the “isolation line” occurs. This is a period of rehabilitation and, during this time, additional interventions in the heart are not performed. Efficacy is assessed after this period and after discontinuation or reduction of dosages of antiarrhythmic drugs.
The overall effectiveness of primary procedures for isolating the pulmonary veins in paroxysmal forms of atrial fibrillation is 65-70%. This is due to restoration of conduction in isolated structures, other arrhythmias, progression of the disease, etc. Therefore, some patients (up to 50%) require a repeat procedure to identify and eliminate conduction breakthroughs in the pulmonary veins or concomitant “extrapulmonary” arrhythmias. The effectiveness of secondary surgery and improvement in quality of life is achieved in 90% of patients. It is advisable to carry out cardiac monitoring 3, 6 months and 1 year after the last operation. Cancellation of medications is carried out only with the consent of the treating doctor. Often, anticoagulant (thinning) therapy remains for long-term use and does not depend on the results of the operation (calculated using a specific CHADS2-VASc scale).
The number of complications in the City Clinical Hospital named after. I.V. Davydovsky is less than 1% and includes hemopericardium (accumulation of fluid in the heart sac), hematomas in the puncture area, phrenic nerve paresis (only during cryo-procedures). All complications are effectively managed during the hospital period and may lead to a delay in discharge. There were no deaths observed in our clinic.
Atrial flutter
The goals of management of patients with atrial flutter (AFL) are similar to the management of AF. Based on available data, the risk of stroke in patients with atrial flutter is not significantly different from that in AF. In addition, many patients with atrial flutter have concomitant AF (with this combination, the procedure is performed together). Thus, in patients with atrial flutter, anticoagulant therapy should be used in the same way as in patients with AF. Frequency control in AFL is achieved with the same drugs as in AF, but higher doses of drugs are usually required. Typical forms of AFL have a similar mechanism and “spin” around the tricuspid valve clockwise and counterclockwise.
In order to effectively eliminate this arrhythmia, it is necessary to draw a “demarcation” ablation line in the “narrowest” and “slowest” place of the tachycardia circle - the cava-tricuspid isthmus (from the tricuspid valve to the inferior vena cava).
Ablation of the cava-tricuspid isthmus in isthmus-dependent AFL effectively preserves sinus rhythm with an efficiency of 90-95%. The procedure, as with AF, is performed under intravenous anesthesia, transvenous access (femoral, subclavian, jugular veins).
This procedure is effective in reducing recurrences of AF in selected patients and will help avoid unnecessary hospitalizations. Isthmus ablation is a relatively safe and more effective method than antiarrhythmic drug therapy and is recommended for recurrent atrial flutter. Catheter ablation of left atrial macro-reentry tachycardia is a more complex procedure, with a lower success rate and a high rate of postoperative relapse.
Arrhythmology Center in Moscow
Arrhythmia may not have obvious clinical manifestations. The appearance of symptoms can be triggered by excessive mental and physical activity, previous illnesses, or taking medications. The first attacks of arrhythmia can pass quickly, and a person may not pay attention to them. But in the future, the frequency of attacks may become more frequent; if you do not pay attention to the symptoms, this may lead to the development of life-threatening complications, such as stroke, heart failure, sudden cardiac arrest. Most often, the first signs of arrhythmia are slow or irregular heartbeats, pauses between heartbeats. Also, some people notice a rapid heartbeat with periodic skipping of a heartbeat.
More serious complications include:
- anxiety,
- blurred vision,
- chest pain,
- labored breathing,
- fainting,
- fatigue,
- confusion of thinking,
- increased sweating,
- weakness, dizziness.
Arrhythmias that go unrecognized or go untreated can sometimes cause life-threatening complications affecting the heart and brain.
After analyzing the studies, it was found that cognitive impairment, Alzheimer's disease and vascular dementia are more common in people with arrhythmia. Which was associated with a decrease in blood supply to the brain over a long period of time.
Frequent attacks of arrhythmia provoke a decrease in the contractile function of the heart and can cause heart failure. Another complication of arrhythmia is stroke. This may occur in patients suffering from atrial fibrillation. With arrhythmia, blood can stagnate in the parietal areas of the atria, which can trigger the formation of blood clots. If the clot is poorly attached to the wall of the atrium, it can break off and travel through the bloodstream to the brain.
Cardiac activity can suddenly stop as a result of the development of a condition such as ventricular fibrillation.
Sudden infant death syndrome (SIDS) can be attributed to a hereditary heart disorder caused by arrhythmia.
If you or your loved ones have an increased risk of developing arrhythmia, at the Yusupov Hospital, Cardiology, based on your complaints, they will select an individual examination for you, which will allow you to accurately establish a diagnosis and select treatment.
Cardiac arrhythmia - causes
Depending on the cause and mechanism of development, all arrhythmias are usually divided into two large groups: organic and functional.
Organic . Associated with heart disease and often accompany atrial fibrillation, coronary heart disease (CHD), myocarditis, cardiomyopathy, cardiac malformations and injuries. Most often, organic disorders cause atrial fibrillation. They often occur after cardiac surgery as a complication. The pathology is based on organic damage to the heart muscle, which impedes the passage of an electrical impulse through the conduction system of the heart.
Functional . There are several types:
- Neurogenic . Associated with nervous system disorders. They arise due to severe stress, excessive emotions, intense physical and mental stress, smoking, drinking alcohol, strong coffee and tea, and spicy foods. They can be caused by thyroid diseases, intoxication, fever, infection (microorganism toxins), hypoxia and blood diseases. They often appear in women suffering from premenstrual syndrome (PMS).
- Diselectrolyte . They occur when there is an imbalance in the water-electrolyte balance. They are especially often observed in case of failures in magnesium, potassium, sodium and calcium metabolism.
- Iatrogenic . This type of arrhythmia is caused by taking medications that have an arrhythmogenic effect, in particular cardiac glycosides, sympathomimetics, diuretics, beta-blockers.
- Mechanical . They develop as a result of chest injury from a fall, blow, electric shock, etc.
- Idiopathic . These are all cases of arrhythmias, the cause of which has not been established.
In some cases, hereditary predisposition may play a leading role in the development of the disease.